
Abstract
Background:
Inflammatory bowel diseases (IBDs) have a peak incidence between the second and fourth decades of life and can affect women’s reproductive life.
Objectives:
Our study aimed to assess the impact of IBD on the reproductive life of female patients with this condition.
Design:
Cross-sectional study.
Methods:
Women with IBD followed at our IBD Unit and a group of healthy controls were enrolled. Data on reproductive life were collected using a dedicated questionnaire.
Results:
The study included 457 women, of whom 228 had IBD, and 229 age-matched healthy controls. No differences were found in the use of contraceptives, infertility, and endometriosis. The risk of spontaneous and voluntary abortions was significantly higher in IBD patients than in healthy controls [odds ratio (OR) 2 and 3.62, respectively]. The risk of obstetrical complications in the IBD population was more than six times higher in patients who experienced disease reactivations during pregnancy than in those with persistent remission [OR 6.9, 95% confidence interval (CI) 1.51–31.28]. Finally, we found that the chances of breastfeeding were 66% lower in patients with IBD than in controls (OR 0.44, 95% CI 0.22–0.91).
Conclusion:
Our study underlines the negative impact of IBD on women’s reproductive life, supporting the need for proactive preconception counseling.
Plain language summary
Summarise the established knowledge on this subject
Most women with Inflammatory Bowel Diseases are affected during their reproductive years. Women with IBD have fear, uncertainty, and poor knowledge of how the disease can impact their reproductive life. What are the significant and/or new findings of this study? Higher prevalence of abortions in women with IBD. Confirmed adverse pregnancy outcomes in the case of IBD activity. A lower chance of breastfeeding in women with IBD. Pro-active counselling is needed, which start from the moment of conception choice, with correct management of the pathology.
Introduction
Since the middle of the 20th century, the incidence of inflammatory bowel disease (IBD), namely Crohn’s disease (CD) and ulcerative colitis (UC), has increased in the Western world. The sex ratio of the incidence of CD changed from a male predominance in mid–late childhood and early adolescence (ages 5–14 years) to a higher incidence in women after that, with a complete reverse of the sex ratio to female predominance after age 25 until 75. 1 Instead, the incidence of UC did not differ significantly for female versus male patients (except for the age group of 5–9 years) until age 45 years; then, men had a significantly higher incidence of UC than women. Therefore, most women with IBD are affected during their reproductive years, with fear, uncertainty, and poor knowledge of how the disease can impact their life.2,3 The current literature reports that IBD women experience an higher prevalence of voluntary childlessness,4–6 drug interruption immediately before or during pregnancy,7,8 and a lower rate of breastfeeding compared to healthy women. 9
Recently, the European Crohn’s and Colitis Organisation (ECCO) guidelines on sexuality, fertility, pregnancy, and lactation have been published to properly monitor and treat both conditions and to support doctors in managing patients in these critical stages of their life. 10 Therefore, preconception counseling (PCC) has assumed an increasingly important role over time, with the aim of correctly educating patients, guiding them in their choices, and reassuring them about any concerns regarding the effects of the disease on fertility, and the safety of drugs during the gestational and lactation period of gestation and lactation.11,12
Our study aimed to assess the impact of IBD on the reproductive life of female patients with this condition, particularly regarding fertility, adverse pregnancy outcomes, childbirth, and lactation, considering the perceived influence of pharmacological therapy and the disease activity.
Materials and methods
We conducted a cross-sectional study in IBD patients included in the registry ‘The Paduan Gastrointestinal Disease Natural History Registry: a longitudinal, retrospective and prospective study’ (CESC code: 5370/AO/22) approved by the Ethical Committees of the Padova University Hospital. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution’s human research committee. Moreover, the study has been conducted following the STROBE guidelines.
For the scope of this study, we selected all female patients with IBD aged 18–65 years followed in our center and included in our database. From February to August 2022, these female patients were asked to complete a dedicated questionnaire during their routine follow-up visit. In the same period, healthy women of the same age were recruited among staff, familiars, and friends. Data were collected, anonymized, and aggregated in a dedicated database. The inclusion criteria were: female sex; age between 18 and 65 years; the presence of a confirmed IBD diagnosis (CD, UC, or IBD-Unclassified) from at least 1 year; and absence of IBD or any other gastrointestinal disorders in females enrolled in the control group. The response to the questionnaire was voluntary, and subjects could quit the questionnaire at any time. First, we performed a pilot test of 10 women to assess survey content and duration; no significant changes were needed based on this pilot testing.
