
Abstract
Objective
To evaluate the clinical efficacy of double-balloon endoscopy (DBE) for small bowel disease (SBD).
Methods
The clinical and endoscopic data of patients who underwent DBE in a Chinese tertiary hospital from January 2006 to December 2019 were retrospectively reviewed. The patients were divided into three groups by age: the young group (<45 years), middle-aged group (45–65 years), and older group (>65 years).
Results
In total, 1177 patients who underwent 2134 DBE procedures were included. The anterograde and retrograde route was used in 1111 and 1023 procedures, respectively. The most common reason for performing DBE was suspected small bowel bleeding (SSBB) (53.1%), and the most common SBD was Crohn's disease (CD) (18.1%). Hemostasis was the predominant endoscopic therapy (54.3%). The total complication rate was 0.8%. The incidence of CD was highest in the young group, and the incidence of tumors was highest in the older group; these findings were consistent both among the overall patient population and among patients with SSBB.
Conclusions
DBE is effective and safe for the diagnosis and treatment of SBD and is considered to have great potential as a first-line method for diagnosing SBD.
Keywords
Introduction
Small bowel disease (SBD) is intrinsically difficult to diagnose because the small bowel is the longest part of the gastrointestinal (GI) tract (approximately 3–6 m in length). 1 SBD lacks typical signs and symptoms, making its diagnosis and therapy challenging to gastroenterologists. Additionally, assessment of the whole small intestine was difficult before development of video capsule endoscopy (VCE) and balloon-assisted endoscopy (BAE).
VCE is considered a noninvasive method for inspecting the GI tract with minimum discomfort and has developed into a first-line assessment technique for the small intestine. In contrast to VCE, BAE has the advantage of facilitating collection of biopsy specimens for histologic analysis and can provide therapeutic effects if necessary. 2 BAE is normally divided into double-balloon endoscopy (DBE) and single-balloon endoscopy (SBE). DBE was first described in 2001 and has since become a standard method for diagnosis of SBD in clinical practice.3,4 Compared with SBE, DBE allows for a more complete small bowel evaluation through a combination of retrograde and anterograde procedures. 5
Increasingly more studies are focusing on the value of DBE in patients with SBD. However, these studies have mainly focused on the efficacy of DBE in patients with different indications, such as suspected small bowel bleeding (SSBB), Crohn’s disease (CD), and similar conditions.6–13 Few reports in China have focused on SBD detection by DBE in patients of different ages.14,15
In this study, we retrospectively analyzed the indications, insertion route/depth, diagnostic yield, therapeutic yield, and safety of more than 2000 retrograde and anterograde DBE procedures in our hospital during a 14-year period. We particularly focused on the diagnostic yield of DBE in patients of different age groups and the diagnostic value of DBE in patients with SSBB of different age groups.
Materials and methods
Patients
We performed a retrospective review of patients who underwent DBE from January 2006 to December 2019. Data were collected from the electronic medical records system in our endoscopy center. Demographic data, indications, procedure time, insertion route/depth, total enteroscopy, diagnostic yield, therapeutic yield, and complications were collected and analyzed. The depth of insertion was based on the endoscopist’s report of the anatomic extent reached, and anatomic regions were used because exact measurements were not consistently available. Verbal and written informed consent was obtained from all patients before enrollment. This study was performed in conformity with the Declaration of Helsinki, and the study protocol was approved by the Medical Ethics Committee of Renmin Hospital of Wuhan University.
Preoperative preparation
All patients underwent a ≥12-hour fast before the DBE procedure. Bowel preparation was not mandatory in patients treated by the anterograde route. However, bowel cleansing (administration of polyethylene glycol electrolyte solution mixed with 2000 mL of water about 4 hours before DBE) was needed for patients treated by the retrograde route. The initial insertion route was directly based on the patient’s clinical information and/or medical history. In patients with melena, when the results of VCE and/or computed tomography/magnetic resonance enterography (CT/MR enterography) showed that the lesion was possibly in the jejunum, the initial insertion route was the anterograde approach. In patients with hematochezia, when the results of VCE and/or CT/MR enterography showed that the lesion was possibly in the ileum, the initial insertion route was the retrograde approach. When the location was uncertain, the retrograde route was preferred. The procedure was performed with the patient under general anesthesia (intravenous propofol, 2–3 mg/kg per hour) with cardiorespiratory monitoring.
