
Abstract
Background:
Adherence to inflammatory bowel disease (IBD) medication is crucial to maintain remission, especially during pregnancy.
Objective:
To examine the influence of family planning and pregnancy-related patient knowledge regarding IBD and pregnancy on adherence.
Design:
Cross-sectional survey study
Methods:
We surveyed female patients with IBD aged 18–35 years, who at recruitment to the UK IBD BioResource had not had children. We elicited disease and treatment history, demographics and family planning status via an online questionnaire. Patient knowledge as assessed by the validated Crohn’s and Colitis Pregnancy Knowledge Score (CCPKnow) and adherence by visual analogue scale (VAS).
Results:
In 326 responders (13.8% response rate), good adherence (VAS ⩾ 80) was found in only 38.35%. Disease- and treatment-related factors were not significantly associated with good adherence, except for methotrexate (70.0% adherent of 10 exposed patients versus 37.2% non-exposed; p = 0.036). Patients planning pregnancy for the next year were more often adherent (59.0% versus 35.5%; p = 0.019) and knowledgeable (median CCPKnow 8 versus 7; p = 0.035) compared to those in other family planning categories. Pregnancy-related patient knowledge was significantly associated with adherence (Pearson correlation 0.141; p = 0.015). Adherent patients had significantly higher CCPKnow scores than non-adherent patients (median 8 versus 6; p = 0.009). On binary regression analysis, only planning to conceive within 12 months was independently associated with better adherence (p = 0.016), but not methotrexate exposure (p = 0.076) and CCPKnow (p = 0.056).
Conclusions:
In a cohort of women of childbearing age with IBD overall medication, adherence was low. Planning to conceive within the next year was associated with better adherence and greater patient knowledge.
Background
Inflammatory bowel diseases (IBDs) are chronic diseases that may cause inflammation, ulceration, fistulation and/or stenoses in the gastrointestinal tract. 1 IBD often presents in early adolescence or young adults and therefore affects women of childbearing age with an increasing prevalence of IBD. 2 Active inflammation during conception and pregnancy can adversely affect pregnancy outcomes in patients with IBD.3–5 Active inflammation from IBD should be treated with effective medication prior to and during pregnancy including mesalazine, thiopurine and biologics. 5 Strict control of inflammation is associated with better pregnancy outcomes but requires adherence to maintenance medication for IBD. Medication adherence in general is suboptimal in patients with IBD, 6 and a limited number of studies examining adherence during pregnancy have reported levels of non-adherence around 30–40%.7–9 While the studies examining adherence during pregnancy report slightly better levels than seen outside pregnancy the overall adherence level remains a risk to mother and foetus. 9 Interestingly Watanabe et al. 9 found that adherence dropped from the preconception period to the first trimester of pregnancy.
Many women of childbearing age have concerns about potential medication side effects on the unborn child, 10 although most IBD medications are recommended to be continued during pregnancy by international guidelines.5,11,12 Many women of childbearing age have poor knowledge of IBD and pregnancy-related issues,13–15 which is associated with views contrary to evidence-based medical guidelines and patient facing treatment guidances. 16 In the general IBD population, poor adherence to medical therapy is also associated with higher healthcare costs. 6 Causes of non-adherence are incompletely understood. A lack of belief in the necessity of medications to maintain disease remission and concerns about potential medication toxicity have been reported by several studies.17–19 However, disease-related patient knowledge about IBD in general has previously been found to not predict medication adherence.19,20
Pre-pregnancy counselling to address the importance of controlling IBD by continued maintenance medication has been shown to improve patient knowledge and pregnancy outcomes in women with IBD. 21 While this approach works for women actively choosing to start a family, it will fall short in those 45% of pregnancies in the United States and in the United Kingdom that are unplanned.22,23 There are some variations in unplanned pregnancies around the world, which may alter the potential benefits of pre-pregnancy counselling. It is therefore important to examine adherence in women of childbearing age. We have previously examined medication adherence in women aged 18–45 who were under the care of a specialist IBD clinics in Sydney, Australia. 24 In this pilot study, we found that while adherence was generally high, an association between adherence- and IBD-related pregnancy knowledge was observed on binary analysis Crohn’s and Colitis Pregnancy Knowledge Score (CCPKnow: p = 0.02) with borderline results on continuous analysis (CCPKnow: p = 0.08). 24 Therefore, larger studies in a more general setting representing the wider IBD patient community outside of specialist services were required.