Briefly, the questionnaire was divided in 2 parts: the first part, composed of 25 questions, dedicated to demographic data (age in menarche and number of children), presence of current or past endometriosis, presence, reasons, and duration of current or past hormonal therapy, presence of current or past infertility (defined as failure to conceive after 1 year of unprotected sex), history of spontaneous of voluntarily abortions, and age at first pregnancy if any. The second part was dedicated to those who had experienced at least 1 pregnancy (45 questions for each pregnancy). We collected data on in vitro fertilization, any surgery before conception, way of delivery (natural or cesarean delivery), and any obstetrical complications [eclampsia, Hemolysis, Elevated Liver enzymes and Low Platelets (HELLP) syndrome, low weight for gestational age, gestational diabetes, and oligohydramnios] were collected. The questionnaire also asked about IBD therapy before and during pregnancy and any change, suspension, and resumption during pregnancy and disease reactivations. Finally, data about children and any child infection during their first year of life, and information about breastfeeding such as duration and reason behind any failure to breast were also collected.
Statistical analysis
Results were summarized as frequencies and percentages (categorical variables) and as means with standard deviations (SDs, continuous variables). Categorical variables were compared with the χ2 test, while continuous variables were compared using the Student’s t test. Logistic regression was used to analyze the risk of having specific outcomes in IBD compared to controls, expressing as odds ratio (OR) and 95% confidence intervals (CIs). The statistical significance was set at 0.05. Data were analyzed using STATA11 software (Stata Corp., College Station, TX, USA).
Results
At the beginning of the study, 721 IBD women aged 18–65 years with an IBD diagnosis from at least 1 year were included in our registry. All of them were asked to complete the questionnaire, and 228 agreed to participate (31.6% of the response rate), with the main reason for nonresponse as the lack of time or unwillingness to respond. No questionnaire was incomplete. Among the 228 patients, 127 had CD (56%) and 101 UC (44%). Healthy controls enrolled were 229. Table 1 summarizes the primary demographic and clinical characteristics of our population. The most common comorbidities were a rheumatological autoimmune disease, found in 18.9% (43/228) patients (21.3% for CD, and 14.9% for UC) and only in 2.2% (5/229) controls (p < 0.001) (Table 1).