DBE system and procedure
All DBE procedures were performed by experienced endoscopists using the EN-450P5, 450T5, or EN-530T endoscopy system (Fujifilm, Tokyo, Japan) according to the principles and techniques described by the innovators Yamamoto et al. 3 Carbon dioxide insufflation was used during the DBE procedure without X-ray fluoroscopy guidance. The operation was ended if the target lesion was reached or no further progress was considered possible. In patients with no history of abdominal surgery, we inserted the endoscope as far as possible if total small bowel evaluation was required, even if the lesion had already been found.
Endoscopic therapy
Endoscopic hemostasis was performed by electrocoagulation using an argon plasma coagulation (APC) device (Erbe, Tubingen, Germany) and clipping using a Resolution Clip Device (Boston Scientific, MA, USA) and QuickClip 2 (Olympus, Tokyo, Japan). A submucosal injection of adrenaline was administered before APC and clipping if needed. Enteroscopic resection of sessile polyps was performed according to a previous description.7,16
Statistical analysis
Continuous variables are expressed as mean ± standard deviation. Analysis of variance was used to compare differences in multiple testing. For comparison of categorical variables, the chi-square test and/or Fisher’s exact test were used as appropriate. Differences were considered significant at a P value of <0.05. The statistical analysis was performed using IBM SPSS Statistics for Windows, version 22.0 (IBM Corp., Armonk, NY, USA).
Results
Patients’ clinical characteristics
A total of 1219 patients underwent 2176 DBE procedures for SBD during the study period. Terminal ileal intubation could not be performed in 17 patients (17 DBEs), an anesthetic risk was identified in 15 patients (15 DBEs), and insufficient bowel preparation occurred in 10 patients (10 DBEs). Therefore, 1177 patients (2134 DBEs) with SBD were enrolled in this study (Figure 1). The patients’ mean age was 44.9 ± 17.5 years, and 67.6% patients were male. The patients were divided into three groups by age: the young group [<45 years, n = 508 (43.2%)], middle-aged group [45–65 years, n = 398 (33.8%)], and older group [>65 years, n = 271 (23.0%)]. The most common indication for DBE was SSBB (53.1%), followed by chronic abdominal pain (24.9%) and abdominal distention (5.5%) (Table 1).

Flowchart for the process of identifying the study cohort. DBE: double-balloon endoscopy; SBD: small bowel disease.
Patients’ baseline characteristics.

Data are presented as mean ± standard deviation or n (%).
DBE: double-balloon endoscopy; SSBB: suspected small bowel bleeding.
Characteristics of DBE technique
The procedure time was calculated based on 772 retrograde and 844 anterograde procedures. The mean procedure time for the retrograde approach was 122.3 ± 26.5 minutes, which was significantly longer than that of the anterograde approach (57.3 ± 29.4 minutes, P < 0.01) (Table 2). The depth of insertion was calculated based on 888 retrograde and 838 anterograde procedures. Insertion to the proximal ileum and deeper small bowel was achieved by retrograde procedures in 28.6% of cases, while insertion to the distal jejunum and deeper small bowel was achieved in 74.9% of anterograde procedures (Table 2). Retrograde DBE alone was performed in 184 patients, and anterograde DBE alone was performed in 108 patients. Bidirectional DBE was performed in 985 patients, and total small bowel evaluation was performed in 641 patients; thus, the rate of successful total enteroscopy was 65.1% (Table 2).
Characteristics of DBE technique.

Data are presented as mean ± standard deviation, n, or n (%).
*Data from 772 retrograde and 844 anterograde procedures. #Data from 888 retrograde and 838 anterograde procedures.
DBE: double-balloon endoscopy.
Endoscopic findings and their locations
The overall diagnostic yield of DBE was 60.2% (709/1177). The most common SBDs were CD (18.1%), tumors (16.7%), and nonspecific enteritis (7.0%). Other frequent SBDs were diverticula (59 cases), angioectasias (51 cases), and polyps (40 cases) (Table 3). Among the 213 cases of CD, the most common location was the ileum (79.8%). The proportion of patients with CD in the ileum was significantly higher than that in the proximal small bowel (P < 0.01). The ileum was also the most common location of nonspecific enteritis (72.0%). The most common site of tumors was the proximal small bowel (64.3%). The proportions of stromal tumors (72.1%) and adenocarcinoma (67.2%) were significantly higher in the proximal small bowel (P < 0.01), whereas the proportion of lymphoma was lower in the ileum (32.0%), although without statistical significance (Table 3).
