
Abstract
Background:
Videocapsule endoscopy (VCE) and double-balloon enteroscopy (DBE) are part of the diagnostic and therapeutic work-up of indications other than suspected small bowel bleeding (OSBB). The literature is currently lacking studies describing these procedures in this particular setting.
Objectives:
We assessed the clinical impact of VCE and DBE in a large monocentric cohort of OSBB patients, as compared to a control group of suspected small bowel bleeding (SSBB) patients who underwent enteroscopy over the same period.
Design:
Monocentric, retrospective, cohort study.
Methods:
We collected the data of consecutive patients with OSBB undergoing VCE and/or DBE from March 2001 to July 2020. The demographic and clinical parameters of the patients, technical characteristics, and adverse events for each procedure were collected. The impact of VCE and DBE was defined in terms of diagnostic yield (DY). The patients were subdivided according to the main indication into four groups: celiac disease, Crohn’s disease (CD), neoplasia, and persistent gastrointestinal symptoms.
Results:
A total of 611 VCEs and 387 DBEs were performed for OSBB. The main indications were complicated celiac disease and CD. The DYs of VCE and DBE overall were 53 and 61.7%, respectively, with some variance among the four groups. We report no statistical differences in the DY of VCE and DBE in SSBB vs OSBB (57.7% vs 53%, p = 0.0859 and 68.8% vs 61.7%, p = 0.0582, respectively). OSBB patients were significantly younger than those with SSBB. However, similarly to SSBB (k = 0.059), poor agreement between the enteroscopic techniques was found in the OSBB population (k = 0.109). The safety of both procedures in OSBB was comparable to that in SSBB patients.
Conclusion:
VCE and DBE are effective and safe in suspected OSBB, where their role is similar to that in SSBB, their main indication.
Keywords
Introduction
In the last two decades, videocapsule endoscopy (VCE) 1 and device-assisted enteroscopy (DAE), most commonly double-balloon enteroscopy (DBE),2–4 have emerged as reference standards for the diagnosis and endoscopic treatment of small bowel (SB) diseases.
Their main indication is suspected SB bleeding (SSBB), 4 but in recent years indications other than SSBB (OSBB) have emerged and are gaining importance.4–6 Among OSBB indications, the most important are the diagnosis and follow-up of complicated celiac disease (CeD), malabsorption, and SB Crohn’s disease (CD). Moreover, VCE and DAE are used to investigate inherited polyposis syndromes, allowing detection, diagnosis, and various therapeutic approaches.7,8
VCE is a diagnostic tool, while DAE allows a wide range of therapeutic interventions, which include tissue sampling, polypectomy, hemostasis with argon plasma coagulation or hemostatic endoclips, tattooing (prior to surgery or for endoscopic reference), endoscopic mucosal resection, retrieval of foreign bodies, enteral stricture dilation, the placement of jejunal feeding tubes, the treatment of early postoperative SB obstruction, and the performance of endoscopic retrograde cholangio-pancreatography in patients with postsurgical anatomy.9–14
In OSBB, VCE and DBE show comparable diagnostic yields (DYs) of 16% and 18%, respectively, for inflammatory lesions, and 11% for both suspected SB neoplasm and polyps. 15 Interestingly, when performed in patients with a positive VCE result, DBE DY is significantly higher; however, it should be kept in mind that these data refer to studies investigating obscure gastrointestinal bleeding. 16
Several studies in the literature have described the diagnostic role of DAE and VCE in SSBB, yet only a few have focused on OSBB. The aim of our study is to evaluate the clinical efficacy of VCE and DBE in terms of their DY in OSBB by investigating a large monocentric cohort of patients recruited over a long period.
Patients and methods
We retrospectively enrolled all consecutive patients referred to the Gastroenterology and Endoscopy Unit of Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico (Milan, Italy), who underwent VCE and/or DBE from 1 March 2001 to 31 July 2020. Both adult and pediatric patients were included in the study. The following clinical data were collected for each patient: sex, date of birth, age at the time of the procedure, comorbidities, and number of VCEs and/or DBEs undergone.
Videocapsule enteroscopy
Different types of capsules were used from 2001 to 2020, such as M2A, M2A Plus, SB2, SB3, PillCam COLON 2, and PillCam Crohn’s capsule. All examinations were performed after bowel preparation, which consisted of the intake of a 2-l polyethylene-glycol-based solution on the day before the procedure and overnight fasting.