We therefore aimed to examine medication adherence and disease-specific knowledge in women of childbearing age that have mainly not had children yet by examining the UK IBD BioResource cohort.
Methods
Study cohort
The UK IBD BioResource is an open research platform that started prospectively recruiting patients with IBD from over 100 UK hospitals in 2016. 25 By 2019, 25,000 patients had been included and current recruitment stands at over 35,000 patients. Patients provide baseline data on inclusion; disease and treatment characteristics are collected from medical records at baseline and blood sampled for genetic analysis. 25 Patients can also consent to be contacted for further studies nested within the UK IBD BioResource cohort. 26 For this study, we approached 2399 female patients aged 18–35 years, who at recruitment to UK IBD BioResource had not had children. Our survey was targeted to include patients who were yet to have children, but we had no prior update of patients’ family status prior to this survey. Those who declared having had children on survey invitation were deemed not eligible, but we did not exclude those who had children but proceeded to give survey responses regardless.
Recruitment and study procedures
Potential participants were contacted by email on up to three occasions and invited to fill in an electronic survey hosted on the secure Research Electronic Data Capture (REDCap) research environment. Study data were collected and managed using REDCap electronic data capture tools hosted at Leeds Teaching Hospitals.27,28 REDCap is a secure, web-based software platform designed to support data capture for research studies. Participants provided informed consent after reading the online patient information leaflet by continuing to the research questionnaire and answered questions around current relationship status, current reproduction, future reproduction intentions, current disease state and current IBD medication. Medication adherence was assessed by a visual analogue scale (VAS; 0–100), which has been validated for IBD with a cut-off of ⩾80 deemed as adherent. 29 We assessed current psychological state with the Hospital Anxiety and Depression Scale (HADS). 30 Pregnancy-related IBD knowledge was assessed by the CCPKnow, a validated self-assessment tool with score ranging from 0 to 17 and scores ⩾8 deemed adequate. 13 Patients self-rated their disease control during the preceding year on a simple 4-point scale from remission, mild, moderate and severe disease. Demographic and phenotype type data were extracted from the UK IBD BioResource.
Statistical analysis plan
Based on the 74% adherence rate found in a prior UK-based IBD study, 31 a minimum of 296 patients were required to be enrolled in this study to achieve a 95% confidence level and 5% margin of error. Descriptive statistics are reported as mean or proportions. Categorical data were compared between groups using chi-square test, whereas independent samples t-test was used for normally distributed continuous variables and Mann–Whitney U-test for non-normally distributed continuous variables. We performed a binary regression analysis to determine factors independently associated with medication adherence. Differences were considered statistically significant if p < 0.05. IBM SPSS version 25 (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp) was used for statistical analysis.
Results
Cohort composition, disease and treatment characteristics
We invited a total of 2399 UK IBD BioResource participants, 73 of whom declined and 112 were found to be ineligible. We received 316 (13.8%) responses with sufficient data for analysis. Respondents were aged 18–34 years and predominantly of white British ethnicity (Table 1). Disease phenotype, surgical history and current treatment are displayed in Table 2. Medication exposure included current use of mesalazine in 90 (28.5%), thiopurines in 94 (29.7%), methotrexate in 10 (3.2%), anti-Tumour Necrosis Factor-antagonists in 103 (32.6%), vedolizumab in 38 (12.0%), ustekinumab in 30 (9.5%) and tofacitinib in five cases (1.6%). Steroid exposure occurred in 77 (24.4%) in preceding year, whereas 38 (12.2%; Table 2) required a hospital admission in the preceding year. Current self-rated disease activity was remission in 96 (30.8%), mild in 121 (38.8%), moderate in 74 (23.7%) and severe in 21 (6.7%) of participants.