Endoscopic findings and their locations detected by DBE.

*The difference between the ileum with proximal small intestine (jejunum and duodenum) was analyzed.
DBE: double-balloon endoscopy.
Endoscopic therapy
In total, 127 therapeutic procedures were performed in 122 patients. The most common procedure was hemostasis (58.2%). Endoscopic hemostasis included APC (25.4%), the use of hemoclips (22.1%), and epinephrine injection (10.7%). Polypectomy was performed in 36 patients (29.5%). Foreign body removal and dilatation of stenosis was performed in nine and six patients each (Table 4).
Endoscopic therapy during DBE.

APC: argon plasma coagulation; DBE: double-balloon endoscopy.
DBE-associated complications
Nine patients developed DBE-associated complications (0.8%). These complications occurred during diagnostic procedures in three patients and during therapeutic procedures in six patients. The complication rates during retrograde and anterograde DBE were 0.3% (3/1023) and 0.5% (6/1111), respectively. The most common diagnostic complication was pancreatitis (n = 2). The most common therapeutic complication was perforation (n = 4), all cases of which occurred during polypectomy in patients with Peutz–Jeghers syndrome (Table 5).
DBE complications during diagnosis and therapy.

DBE: double-balloon endoscopy.
Diagnostic yield of DBE in different age groups
The diagnostic yield was 59.8%, 58.5%, and 63.1% in the young, middle-aged, and older group, respectively. There was no significant difference in the diagnostic yield between any two groups (Figure 2(a)). A total of 148 cases of CD occurred in the young group (29.1%), 62 in the middle-aged group (15.6%), and 3 in the older group (1.1%). There was a significant difference in the diagnostic yield between any two groups (P < 0.01). Forty-two cases of tumors occurred in the young group (8.3%), 47 in the middle-aged group (11.8%), and 106 in the older group (39.1%). There was no significant difference in the diagnostic yield between the young and middle-aged groups, but there was a significant difference in the diagnostic yield between the young and older groups and between the middle-aged and older groups (P < 0.01). Among patients with nonspecific enteritis, diverticula, and angioectasias, the differences in the diagnostic yield between any two age groups are shown in Figure 2(b).
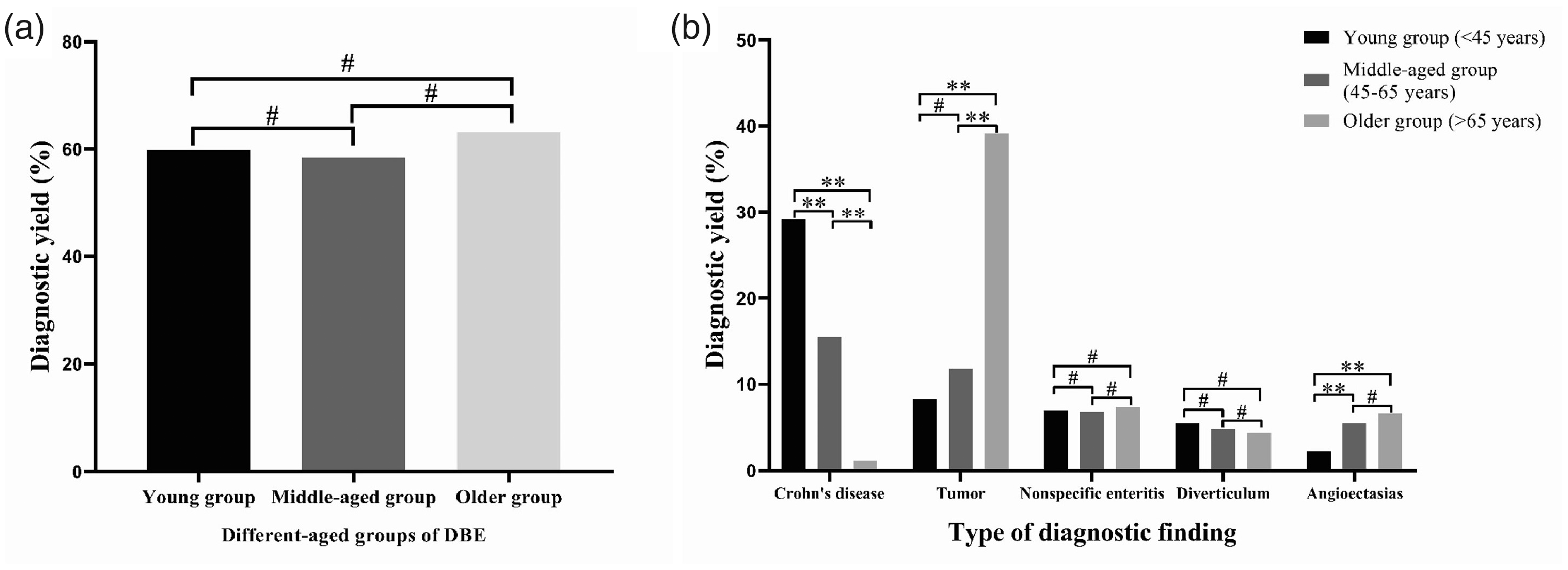
(a) Diagnostic yield of DBE in different age groups. (b) Diagnostic yield of DBE of various types of endoscopic findings in different age groups. DBE: double-balloon endoscopy. *P < 0.05, **P < 0.01, #P > 0.05.
Diagnostic yield of DBE in patients with SSBB in different age groups