The Given/Medtronic imaging recording system was positioned according to the manufacturers’ instructions; data were downloaded on a dedicated computer workstation and were analyzed with dedicated software. A patency capsule test was performed prior to VCE, according to guideline indications, for instance in the event of obstructive or sub-obstructive symptoms and/or previous SB surgery. 4 Each examination lasted at least 9 h, in accordance with the manufacturer’s specifications, and was conducted until battery exhaustion. The VCE imaging results were defined according to the adequacy of mucosal visibility: from 2001 to 2019, visibility was rated as optimal, good, sufficient, or poor. Mucosal visibility was then defined as adequate if optimal or good, and inadequate in all other cases. Since 2020, the Small Bowel Mucosal Visibility Scoring System 17 was used.
For each VCE, the following data were recorded: indication, type of capsule, completion rate, gastric and SB transit times, SB cleansing, and endoscopic findings (type and location of the lesions along SB tertiles).
Device-assisted enteroscopy
DBE was the type of DAE employed. DBEs were performed with Fujifilm (Fujinon, Saitama, Japan) equipment, and three types of enteroscope were used: standard (EN-580T), short (EI-580BT), and slim (EN-450P5 and then EN-580XP). The route of insertion was established according to the localization of the target lesion on VCE or other imaging techniques or based on clinical presentation. Preparation for the oral route procedure consisted of patients fasting for 6–8 h prior to examination; for the anal route, every patient followed an intestinal preparation protocol similar to that for colonoscopy and fasted for 6–8 h before examination. DBE was performed under conscious sedation. In the presence of significant comorbidities defined as an ASA score ⩾3, in pediatric patients, or in procedures considered to have a high risk of complications (e.g., polypectomy, endoscopic mucosal resection), DBE was performed with anesthetist support.
For each procedure the following data were recorded: indication, route of insertion, type of sedation, duration, depth, number of advancement steps, endoscopic findings (type and location in the gastrointestinal tract) and procedures, adverse events, and serum amylase and lipase levels.
DY and agreement between VCE and DBE
We defined the effectiveness of VCE and DBE in terms of DY, which indicates the ability to identify significant lesions and is calculated as the proportion of positive tests out of the total number of tests considered. Procedures were defined as positive when highly suggestive lesions, according to the indication, were found in any segment of the gastrointestinal tract.18,19 Highly suggestive lesions, based on the indication for enteroscopy, are reported in Supplemental File 1.
The safety of the procedures was analyzed in terms of the frequency of adverse events in all procedures according to the ASGE lexicon. 20
Agreement between the two procedures was determined by considering only cases in which VCE was followed by DBE for diagnostic or therapeutic purposes within 6 months. DBE was defined as the reference standard.
Statistical analysis
All statistical analyses were carried out with IBM SPSS Statistic (release 23; IBM, Armonk, New York, USA) and GraphPad Prism (release 6.0; GraphPad Software, San Diego, California, USA).
Data related to the patients’ clinical and demographic characteristics and findings on VCE and DBE were analyzed descriptively, producing sums and percentages for the categorical variables, median and interquartile range 25-75% (IQR, Q1-Q3) for continuous variables. Categorical variables were compared with Fisher’s exact test or with the χ2 or McNemar’s test, yielding the odds ratio (OR) and its confidence interval (95% CI). Values of p < 0.05 were considered statistically significant. Continuous variables were compared with Student’s t-test, in the case of normal distribution, and with the Kruskal–Wallis test or Mann–Whitney U test in the case of non-normal distribution. We matched each OSBB procedure with an SSBB procedure with a random forest distance measure methods considering patients’ age and sex.
The sensitivity, specificity, and likelihood ratio of VCE were calculated, considering DBE as the standard reference. Agreement between the two methods was obtained by calculating Cohen’s κ coefficient and its confidence interval; the agreement obtained was considered poor (k = 0.00–0.20), modest (k = 0.21–0.40), moderate (k = 0.41–0.60), good (k = 0.61–0.80), or almost perfect (k = 0.81–1.00).
The study was carried out in accordance with the Declaration of Helsinki, adopted in 1964 and incorporating all later amendments. All study participants gave their informed consent for data retrieval and endoscopic treatment. Their data were treated confidentially, in compliance with the most recent national and European privacy laws (protocol number 137/2021, Comitato Etico Milano Area 2). The reporting of this study conforms to the STROBE statement. 21
Results
Patient cohort
A total of 2212 procedures for any indication were performed in 1606 patients: 794 DBEs (592 patients) and 1418 VCEs (1200 patients). The population consisted of 749 (46.6%) males and 857 (53.4%) females. The median age at the time of enteroscopy was 67 years (interquartile range, IQR [Q1–Q3] 50–80), and 851 patients (52.4%) were over 65 years of age. The demographic characteristics of the cohort are described in Table 1.