Patient demographics and social background.

Disease phenotype and treatment.

Percentages are calculated for the whole cohort for diagnosis and medical treatment. For phenotype, surgery and stoma data, the percentages are calculated for the CD and the UC/IBD-U cohort separately. Where data do not add for the total cohort, we omitted missing data.
CD, Crohn’s Disease; IBD-U, Inflammatory Bowel Disease-Unclassified; UC, ulcerative colitis.
Mental health, knowledge and adherence
Results for HADS, CCPKnow and VAS were not normally distributed and hence analysed with non-parametric tests. HADS was separately analysed for anxiety (HADSA) and depression (HADSD). Median anxiety score (HADSA) was 9 [interquartile range (IQR) 6–12], 52.9% had a score ⩾9 (possibly abnormal), whereas 24.9% had an abnormal score of ⩾12. Median depression score (HADSD) was 4 (IQR 2–7), 10.1% had a score ⩾9 (possibly abnormal), whereas 2.0% had an abnormal score of ⩾12. Median disease-related pregnancy knowledge score (CCPKnow) was 7 (IQR 4–10), with at least adequate knowledge (⩾8) found in 44.5%. Median adherence score (VAS) was 51 (IQR 51–100) with good adherence (⩾80) found in 38.35%.
Factors associated with good adherence
Age, ethnicity, household income, level of education, employment status, relationship status, sexual orientation, self-rated disease activity, type of IBD diagnosis, IBD phenotype, having a stoma, IBD-related surgery, having extra-intestinal, manifestations, hospital admission within 12 months, steroid exposure within 12 months, having discussed family planning with a healthcare professional were all not associated with good adherence (all chi-square tests p > 0.05). Exposure to different types of IBD medication was not significant when assessed for binary adherence outcomes except for methotrexate. Patients exposed to methotrexate were more likely to be adherent than those not exposed (70.0% adherent versus 37.2%; p = 0.036); however, this was in a very small sample (n = 10). Current family planning intentions were associated with significant differences in adherence status. Those planning for a pregnancy in the next year were significantly more likely to be adherent (59.0%) compared to those who had actively aimed for a pregnancy (previous pregnancy, currently pregnant and currently aiming to conceive; 33.3%), those planning for children in the more distant future (38.7%) and those not planning to have children (29.0%; p = 0.019). Patients planning to conceive had significantly higher CCPKnow scores than those meeting criteria for the other family planning categories (median 8 versus 7; p = 0.035).
Disease-related patient knowledge (CCPKnow) was significantly associated with adherence [Pearson correlation 0.141 (weak correlation); p = 0.015; Figure 1(a)]. Adherent patients had significantly higher CCPKnow scores than non-adherent patients [median 8 (IQR 5–12) versus 6 (IQR 3–10); p = 0.009; Figure 1(b)]. HADSA and HADSD were not significantly associated with adherence.

Relation between adherence and CCPKnow. (a) Correlation analysis and (b) categorical analysis.
Binary regression analysis (mode: enter) revealed that planning to conceive within 12 months was independently associated with better adherence [odds ratio (OR) 2.363 95% confidence interval (CI) 1.177–4.478; p = 0.016; Table 3], whereas methotrexate exposure (OR 3.507 95% CI 0.876–14.044; p = 0.076) and CCPKnow (OR 1.600 95% CI 0.987–2.593; p = 0.056) did not meet significance criteria.
Factors associated with good adherence.