Demographic and clinical characteristics of IBD cases and controls, with differentiation between CD and UC.
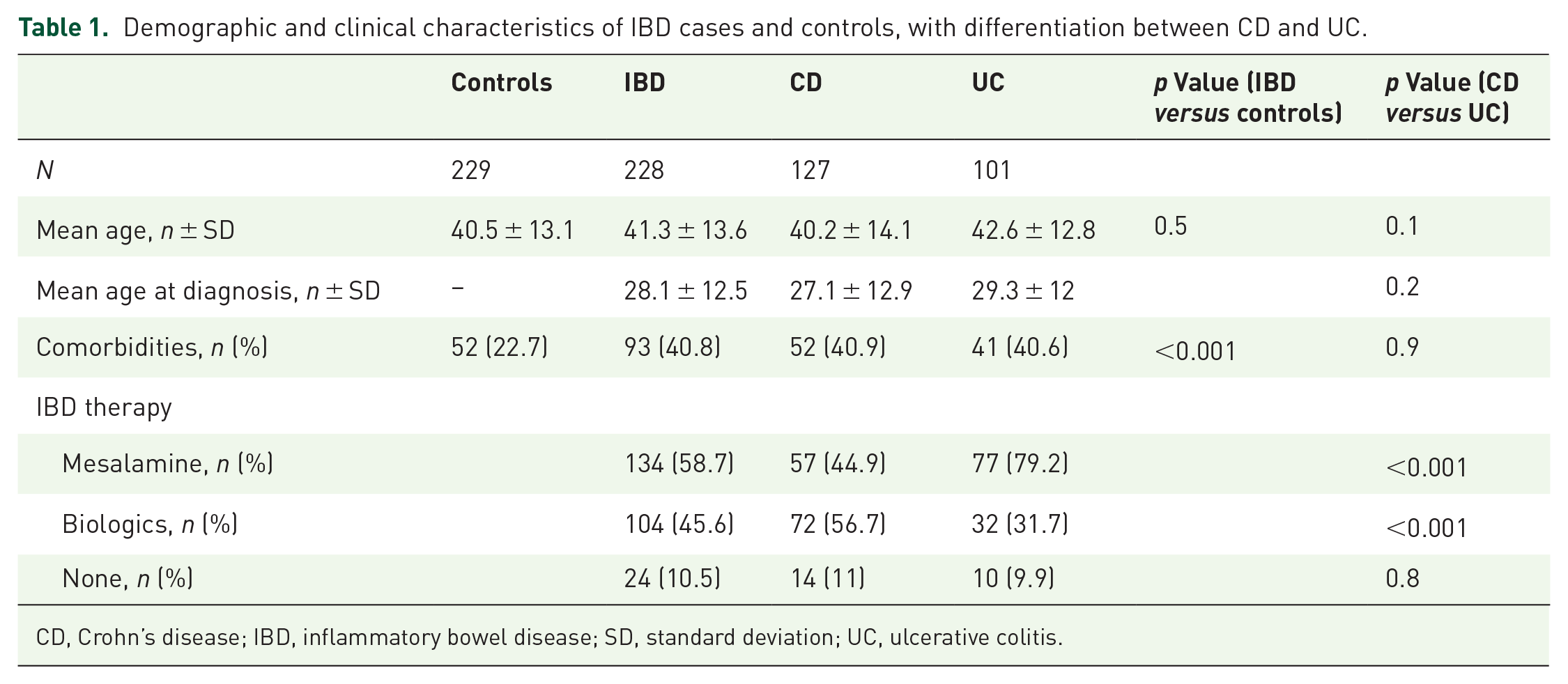
CD, Crohn’s disease; IBD, inflammatory bowel disease; SD, standard deviation; UC, ulcerative colitis.
At the time of the questionnaire, the most used drugs were mesalamine (58.7%) and biologic drugs (45.6%), with a significant difference between CD and UC (Table 1); 10.5% of the patients did not take specific therapy.
The use of oral estrogen-progestogen or only progestogen pills was similar between IBD female patients and healthy controls (OR 0.99, 95% CI 0.68–1.43). However, a different reason for hormone replacement therapy (HRT) was provided by the two groups (p = 0.003): 52.5% (64/122) of IBD female patients took HRT for menstrual cycle disorders, 60.5% (75/124) of the healthy controls took it for contraceptive purposes. No difference in HRT intake was found between patients with CD and UC (p = 0.7). We did not observe significant differences in the incidence of infertility between the two groups (OR 1.76, 95% CI 0.78–3.94). Furthermore, none of the 10 patients who underwent bowel resection or stricturoplasty surgery had infertility problems. No increased rate of endometriosis was found in the group of women with IBD (OR 1.39, 95% CI 0.63–3.10) (Table 2). We separately considered the risk of spontaneous and voluntary termination of pregnancy (VTP), finding that female patients with IBD had a double risk of spontaneous abortion (OR 2, 95% CI 1.05–3.83) and 3.62 times risk of having a VTP (OR 3.62, 95% CI 1.41–9.2). However, 10 female patients had a spontaneous abortion before diagnosis and 18 after diagnosis; thus, comparing the number of spontaneous abortions in controls with IBD patients after diagnosis (7.2% versus 7.9%, p = 0.1), no difference was observed. Similarly, 10 female IBD patients underwent a voluntary abortion before the IBD diagnosis, 6 after, and 3 both before and after the IBD diagnosis. No difference in the risk of abortion was found between CD and UC.
Study outcomes in the overall population (229 controls, 228 IBD patients).

Ten before IBD diagnosis and 18 after IBD diagnosis.
Ten before IBD diagnosis, six after IBD diagnosis, and three both before and after. Maximum number of voluntary abortions six in IBD patients and three in controls.
CI, confidence interval; IBD, inflammatory bowel disease; OR, odds ratio.