Demographic characteristics of the population.

Median [Q1–Q3].
DBE, double-balloon enteroscopy; VCE, videocapsule endoscopy.
A total of 611 (43%) VCEs and 387 (49%) DBEs were performed for OSBB. Procedures were divided into groups based on their main indications and the results analyzed, for known, suspected, or refractory CeD (RCeD) (CeD group),22,23 diagnosis or follow-up of CD (CD group), suspected or known SB neoplasia (NeoPl group),24,25 and persistent gastrointestinal symptoms (Sympt group). Other minor indications are listed in Supplemental File 1.26–29 The distribution of the different indications are represented in Figure 1.

OSBB indication subtypes for VCE (a) and DBE (b).
VCE and DBE
The demographic and technical aspects of the enteroscopies are described in Table 2.
Demographic characteristics of patients and technical aspects of enteroscopies performed for OSBB compared with SSBB.

SSBB versus OSBB.
Hours:minutes.
Median [Q1–Q3].
From the pylorus in anterograde DBE and from the ileocecal valve in the retrograde DBE.
CD, Crohn’s disease; DBE, double-balloon enteroscopy; NA, not applicable; OSBB, other than small bowel bleeding; SB, small bowel; SSBB, suspected small bowel bleeding; VCE, videocapsule endoscopy.
The youngest patient who underwent VCE for OSBB was 10 years old, while the oldest was 85 years old. Among the four main groups, patients in the CD group undergoing either VCE or DBE were significantly younger than those in the CeD group (p < 0.001 and p < 0.031, respectively). There were significantly more women in the CeD group than in the NeoPl group undergoing either VCE (p = 0.002) or DBE (p = 0.048). There were no statistical differences in any of the demographic variables between patients from the CeD group and those with symptoms (p = 0.070).
In the VCE group, there were no adverse events or capsule retentions. Among patients who underwent DBE, only two adverse events occurred: one patient experienced mild pancreatitis and another patient developed Takotsubo syndrome 8 h after the procedure.
A total of 496 and 305 patients, respectively, underwent at least one VCE or DBE. Some of the patients underwent more than one procedure in the period considered. In particular, two patients repeated VCE seven times, and another two patients repeated it six times. These particular patients were affected by RCeD type 2 and were under long-term follow-up.30,31 Consequently, they required multiple evaluations of SB mucosa to monitor and adapt the therapeutic approach. The distributions are presented in Supplementary File 1.
Findings, DYs, and VCE–DBE agreement
Endoscopic findings for each procedure were recorded according to the subgroup. In the CeD group, the most common findings were atrophy (including mosaicism and scalloping), followed by ulcers both on VCE and DBE. In CD, aphthae and ulcers were the most common findings with both techniques. Interestingly, in the CD and NeoPl groups, a significantly higher rate of stenosis was detected on DBE compared with VCE (27.4% versus 6.7% in CD; 25% versus 2% in NeoPl). Lastly, in patients who underwent enteroscopy for persistent unexplained symptoms, the most common findings were polyps (28.6%) and aphthae (23.8%) on VCE, while atrophy (41.7%) and polyps (19.4%) were the predominant findings on DBE. The endoscopic findings of the main subgroups are reported in detail in Table 3 and endoscopic images are shown in Figure 2.
Endoscopic findings per category.

CD, Crohn’s disease; DBE, double-balloon enteroscopy; GI, gastrointestinal; VCE, videocapsule endoscopy.

Imaging findings in OSBB: voluminous neoformation (metastatic melanoma) protruding in the jejunal lumen, VCE (a) and DBE (b); severe atrophy, with scalloping and granular mucosa of the proximal jejunum in a patient with refractory celiac disease type II, VCE (c) and DBE (d); ulcerated stenosis at the distal ileum of a patient with known CD, VCE (e) and DBE (f).
Overall, the VCE DY in OSBB was 53%. Interestingly, a similar result was obtained for VCE performed for SSBB, with a DY of 57.7% (p = 0.0859). 32 When each subgroup is considered separately, the VCE DY was more heterogeneous, ranging from 62.3% in the NeoPl group and 56.9% in the CeD group, to 41.9 and 37.5% in the CD and Sympt groups, respectively. A statistical difference was observed between the DYs in the CeD and the CD groups (p = 0.0053), and between the NeoPl and the CD groups (p = 0.0140).