The total diagnostic yield for SSBB was 62.6% (391/625). The diagnostic yield of DBE in patients with SSBB was 56.3%, 59.8%, and 74.0% in the young, middle-aged, and older groups, respectively. There was no significant difference in the diagnostic yield between any two groups (Figure 3(a)). Forty-four cases of CD occurred in the young group (18.0%), 9 in the middle-aged group (4.5%), and one in the older group (0.7%). There was a significant difference in the diagnostic yield between any two groups (P < 0.01 or P < 0.05). Eight cases of tumors occurred in the young group (3.3%), nine in the middle-aged group (4.5%), and 58 in the older group (32.0%). There was no significant difference in the diagnostic yield between the young and middle-aged groups, but there was a significant difference in the diagnostic yield between the young and older groups and between the middle-aged and older groups (P < 0.01) (Figure 3(b)). Among patients with nonspecific enteritis, diverticula, and angioectasias, the differences in the diagnostic yield between any two groups are shown in Figure 3(b).

(a) Diagnostic yield of DBE in patients with SSBB in different age groups. (b) Diagnostic yield of DBE in patients with SSBB characterized by various types of endoscopic findings in different age groups. DBE: double-balloon endoscopy; SSBB: suspected small bowel bleeding. *P < 0.05, **P < 0.01, #P > 0.05.
Discussion
DBE is not only a diagnostic tool but also a therapeutic method that has been considered the gold standard technique for endoscopic evaluation of the small intestine since its initial development nearly 20 years ago. In this retrospective study, we analyzed the data of more than 2000 cases of DBE procedures performed during a 14-year period.
Increasingly more studies are showing that SSBB is the major indication for DBE, and DBE may be preferred when complete small bowel visualization is anticipated because lesions are located in the midportion of the small bowel or multiple lesions are present throughout the small bowel. 17 The diagnostic strategy for SSBB includes several steps. 1 The first step is to perform second-look upper endoscopy and colonoscopy procedures with or without push enteroscopy. If the results of the second-look investigations are normal, the next step is typically an assessment of the small bowel. VCE is recommended as the first-line investigation technique for small bowel bleeding if no obstruction is present. CT/MR enterography is recommended if the patient has a possible obstruction. If the results of VCE or CT/MR enterography are positive, the next step is specific management, such as device assisted endoscopy, surgery, and/or intraoperative endoscopy. If the results of VCE or CT/MR enterography are negative, the next step is clinical follow-up.
The diagnostic yield for SSBB ranges from 58% to 78%. 18 The most common reason for performing DBE was also SSBB (53.1%) in the present study. The diagnostic yield for SSBB was 62.6%, which is similar to previous studies.19,20 In the current study, angioectasias, tumors, and diverticula were the three most common etiologies of SSBB (12.5%, 12.0%, and 10.9%, respectively). Previous studies from Asia showed that a tumor was the most common etiology of SSBB21,22; however, angiodysplasia was considered the most common cause of SSBB in Western studies. 23 In our previous study, the three most frequent diagnoses were angioectasias, diverticula, and tumors. 7 The reason for the inconsistency in our research outcomes may be the differences in the patient enrollment criteria.