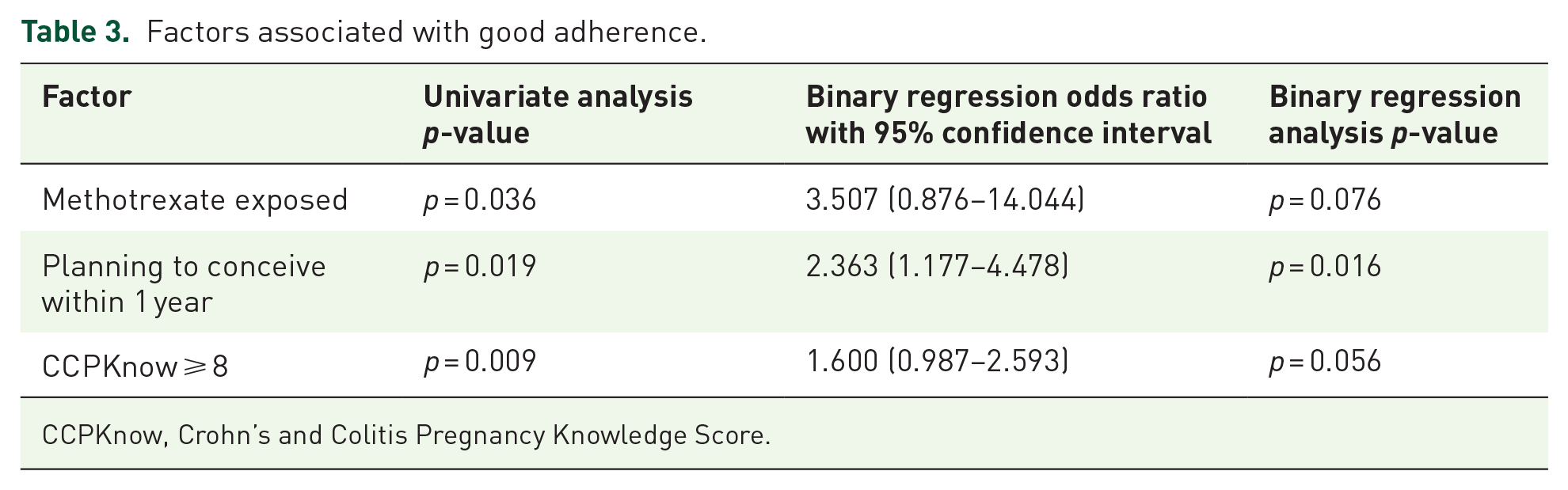
CCPKnow, Crohn’s and Colitis Pregnancy Knowledge Score.
Discussion
We examined medication adherence in a large cohort of women of childbearing age who had not had children and found low adherence rates of only 38.4%. Based on our pilot work, 24 we aimed to confirm whether patient knowledge of IBD and pregnancy is associated with good adherence to IBD maintenance medication in women of childbearing age. We identified that future family plans, especially the wish to conceive within the next year, was associated with better adherence and better patient knowledge of IBD- and pregnancy-related issues.