Regarding DBE, the overall DY obtained for OSBB was 61.7%, which was not statistically different to the DY of DBE for SSBB (68.8%; p = 0.0582). 32 On the other hand, the DBE DYs of each subgroup were not statistically different. Lastly, for each category, the DYs of VCE and DBE were compared (Tables 4 and 5).
DBE and VCE DYs in the different subgroups.

OSBB only includes data from celiac disease, Crohn’s disease, neoplasia, and symptoms.
CD, Crohn’s disease; DBE, double-balloon enteroscopy; DY, diagnostic yield; OSBB, other than small bowel bleeding; SSBB, suspected small bowel bleeding; VCE, videocapsule endoscopy.
Comparisons of DYs.
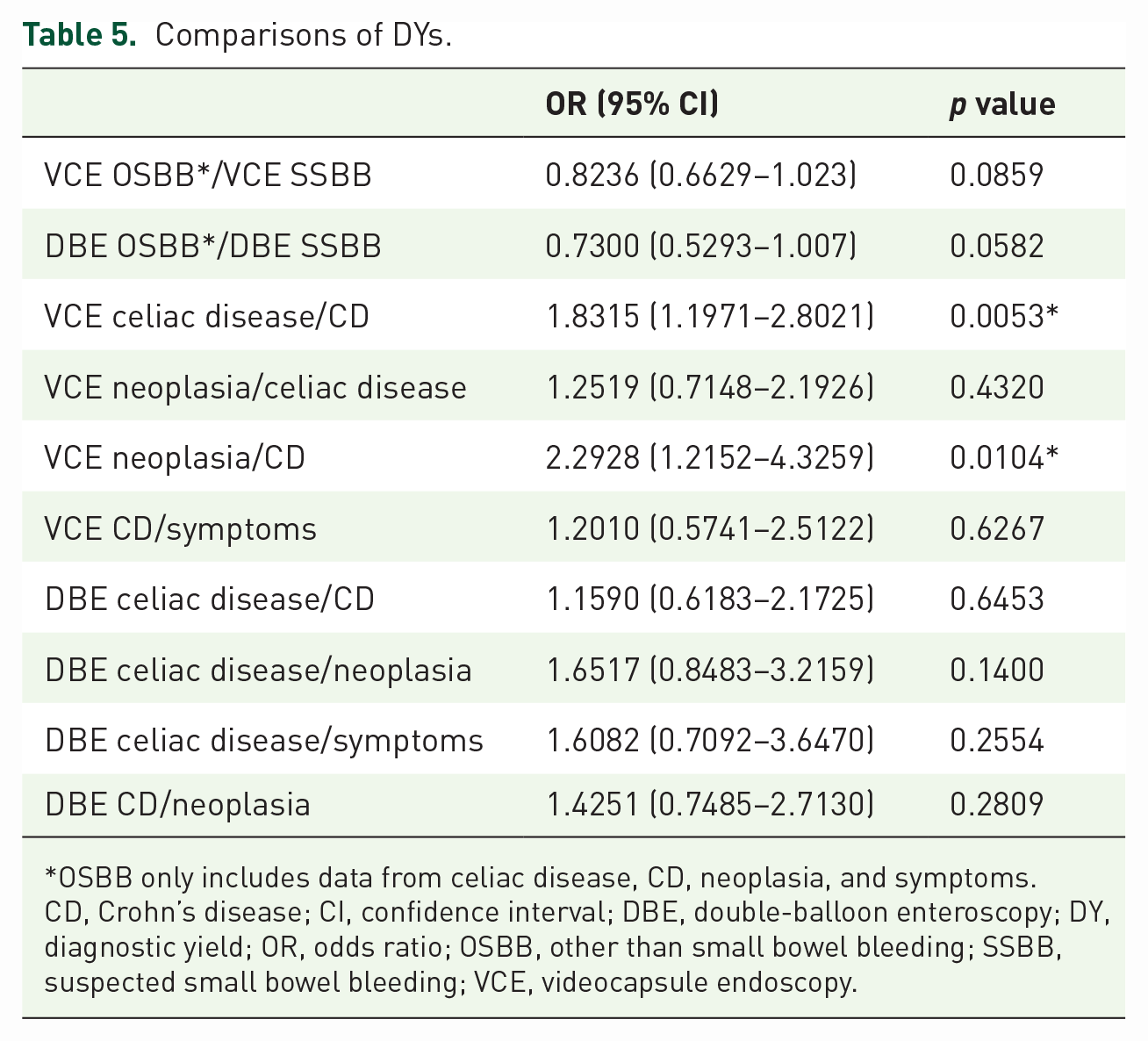
OSBB only includes data from celiac disease, CD, neoplasia, and symptoms.
