
Abstract
Patients with inflammatory bowel disease (IBD) are not at increased risk of SARS-CoV-2 infection compared to the general population, and most are not at increased risk for severe disease. COVID-19 is nonetheless common, and vaccination is critical. Four safe and efficacious vaccines are now available for the prevention of COVID-19, with most data available for mRNA vaccines. Patients with IBD have a robust humoral response to vaccination with rates of seroconversion exceeding 95% following a two-dose mRNA vaccine series and 99% following a three-dose mRNA series, although those on certain therapies including anti-tumor necrosis factor α agents may have lower antibody concentrations and waning of antibodies over time. Additionally, rates of cell-mediated immune response, even in those patients with IBD who did not have evidence of humoral immunity, are high. Vaccines are safe and have not been associated with flares in disease activity. Gastroenterology providers should take an active role in ensuring patients with IBD are appropriately vaccinated against COVID-19.
Introduction
To date, the COVID-19 pandemic caused by SARS-CoV-2 has led to over 6 million deaths worldwide. 1 Since the beginning of the pandemic, there has been concern that patients with inflammatory bowel disease (IBD) may be at greater risk of contracting COVID-19 as well as suffering severe COVID-19 outcomes including hospitalization, intensive care unit admission, or death, whether from factors related to IBD itself or as a result of immune modifying therapies used to treat IBD. Furthermore, while effective COVID-19 vaccine development was swift, patients with IBD were excluded from the original clinical trials which demonstrated vaccine efficacy, leading to additional uncertainty in this population. Since that time however, much data has been collected which has shown that most patients with IBD are not at increased risk for severe COVID-19 infection and that vaccines are both safe and effective in this population. This review summarizes these findings including relevant articles identified in PubMed® using search terms ‘COVID-19 vaccine and IBD’ published between March 2020 and December 2022.
COVID-19 risk in an IBD population
There does not appear to be an increased risk of contracting COVID-19 in an IBD population. This has been demonstrated in multiple studies including a nationwide retrospective study of 38,378 patients with IBD within the U.S. Veterans Affairs (VA) healthcare system that showed no increased risk of COVID-19 as compared to matched patients without IBD. 2 Similar findings have been noted both outside the VA in the United States as well as abroad.3,4 Even when accounting for immunosuppression, including anti-tumor necrosis factor α (TNF) therapy and immunomodulators, no difference in the rate of COVID-19 infection has been noted.5,6 Additionally, most studies have shown that when patients with IBD do contract COVID-19, there is not a greater risk of severe disease. This includes a retrospective population-based cohort study drawing from electronic health records of 40 million patients which showed no increased rate of hospitalization or mortality in patients with COVID-19 infection with IBD as compared to propensity-matched patients without IBD. 7
Those studies that have shown higher than expected mortality in patients with IBD have identified several potential contributing factors, including medications, age, comorbidities, IBD activity and severity, and vaccination status. 8 Perhaps most notable among these contributing factors is the use of systemic corticosteroids, which has been frequently associated with more severe disease.7,9–11 While initially there was concern from Surveillance Epidemiology of Coronavirus Under Research Exclusion (SECURE-IBD), a large international registry, that patients on mesalamine may be at risk for more severe disease, subsequent updates have not shown this to be the case, raising the question of initial reporting bias (i.e., unexpected results such as severe infection on a therapy generally considered to be low risk may have been more likely to be reported).9,11 Additionally, biologics, including anti-TNF, anti-integrins, and anti-interleukin (IL) 12/23 therapies do not appear to be associated with an increased risk of hospitalization or death from COVID-19 and may actually lower risk of these adverse outcomes . 11 As a result, providers should be aware that IBD therapies should not be interrupted due to risk of COVID-19; on the contrary, these therapies should be continued to avoid a disease flare that may require corticosteroids. Lastly, other factors that are associated with severe COVID-19 in patients with IBD are similar to those seen in other populations and include older age, increased comorbidities, and unvaccinated status.10,12,13
Vaccine recommendations