Adherence levels in our study (38.4%) were considerably lower than those seen in other cohorts of women with IBD of childbearing age. In 2016, we found that good adherence as measured by the medicine adherence rating scale (MARS) 32 was 74.4% in 1324 women, who were members of the UK IBD patient support charity. 31 Our pilot study of women under the specialist Sydney IBD clinic found again high adherence rate of 84% using MARS. 24 During pregnancy, adherence rates vary widely with some studies reporting excellent adherence, 33 some suboptimal adherence7,8 and in one study nearly 50% became non-adherent. 20 Our current study population differs significantly from those cohort as we did not aim to include patients who already have children. Furthermore, patient support charity membership is associated with better adherence, and we expect that membership will be low in our cohort as seen in most cohort studies. 19 The Sydney cohort was under a single specialist clinic, which will have likely also increased adherence. 24 In addition, we used a different adherence measure. Although VAS is fully validated against thiopurine metabolite levels in IBD with good correlation with MARS too, there are obvious differences in the way adherence was measured. 29
Following on from our pilot study, we confirmed the association of better disease-related pregnancy knowledge and adherence, both on binary and correlation analyses. Through regression analysis, we established that the main effect on adherence is driven by the wish to conceive in the next year, which in turn is associated with better knowledge and better adherence. Patients may have accessed pre-pregnancy counselling, which may have helped them in increasing their knowledge and subsequently adherence, as seen in the two Danish adherence studies examining pregnant IBD cohorts.7,8 It appears that wishing to conceive may influence women to potentially educate themselves and increased adherence. This hypothesis will be tested in the longitudinal follow-up of this cohort that we plan to conduct over the next few years to determine trajectories of patient knowledge and adherence as women’s family planning decisions evolve. We have seen a numerical lower rate of adherence in those patients trying to currently conceive, but as numbers are small this may be a random non-significant finding.
In our very selected cohort of women most disease-related factors including perceived disease severity, need for hospital admission in the last year and need for steroids in the last year were not associated with adherence. Interestingly, we found that apart from methotrexate, exposure to different medications was not associated with adherence, in contrast to studies in more general IBD populations where adherence was better on biologics.6,19 As our aim was to examine the aspects around family planning on adherence, we did not examine for wider measures around adherence including belief of necessity and potential medication concerns. We found however that psychological symptoms of anxiety and depression were not associated with adherence.
The main strength of our study lies in the examination of a well-defined multi-centre cohort of women with IBD, for whom family planning decisions are most relevant as we focussed on those yet to start a family. By using the UK IBD BioResource, we have avoided influence from single centres or clinicians on adherence and knowledge, thereby examining a less select cohort. We used validated tools to assess adherence, anxiety and depression and knowledge. There are a number of limitations to our work. Firstly, we used a survey design with a relatively low response rate, which may in turn reflect that UK IBD BioResource participants get offered participation for several studies per year. Secondly, we used VAS to measure adherence, which while fully validated for IBD, is less often used than other adherence measures. This could potentially lead to differences in absolute levels of adherence but is unlikely to affect associations with adherence. Thirdly, we did not examine for necessity belief and medication concerns as due to the nature of our study the questionnaires were already relatively long. Fourthly, our sample size calculation was based on a presumed adherence rate of 74% and as our adherence rate was lower at 38%, this could have affected the statistical power to detect some associations of adherence. It would have been interesting to compare the adherence between all family planning subgroup, but our sample size was too small to allow meaningful analysis on this aspect.
In conclusion, we have demonstrated that women wishing to conceive within the next year had better adherence to IBD maintenance medication and better pregnancy-specific disease-related knowledge. Clinical teams should focus efforts on improving pre-conception knowledge as the pre-conception group demonstrated better adherence. Longitudinal follow-up of this cohort will examine whether adherence and patient knowledge changes as individual family planning decisions evolve.
Supplemental Material
sj-pdf-1-tag-10.1177_17562848231193211 – Supplemental material for Planning to conceive within a year is associated with better pregnancy-specific disease-related patient knowledge and better medication adherence in women of childbearing age with inflammatory bowel disease
Supplemental material, sj-pdf-1-tag-10.1177_17562848231193211 for Planning to conceive within a year is associated with better pregnancy-specific disease-related patient knowledge and better medication adherence in women of childbearing age with inflammatory bowel disease by Christian P. Selinger, Robyn Laube, Helen Steed, Matthew Brookes, NIHR BioResource and Rupert W. L. Leong in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
We thank NIHR BioResource volunteers for their participation and gratefully acknowledge NIHR BioResource centres, NHS Trusts and staff for their contribution. We thank the National Institute for Health and Care Research, NHS Blood and Transplant and Health Data Research UK as part of the Digital Innovation Hub Programme. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.