CD, Crohn’s disease; CI, confidence interval; DBE, double-balloon enteroscopy; DY, diagnostic yield; OR, odds ratio; OSBB, other than small bowel bleeding; SSBB, suspected small bowel bleeding; VCE, videocapsule endoscopy.
Due to the demographic difference, in a sub-analysis, we sex-age matched OSBB patients according to the SSBB group. We obtained 212 VCEs and 157 DBEs. matched in a 1:1 ratio. Overall mean weighted distance of covariates after random forest matching was 0.083 (IQR −0.168– 0.539) for DBE and 0.085 (IQR −0.252–0.617) for VCE. The analyses show a comparable DY between the OSBB and SSBB procedures, for both VCEs and DBEs (79.6% vs 79.6% and 52% vs 59.9% for VCE and DBE respectively, with p values of 1 and 0.21, respectively).
A total of 119 patients with OSBB underwent both DBE and VCE: 55 patients in the CeD, 24 in the CD, 29 in the NeoPl, and 11 in the Sympt group. The agreement between VCE and DBE was calculated with Cohen’s κ coefficient, considering DBE as the reference standard (Table 6). Compared with SSBB (k = 0.059), poor agreement was found in the OSBB population (k = 0.109).
Sensitivity, specificity, likelihood ratio, and Cohen’s κ coefficient (95% CI), considering DBE as the reference standard

CD, Crohn’s disease; CI, confidence interval; LR, likelihood ratio; OSBB, other than small bowel bleeding; SSBB, suspected small bowel bleeding.
Discussion
For our cohort study, we enrolled the largest European case series of patients undergoing VCE and DBE for known or suspected SB disease without a bleeding indication.
Studies of SB endoscopy in this setting are lacking, with most of the published research focusing on enteroscopy in SSBB, which remains the main indication for enteroscopic procedures and accounts for 70% of the indications for VCE and DBE. 33 However, analysis of the data collected at our center reveals a significant difference: in our cohort, only 55% of VCEs and 52% of DBEs were performed for SSBB. This is because the Fondazione IRCCS Ca’ Granda Ospedale Policlinico is a regional reference center for many SB diseases (such as CD and CeD) and we recruited a large series of patients with indications other than SSBB.
We analyzed the demographic characteristics and endoscopic findings of those with known or suspected enteropathy without signs of bleeding who underwent VCE and/or DBE. Results were also stratified according to the main indication. Patients with SSBB who underwent enteroscopies during the same period served as the control group.
Moreover, due to the large sample size, we were able to perform a comparison analysis between VCE and DBE. To the best of our knowledge, this is the first such report in the literature.
Analysis of the demographic characteristics of our cohort indicates that among patients who underwent VCE, those with OSBB have a lower average age and are more commonly female compared with the SSBB group. Also, a higher proportion (53.8%) of the SSBB group are elderly (over 65 years of age) compared with the OSBB group (17.8%). This is consistent with the main indications for VCE and DBE. Our data show that chronic SB enteropathies occur on average at an earlier age than overt or occult bleeding of the SB and are more common in women.
The completion rate, gastric and intestinal transit time, and the frequency of adverse events are comparable and similar between the SSBB and OSBB groups.
The frequency of procedures with anesthetists support, the mean duration of procedures, the mean number of advances, and the depth reached in the SB did not differ between DBE performed for OSBB or for SSBB. The frequency of anterograde procedures was higher (3:1) for OSBB than for SSBB (5:1), although more retrograde procedures were performed in the OSBB population than in the SSBB group. A possible explanation is that in patients with known or suspected CD, more frequently represented in our OSBB group, the SB is usually investigated using the retrograde approach, since the terminal ileum and the ileocecal valve are the most commonly affected regions. 34
The rate of adverse events associated with DBE was 0.5% in the OSBB population, which was lower than in the SSBB population (1.5%). However, this difference is not statistically significant (p = 0.28), even though more endoscopic therapeutic interventions were performed in the SSBB group (48.4% versus 13.4%, p < 0.001; of note, biopsies and tattoos were excluded).