Initially approved under an emergency use authorization (EUA) by the United States Food and Drug Administration (FDA), COVID-19 vaccines were quickly incorporated into the scheduled immunization recommendations by the Advisory Committee on Immunization Practice (ACIP), a group of medical and public health experts which advises the Centers for Disease Control and Prevention (CDC). Gastroenterology societies similarly acted quickly, issuing recommendations that patients with IBD be vaccinated against COVID-19 without delay.14,15 The initial vaccine schedule consisted of two doses of BNT162b2 (Pfizer-BioNTech) given 3 weeks apart, two doses of mRNA-1273 (Moderna/National Institutes of Health) given 4 weeks apart, or one dose of Ad26.COV2.S (Johnson & Johnson). Vaccination proved to be highly effective, and prompt adoption of these vaccine recommendations changed the course of the pandemic. 16
COVID-19 vaccines remain highly effective in preventing severe disease; however, providers should be aware of several important updates. 17 In August 2021, the ACIP issued recommendations that those considered moderately to severely immunosuppressed should receive an additional dose of an mRNA vaccine administered four or more weeks after the initial regimen. 18 These recommendations came following data published in solid organ transplant recipients in which rates of seroconversion were as low as 35% after two doses of an mRNA vaccine. 19 Fortunately rates of seroconversion were subsequently shown to be significantly higher in an IBD population; however, an additional dose to complete the primary series should nonetheless be considered in those patients with IBD who are considered moderately to severely immunosuppressed as defined by the CDC Yellow Book and Infectious Disease Society of America guidelines for vaccination of an immunocompromised host.20,21 In an IBD population, this includes those treated with ⩾20 mg prednisone, anti-TNF agents, or immunomodulators including thiopurines and methotrexate. 22
Waning of vaccine-induced immunity and the emergence of highly transmissible variants including Delta prompted recommendation of a booster dose following the primary series in all adults. 23 Most recently, in response to the Omicron variant in the fall of 2022, monovalent booster doses were replaced by a bivalent booster which contains equal components from Omicron and ancestral strains. 24 The bivalent booster should be administered two or more months after completing the primary series (or two or more months after the monovalent booster if this was administered).
Note that as of December 2021, the ACIP preferentially recommends mRNA vaccines over a viral vector vaccine. This recommendation was made both in response to lower rates of seroconversion in those who received a viral vector vaccine as well as rare but serious adverse events including thrombosis with thrombocytopenia syndrome and Guillain-Barré syndrome which have been associated with viral vector vaccines. 25 Therefore, for both initial and booster doses, an mRNA vaccine should now be recommended over a viral vector vaccine.
Lastly, as of July 2022, NVX-CoV2373 (Novavax), a subunit protein vaccine administered as two-dose series 3 weeks apart, was additionally issued an EUA. Little data is available on the efficacy of this vaccine in an IBD population; however, it appears quite effective in the general population and may be an especially important vaccine in those who are hesitant to receive an mRNA vaccine or who may have an allergy to an mRNA vaccine component. 26 Those patients who receive NVX-CoV2373 should still go on to receive a bivalent mRNA booster as, to date, NVX-CoV2373 is only available as a monovalent booster. 24
Humoral immune response
Patients with IBD and other immunosuppressed populations were initially excluded from the clinical trials which resulted in COVID-19 vaccination authorization and/or approval. Given certain patients with IBD, including those on anti-TNF therapy, have been shown to have an impaired immune response to other vaccines including the influenza vaccine, there was concern that the immune modifying therapy used to treat IBD may also impact COVID-19 vaccine response.27,28 Patients with IBD however have a high rate of seroconversion following COVID-19 primary series vaccination. In fact, several large studies have shown rates of seroconversion exceeding 95% after a two-dose mRNA series.29–33 Lower rates of seroconversion have been shown in older patients as well as those treated with anti-TNF therapy (especially anti-TNF with an immunomodulator), tofacitinib, and systemic corticosteroids whereas relatively higher rates of seroconversion have been shown in those on vedolizumab, ustekinumab, and aminosalicylates.29–35 See Table 1. In those who received a third dose of an mRNA vaccine or an mRNA vaccine following an adenovirus vaccine, seroconversion is nearly universal, with rates typically exceeding 99%.36–39 See Table 2.