When the lesion location was uncertain, the retrograde route was preferred. This is not consistent with the recommendation of the European Society of Gastrointestinal Endoscopy. 2 We preferred the retrograde route for two main reasons. First, we found that the most common SBD was CD in our clinical practice, and the retrograde approach should be considered first in such cases given the propensity of CD to involve the distal small bowel.24,25 Second, two patients were found to have pancreatitis when using the anterograde approach as the initial insertion route, necessitating a longer hospitalization time and higher clinical expense.
In this study, the proportion of CD was higher in the ileum than in the jejunum, which is similar to previous reports. 26 Therefore, retrograde DBE should be recommended in patients with suspected CD. Additionally, the outcomes of CT/MR enterography or VCE might help to determine the preferred route for DBE. In the present study, all patients diagnosed with CD had been examined by colonoscopy; however, only 57 patients with CD had already had positive ileocolonoscopy findings. We were unable to acquire an adequate pathological sample from every patient with suspected CD through ileocolonoscopy. Hence, DBE investigations were required for those patients to achieve a definitive diagnosis. In addition, typical endoscopic findings such as longitudinal ulcers or a cobblestone appearance can help to achieve a diagnosis of CD in clinical practice. However, CD can only be diagnosed after ruling out other possible causes. Some cases of CD are very difficult to differentiate from Behcet’s syndrome, drug-induced ulcers, nonspecific enteritis, and other conditions. There is no one test that can be used to diagnose CD alone. A combination of tests is needed to help confirm a diagnosis of CD, such as blood tests, ileocolonoscopy, CT/MR enterography, VCE, BAE, and pathological examination. Some patients even require surgery for a definitive diagnosis. Attention should also be given to the patient’s medical history.
The three most common tumors in the present study were adenocarcinoma, stromal tumors, and lymphoma, and this order is consistent with the results of an Asian study. 27 However, Bilimoria et al. 28 found that the most common small bowel tumors were neuroendocrine tumors, adenocarcinoma, and lymphoma. In a study from Japan, lymphoma and stromal tumors were the top two small bowel tumors. 29 Other than lymphoma, most of these small bowel tumors were located in the proximal small bowel, which is also similar to previous reports.27,30 Therefore, anterograde DBE should be preferred in patients with a suspected tumor but with no clinical information.
The rate of complete small bowel examination widely ranges from 5% to 93% among previous studies.31–33 The reason for this notable discrepancy is largely unclear but may be explained by different centers’ experience levels and quality of reporting. In this study, the rate of total endoscopy (65.1%) was similar to that in previous Asian reports.9,34 The target lesion was found in 217 of all cases in which total enteroscopy was attempted. Among them, 64 benefited from complete small bowel evaluation to achieve a definitive diagnosis. To minimize the rate of missing lesions, we attempted to complete a total GI tract examination in patients without a history of abdominal surgery. Increased levels of one or more pancreatic serum marker (e.g., hyperlipasemia) is very common after an anterograde DBE procedure of long duration, and acute pancreatitis may occur in patients who had abdominal pain when they underwent anterograde DBE. 35 Normally, the amylase level would be checked after a >2-hour procedure using the anterograde approach in our center.
Study limitations
Some limitations of this study must be acknowledged. First, it was a single-center retrospective study. Possible bias might have existed in assessing the clinical value of the study findings. Second, evaluation of the insertion depth might have differed among the endoscopists. Finally, follow-up was not considered because it was not the main point of the study; however, false-negative findings may occur even if a total small bowel evaluation is completed during bidirectional DBE procedures.
Conclusions
This study underlines the use of DBE for diagnosis and therapy of SBD, especially with respect to the diagnostic yield in different age groups. We found that DBE is effective and safe for the diagnosis and therapy of SBD. DBE can be regarded as a very promising means for diagnosing SBD. Prospective studies should concentrate on advances in the DBE technique with proper patient selection; this may lead to higher diagnostic and therapeutic yield and lower complication rates.
Footnotes
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.