Pregnancy and puerperium
Regarding the number of pregnancies, in our population, 26.8% (61/228) of female patients with IBD had at least one pregnancy after IBD diagnosis and 51.1% (117/229) among controls. Moreover, 13.2% (30/228) IBD cases and 24.5% (56/229) controls had a second pregnancy. For this study, we only considered the first pregnancy. Data showed that women with IBD had a higher mean age at the first pregnancy (31.6 ± 5.4 years) compared to the control group (29.8 ± 4.3 years, p = 0.02), with a mean age of 30.6 ± 5.5 in the CD group and 33 ± 5.1 in the UC group. At the beginning of their pregnancy, 94.3% (33/35) of female CD patients and 84.6% (22/26) of UC were in clinical disease remission. During pregnancy, the most used drug was mesalamine in monotherapy as oral intake (30/61, 49.2%), while 8.2% assumed the combination of oral mesalamine plus topical therapy (mesalamine or steroid). Seven patients (11.5%) took biologics, while 16.4% interrupted their therapies at the beginning of the pregnancy (four were taking an immunosuppressor). The rest of the patients had no therapy. Thirteen patients (21.3%) experienced a disease reactivation during pregnancy (only three were active at conception); one was on biological therapy, and the others were taking mesalamine. Disease reactivations were mainly treated with oral steroids (53.8%) and the remaining ones with oral mesalamine or topical therapy optimization. No reactivation was treated with biologics.
Obstetrical complications related to pregnancy had a similar risk in the two groups (OR 1.09, 95% CI 0.45–2.64) without difference between CD and UC patients (p = 0.11) (Table 3). However, the risk of complications in the IBD population was more than six times higher in patients who experienced disease reactivations during pregnancy than those with persistent remission (OR 6.9, 95% CI 1.51–31.28).
Study outcomes at the first pregnancy (117 controls, 61 IBD patients).

CI, confidence interval; IBD, inflammatory bowel disease; OR, odds ratio.
Additionally, we did not observe any difference in the risk of cesarean delivery between IBD and controls (OR 1.54, 95% CI 0.81–2.92). However, we found differences in the reasons for the cesarean section (p = 0.34): 19.2% of IBD cases underwent cesarean section due to fetal problems, compared to 29% (11/38) of controls and 19.2% due to previous surgery compared to only 2.6% (1/38) of controls. Other less frequent reasons included insufficient vaginal dilatation, use of medical advice, and twin pregnancy.
We observed that after the first pregnancy, the chances of breastfeeding were 66% lower in patients with IBD than in controls (OR 0.44, 95% CI 0.22–0.91). In the group of women with IBD, 13.1% did not breastfeed for personal choice, compared to 3.4% in the control group, while 11.5% (7/61) did not breastfeed due to lack of milk, similar to healthy women (11.1%, 13/117). About 84% of patients who did not breastfeed took mesalamine as monotherapy.
Furthermore, 37.7% of women with IBD (13/35, 37.1% in CD and 10/26, 38.5% in UC) had a disease relapse after their first pregnancy, within 12 months of delivery, and biologic drugs were adopted in 21.7% for these disease reactivations.
Discussion
IBDs are chronic progressive immune-mediated diseases characterized by uncontrolled inflammation of the gastrointestinal tract. Their impact on daily life, particularly on the reproductive life of affected women, is considerable.2,3 Therefore, our study aimed to analyze a cohort of patients with IBD to understand how these diseases impact women’s reproductive health using a group of healthy women as a comparator.
Consistent with what is reported in the literature, we found a high incidence of IBD between the second and fourth decades of life (mean age at diagnosis 28.1 ± 12.5 years old) and a considerable increase in extraintestinal manifestations of rheumatologic nature compared to the general population: 18.9% versus 2.2%.13,14
Similar rates of endometriosis were found in our patients and controls. These data are in disagreement with Chiaffarino et al., 15 who reported in a systematic review a rate of endometriosis from 2% to 3.4 % in IBD patients, while between 0% and 1% among control subjects. Similarly, a large Danish cohort study reported that women with endometriosis had an increased risk of CD and UC with a standardized incidence ratio of 1.5 (95% CI 1.3–1.7) and 1.6 (95% CI 1.3–2.0), respectively. 16
Regarding the reproductive sphere, our data did not show difference between the risk of infertility in women with IBD and healthy subjects. This is in line with what is reported in medical literature, where infertility in IBD had a prevalence similar to that of the general population, particularly in patients with an inactive disease or who have never undergone surgery.5,17 Instead, surgery may have a significant impact on fertility, mainly through adhesions or abdominal/pelvic organs damage; a meta-analysis published in 2006 suggested that the rate of infertility was 48% in UC patients with ileal pouch-anal anastomosis, with a risk three times greater than people treated with medical therapy. 18 In our population, none of the patients who underwent surgery for IBD were affected by infertility.