Humoral and CMIR after COVID-19 primary series (two-dose mRNA vaccine or one-dose adenovirus vector vaccine).
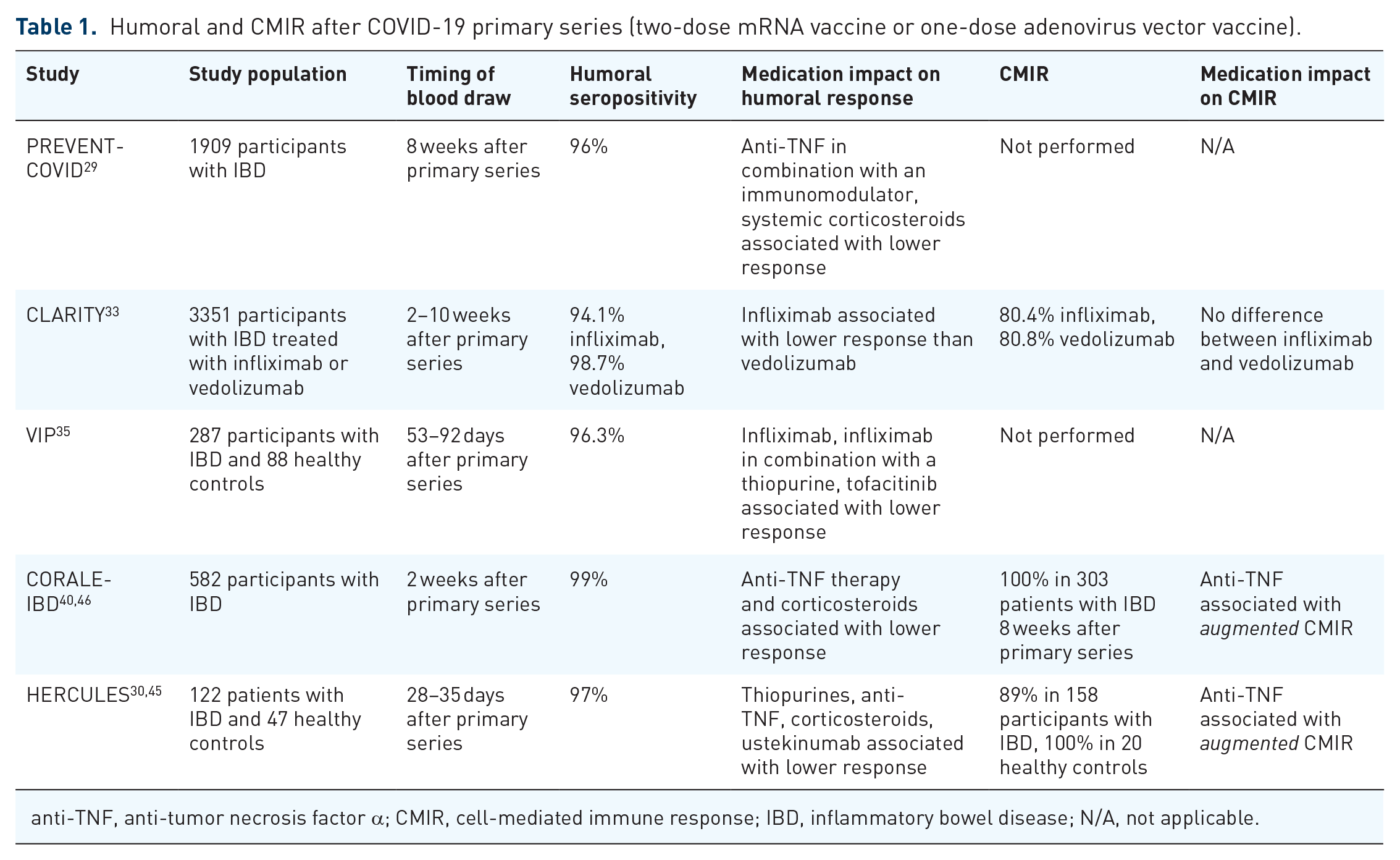
anti-TNF, anti-tumor necrosis factor α; CMIR, cell-mediated immune response; IBD, inflammatory bowel disease; N/A, not applicable.