Additionally, the rate of adverse events observed in OSBB and SSBB combined was 1% for all procedures, and 0.8% for diagnostic DBEs and 8% for therapeutic DBEs. 4
A total of 559 VCEs were performed for OSBB with a DY of 53%, comparable with the DY of VCE for SSBB (57.7%, p = 0.086). The highest VCE DYs were obtained in the following three groups: 56.9% in CeD, 41.9% in CD, and 62.3% in patients with suspected SB neoplasia. Nevertheless, there is a significant difference between the DYs of VCE performed for CeD and that performed for CD [OR 1.831; 95% confidence interval (CI) 1.197–2.802; p = 0.005], as well as between that performed for suspected neoplasia and for CD (OR 2.293; 95% CI 1.215–4.326; p = 0.010).
Similarly to VCE, studies focused on the DY of DBE for these indications are lacking, despite the pivotal role of DBE in these settings. Indeed, DBE allows therapeutic procedures (e.g., polypectomy and stenosis dilation), biopsies, and tattoos to be performed. For example, DBE can make a definite (histological) diagnosis possible even in the absence of macroscopically observable mucosal lesions. This also applies in the case of suspected complicated CeD, where histology is decisive in confirming or excluding the diagnosis. Interestingly, the DY of DBE in patients with OSBB was comparable with that of patients with SSBB (61.7% versus 68.8%). In particular, although not statistically significant, our data show that DBE has a higher DY in the CeD (67.1%) and CD (63.7%) groups compared with the Sympt (55.9%) and NeoPl (55.2%) groups. After matching for age and sex, the DY of both VCE and DBE were comparable between the OSBB and the SSBB groups.
In the OSBB population, suboptimal agreement between the two procedures was observed (k = 0.109). Analysis of the four main subgroups showed comparable agreement, except for the NeoPl group, which had modest agreement (k = 0.313). Similar suboptimal agreement was found in the SSBB population (k = 0.059). Notably, agreement between the two modalities strongly depended on the time interval between VCE and DBE in the case of SSBB. In the case of OSBB, the time interval between VCE and DBE was greater on average than that for SSBB because it is rarely an emergency procedure. Moreover, in the setting of OSBB, reducing the time interval between the procedures did not impact agreement because non-bleeding lesions rarely self-resolve. Most importantly, in our center, DBEs are often also performed after a negative VCE because of significant clinical or radiological suspicion. This is also supported by the expertise of our tertiary center for DBE enteroscopy and the easier access to this advanced endoscopic technique.
Despite the large population studied, some limitations must be highlighted, especially the retrospective nature of the study. Moreover, the heterogeneity of the indications in the OSBB group and the different types of videocapsules and scopes used may have influenced the results. The indications are not comparable with those of other studies as the clinic is a referral center for celiac disease and CD; however, this has allowed us to describe the clinical impact of VCE and DBE in a large number of patients belonging to these groups.
Conclusion
Overall, these findings show for the first time that VCE is a valuable and effective tool for the management of patients with suspected or known complicated CeD, CD, suspected enteric neoplasm, or persistent digestive symptoms, and that its role is comparable with its existing role in suspected bleeding of the small intestine. In the same way, we also showed that DBE is useful in the clinical management of enteropathies without suspected bleeding because of its high DY and because therapeutic procedures may be performed without resorting to surgery.
Supplemental Material
sj-docx-1-tag-10.1177_17562848231176424 – Supplemental material for Clinical impact of videocapsule endoscopy and device-assisted enteroscopy in non-bleeding small bowel lesions
Supplemental material, sj-docx-1-tag-10.1177_17562848231176424 for Clinical impact of videocapsule endoscopy and device-assisted enteroscopy in non-bleeding small bowel lesions by Matilde Topa, Nicoletta Nandi, Lucia Scaramella, Michele Puricelli, Marco Pennazio, Reena Sidhu, David S. Sanders, Gian Eugenio Tontini, Roberto Penagini, Maurizio Vecchi and Luca Elli in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-docx-2-tag-10.1177_17562848231176424 – Supplemental material for Clinical impact of videocapsule endoscopy and device-assisted enteroscopy in non-bleeding small bowel lesions
Supplemental material, sj-docx-2-tag-10.1177_17562848231176424 for Clinical impact of videocapsule endoscopy and device-assisted enteroscopy in non-bleeding small bowel lesions by Matilde Topa, Nicoletta Nandi, Lucia Scaramella, Michele Puricelli, Marco Pennazio, Reena Sidhu, David S. Sanders, Gian Eugenio Tontini, Roberto Penagini, Maurizio Vecchi and Luca Elli in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.