From our population emerged a similar rate of oral contraceptive use than in healthy controls, but with a different reason for starting this therapy between the two groups (p = 0.003): women with IBD took EP mainly for menstrual cycle disorders, whereas healthy subjects took it mainly (60.5%) for contraceptive purposes. In medical literature, there are less conflicting data on the use of EP in women with IBD. Ban et al. showed higher use of contraceptives in female patients with IBD than in healthy controls. However, distinction in the use of the different available contraceptives (oral contraceptives, intrauterine devices, barrier method, etc.) was not made, and the reason for their administration was not specified. 6 Because our IBD population primarily takes EP for menstrual disorders, our results support the limited literature evidence that, in addition to pregnancy planning or gynecological disorders, hormonal contraception may improve overall satisfaction with intestinal symptoms control. 19
Taking into account the number of pregnancies in the two groups, we did not find significant differences between female patients with IBD and healthy women. Likewise, we did not find significant differences between female patients with IBD and healthy women regarding the occurrence of complications during pregnancy. 20 However, we observed a sixfold higher risk of complications in patients with active disease than in women in disease remission, similar to those reported in the literature. 21 The disease reactivation during pregnancy was unrelated to the active state at conception, conversely to those reported in the literature. 22
Regarding the frequency of abortions, we have recorded that this is significantly increased in women with IBD, both considering spontaneous and VTP. There are limited studies about this topic; a Danish cohort study by Nørgård et al. 23 reported that pregnant female patients with IBD are not more likely to choose an elective abortion compared with the general population. Regarding the rate of cesarean deliveries, we did not find a difference between patients and controls. The last guidelines 10 report that the literature does not support a specific preference for cesarean section over vaginal delivery in patients with IBD regarding damage of the anal sphincter in the case of restorative proctocolectomy or development of de novo perianal disease. Therefore, the mode of delivery for these patients should be taken case by case by a multidisciplinary team.
In confirmation of what was highlighted by Selinger et al., 24 women with IBD in our cohort breastfeed less frequently than healthy women, primarily for personal choice or for fear that the therapy could affect the children’s health (13.1% versus 3.4%). However, most of these patients were taking mesalamine, which is allowed during breastfeeding by both international guidelines and medical agencies.
Limitations
It must be emphasized that our study has limitations: first, since it was a single-center study, the number pool of patients recruited was limited, especially those with at least one pregnancy. All data come from self-reported patient answers, which could lead to a potential recall bias; however, we believe that pregnancy is such an essential moment in a woman’s life that the recall bias is reduced. Moreover, as it is a cross-sectional survey and patient reported outcomes, you are not able to accurately assess the IBD disease activity at the time of conception or pregnancy. Finally, we observed that the CI of the risk for adverse pregnancy outcomes in active IBD is very wide. This may be due to the low number of events in this subgroup of patients (active versus remission).
Conclusion
In conclusion, our study underlines the negative impact of IBD on women’s reproductive life, particularly with respect to the risk of complications in cases of disease activity and the decision not to have breastfeeding. Our data reinforce the importance of adequate counseling, as suggested by recent guidelines, 10 through support that starts from the moment of conception choice. This will allow better management of the disease and will reduce the impact of IBD on daily life of IBD women.
In our center, we have not yet developed a schematized and standardized way of PCC: we need to proactively address the issue with our patients, while, for now, we limit ourselves to answering any questions from the patient about pregnancy, lactation, or others, during the routine visit. Therefore, the future goal could be to integrate proactive PCC into standard clinical practice to convey the correct information to patients, improve pregnancy outcomes, and optimize disease management at this stage of their lives.