Humoral and CMIR after additional vaccine dose (three-dose mRNA vaccine or adenovirus vaccine and one-dose mRNA vaccine).
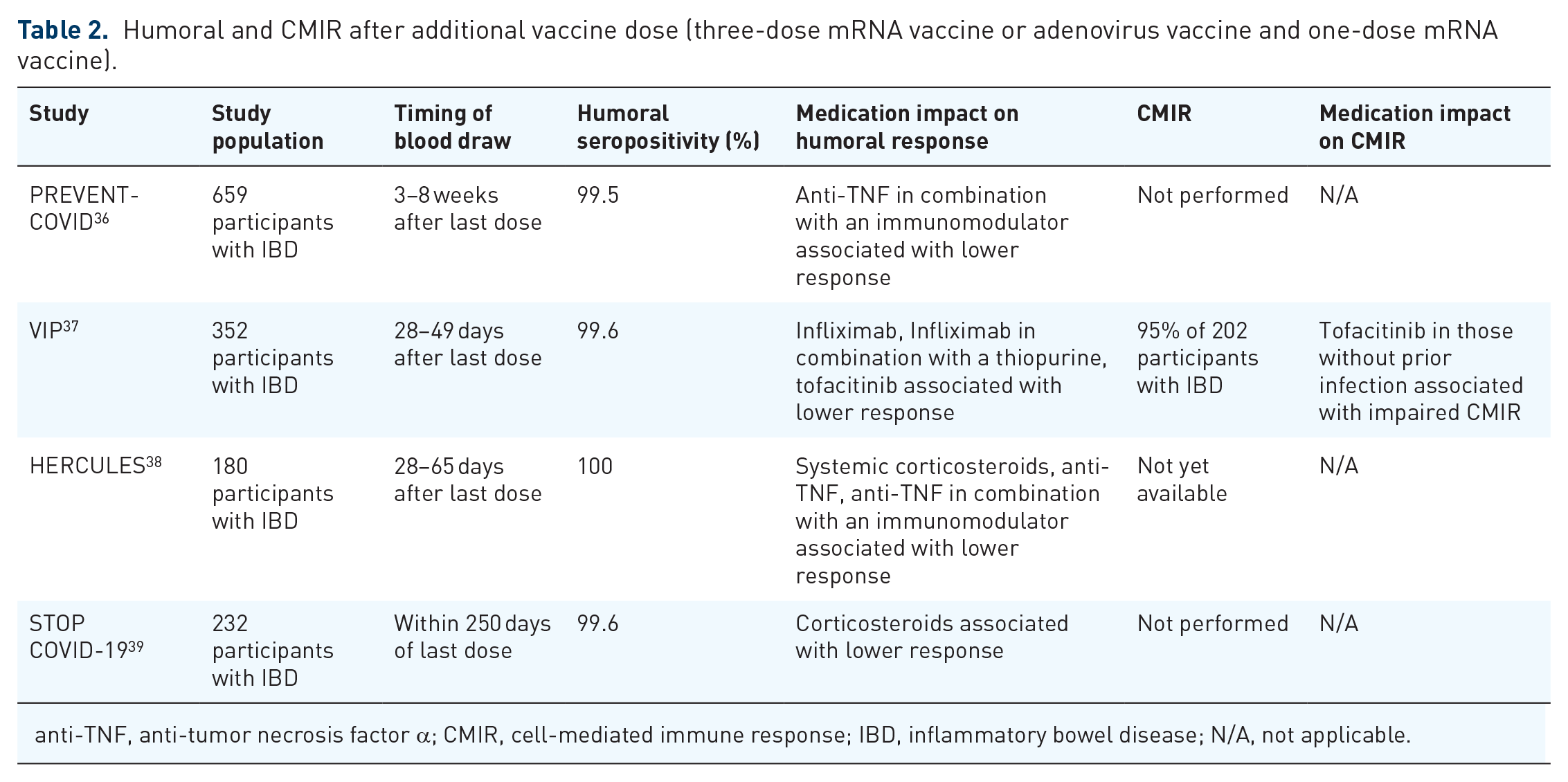
anti-TNF, anti-tumor necrosis factor α; CMIR, cell-mediated immune response; IBD, inflammatory bowel disease; N/A, not applicable.
Several studies have shown that while rates of seroconversion are high, antibody levels are lower in those with IBD on anti-TNF therapy.30,32,35,36,40 The clinical significance of this finding is unclear as there is no known antibody level which is a correlate of immunity, and even in healthy populations, antibody levels wane with time. Additionally, despite a lower mean antibody level, greater than 98% of patients with IBD still demonstrate a sustained humoral immune response 6 months after a third dose (with higher antibody levels in those with previous COVID-19 infection). 41
Lastly, it should be noted that several studies have shown lower rates of seroconversion in those who received a viral vector vaccine.35,40,42 This included data from the PREVENT-COVID cohort, in which the rate of seroconversion in 94 patients who received Ad26.COV2.S was 81% at 3 months and antibody concentrations were significantly lower than in those who received an mRNA vaccine (median 2.7 μg/mL versus 17 μg/mL with mRNA vaccines). 29 As discussed previously, this suspected lower rate of efficacy and known risk of adverse events associated with a viral vector vaccine have led to preferential recommendation of an mRNA vaccine over a viral vector vaccine. 43
Cell-mediated immunity
COVID-19-specific cell-mediated immune response (CMIR) likely additionally plays an important role in limiting disease progression as T-cells restrict cell-to-cell viral dissemination following initial infection. Furthermore, CMIR likely persists longer than waning antibody concentrations following vaccination. T-cell memory also recognizes a wide range of viral proteins, as compared to antibodies, and allows for persistent immunity even in the face of viral variants. 44 Unfortunately, assays measuring T-cell response are considerably more expensive and time-consuming than measuring antibodies, and the level of humoral response does not correlate with CMIR. 44
In those studies that have assessed T-cell response, we have seen high rates of CMIR, even in patients who lacked a humoral immune response. In the HERCULES study, nearly all patients demonstrated CMIR following two doses of an mRNA COVID-19 vaccine, similar to healthy controls. In this study, CMIR was not lower in patients with IBD taking immunosuppressant medication. In fact, those treated with anti-TNF therapy had higher CMIR . 45 An augmented T-cell response after two doses of COVID-19 vaccine was additionally seen in CORALE-IBD, although this has not been seen universally, as CLARITY-IBD showed similar (but not greater) T-cell response in those taking infliximab as compared to vedolizumab.40,46 See Table 1.
Lastly, there has been a paucity of data regarding CMIR in IBD after three doses of COVID-19 vaccine. However, in one study after three vaccine doses, only tofacitinib was associated with reduced CMIR relative to healthy controls. 37 See Table 2.
Efficacy
The clinical trials which resulted in FDA vaccine EUA and/or approval showed high rates of efficacy in preventing severe COVID-19 infection (95% BNT162b2, 94.1% mRNA-1273, 66.9% Ad26.COV2.S, 90.4% NVX-CoV2373).13,26,47,48 Notably however patients on immunosuppressive therapies were excluded from these trials. One recent population-based study in Israel compared rates of COVID-19 in patients with IBD and non-IBD controls who received BNT162b2 and found no difference in vaccine efficacy during a median 22 weeks of follow-up post vaccination. This was true even for those patients on anti-TNF agents or corticosteroids. 49 A large systematic review showed similar findings, although it did highlight a decay in titers over time, supporting the need for booster doses. 50
Safety
Several studies have shown that rates of adverse events in patients with IBD are similar to rates of adverse events noted in clinical trials of COVID-19 vaccines.13,26,47,48 PREVENT-COVID assessed adverse event rate within 7 days of receiving an mRNA or adenovirus vector vaccine in 3316 individuals with IBD. While localized reactions including tenderness or pain at the injection site were common (68% after each dose), serious adverse events, defined as reactions preventing daily activity, were rare overall. In total, only 16 adverse events required emergency room evaluation or hospitalization. 36 Following a third dose, 6% of 659 patients with IBD self-reported any severe adverse event. 51
Data from CORALE-IBD showed similar rates of adverse events in a survey of 246 patients with IBD. Adverse events were more common in younger patients (defined as less than age 55 years). 52 As in the PREVENT-COVID cohort, severe reactions after the third dose were less common than after the second. 53
Data from up to 30 days post vaccination has also been reassuring. Hadi et al. identified 5562 patients with IBD who received a COVID-19 vaccine and found no difference in adverse events as compared to a propensity score matched population without IBD who received the COVID-19 vaccine. This included adverse events of special interest such as anaphylaxis, deep vein thrombosis, and myocarditis/pericarditis. Additionally, this study showed no increase in steroid prescriptions in patients with IBD who received the COVID-19 vaccine as compared to those with IBD who were not vaccinated. 54
Similarly, over a median follow-up of 14 weeks, 707 patients with IBD stringently matched to non-IBD controls and showed no increased rate of disease flare as defined by treatment escalation, steroid initiation, or hospitalization. 49 See Table 3.
Risk of adverse events and IBD flares following COVID-19 vaccination.

IBD, inflammatory bowel disease; N/A, not applicable.
Provider role and practical considerations
Gastroenterology providers are a trusted source of information for their patients with IBD and should take an active role in ensuring patients are vaccinated against COVID-19. Indeed, provider recommendation has been shown to be an important factor in vaccine uptake, and this may be especially true for minority groups.55,56 While rates of vaccination have generally been shown to be high in an IBD population, significant disparities have been noted. In a study including over 1000 patients with IBD, those who were unvaccinated were 2.6 times more likely to identify as an underrepresented minority group. 57
As described above, in the fall of 2022, the ACIP recommended only one bivalent mRNA COVID-19 vaccine booster for persons over 5 years old administered 2 or more months after completing the primary series. Additional booster doses are no longer necessary in high-risk populations or immunosuppressed populations. Furthermore, providers should also be aware it is likely that COVID-19 booster vaccination will be recommended in the fall of 2023.
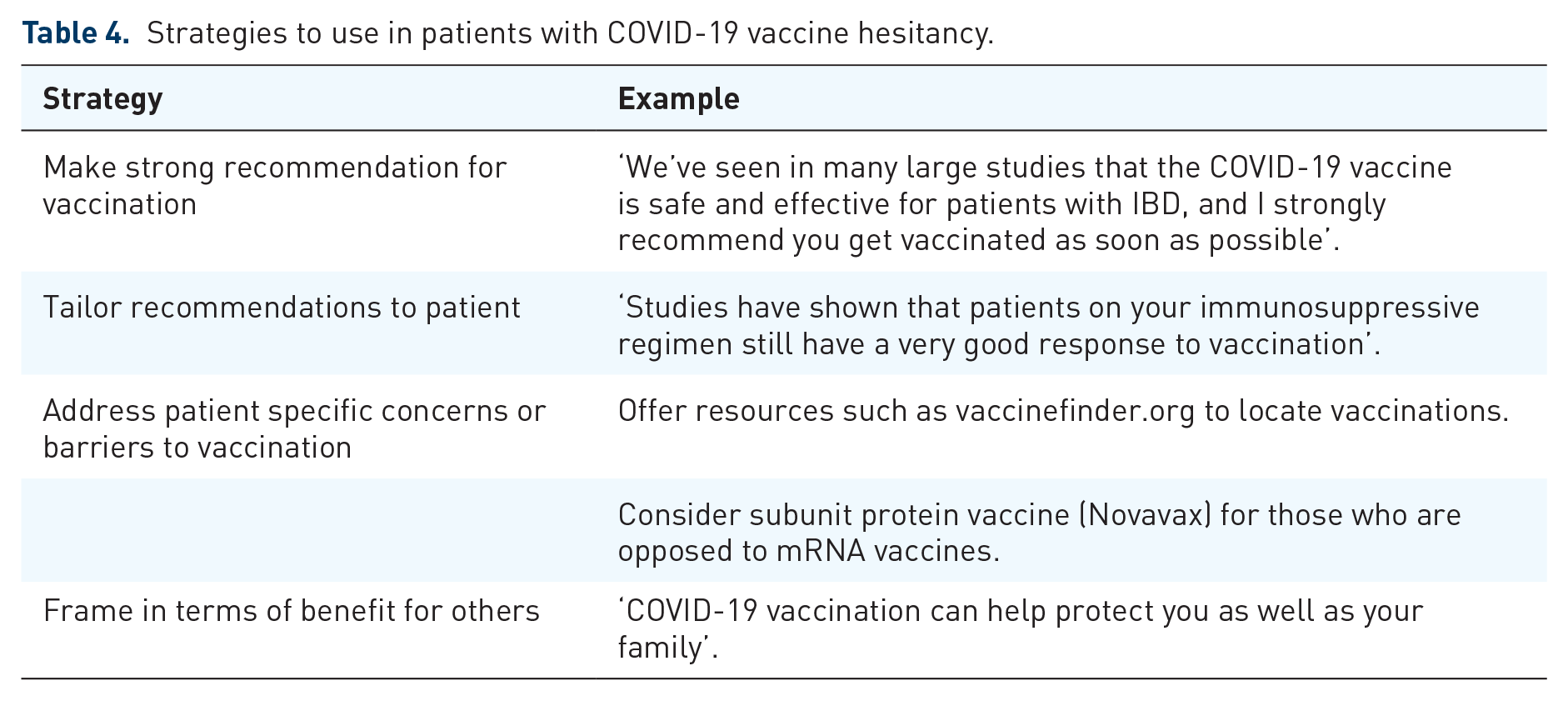
Unfortunately, for many reasons including speed of vaccine development, misinformation and politicization surrounding COVID-19 vaccination, and ‘pandemic fatigue,’ there remain patients with IBD hesitant to undergo vaccination. Providers should play an active role in dispelling misinformation and identifying the source of hesitancy. For those patients wary of mRNA vaccination, providers should consider recommending NVX-CoV2373 (Novavax) either as a primary series or as a monovalent booster. See Table 4 for additional helpful tips on how to increase COVID-19 vaccine uptake.
Strategies to use in patients with COVID-19 vaccine hesitancy.
Providers should reassure patients that, as outlined in this review, vaccines are safe and effective. Because of this high vaccine efficacy even for those on immunosuppressive therapies, currently there is no role for checking antibody levels outside of a research setting. Additionally, vaccines should not be delayed based on medication regimen or timing of biologics. Notably, there has been no correlation between biologic drug levels at time of vaccination and vaccine response. 32
Currently the CDC recommends waiting 3 months after infection prior to vaccination. There is no contraindication to administering the COVID-19 vaccine with other vaccines; however, patients may consider separating the recombinant zoster vaccine and the COVID-19 vaccine due to higher likelihood of systemic adverse effects including malaise and fatigue which have been associated with both vaccines.
Conclusions
Providers and patients should be aware that there is not a greater risk of COVID-19 in patients with IBD, and most patients are not at increased risk of severe disease. Vaccination remains important however as, similar to the general population, severe disease is more common in the unvaccinated, as well as, in those treated with systemic corticosteroids. Thus, efforts should be made to taper corticosteroids as much as possible, but there is otherwise no reason to change effective non-steroid IBD therapies. COVID-19 vaccines are safe and extremely effective, including in patients on immunosuppression. Gastroenterology providers should take an active role in ensuring their patients with IBD are vaccinated against COVID-19.