
Abstract
Background:
Chromoendoscopy is preferred over high-definition white light endoscopy (HDWLE) for dysplasia surveillance in inflammatory bowel disease (IBD) patients, but is more time-consuming to perform and real-world evidence is limited. The prevalence of sessile serrated lesions (SSLs) in IBD patients is also unknown.
Objective:
To determine the yield of polypoid and non-polypoid dysplasia and SSLs in IBD patients undergoing dysplasia surveillance and the associations for these lesions.
Design:
A retrospective cohort study from a tertiary IBD centre.
Methods:
A keyword search of the colonoscopy reporting system was performed. IBD patients with colonic disease that underwent colonoscopy for surveillance between 1 February 2015 and 1 February 2018 were included. Clinical, endoscopic and histopathological outcomes were extracted for the analysis.
Results:
Of 2114 patients identified, 276 eligible colonoscopies in 126 patients were analysed. The median age at colonoscopy was 51 years (interquartile range: 42–58 years). 71/126 (56%) of colonoscopies were performed in male patients, with 57/126 (45%) having ulcerative colitis, 68/126 (54%) Crohn’s colitis and 1/126 (0.79%) IBD-unspecified. The prevalence for any neoplasia was 75/276 (27%). The prevalence for all serrated lesions was 43/276 (16%). Increased age was a risk factor for finding a neoplastic lesion on both univariate and multivariate analyses. Chromoendoscopy was associated with twice the odds of finding a neoplastic lesion (odds ratio: 1.99, 95% confidence interval: 1.13–3.51, p = 0.02), on multivariate analysis. No factor was associated with an increased risk of finding a serrated lesion.
Conclusion:
Significant neoplastic lesions and serrated lesions were detected in 27% and 16% of colonoscopies performed in IBD patients, respectively, with the highest yield in older patients. Chromoendoscopy significantly increased neoplasia yield compared to HDWLE and still has a robust utility in this pragmatic real-world study.
Introduction
Patients with inflammatory bowel disease (IBD) affecting the colon have a higher risk of developing colorectal cancer (CRC) compared to patients without colonic inflammation.1–3 Regular colonoscopies are thus performed for dysplasia surveillance in these patients. 4 In recent years, sessile serrated lesions (SSLs) have been identified as an additional precursor leading to CRC in the general population.5,6 Polyps previously classified ‘hyperplastic’, may, under the 2019 World Health Organization (WHO) criteria have been misclassified, particularly those that were proximal to the splenic flexure and/or greater than 10 mm. We have therefore termed these hyperplastic lesions as ‘Clinically significant serrated polyps’ (CSSPs).7–10
The data on the prevalence of SSLs in IBD cohorts have been contradictory, with reports that IBD cohorts have both higher and lower prevalence of these lesions compared to non-IBD populations.11–13 SSLs have been associated with advanced neoplasia, perhaps even more so than in conventional dysplasia.14,15 The significance of serrated lesions in IBD patients remains to be established, as to whether their occurrence confers a greater malignant potential compared to their occurrence in non-IBD patients. 16 A recent study from Netherlands identified an increased risk of advanced colorectal neoplasia in IBD patients who had dysplastic SSLs and traditional serrated adenomas (TSAs) on the index colonoscopy, but not in patients with non-dysplastic SSLs; however, non-IBD controls were not included for comparison. 17 It is also unknown whether chronic inflammation promotes the development of SSLs and/or conventional adenomas, and, if these are truly observed at a higher frequency in IBD populations.
Colonic IBD patients are at risk of developing both conventional dysplasia, such as tubular adenoma (TA)-like and tubulo-villous adenoma (TVA)-like dysplasia, and non-conventional dysplasia. 14 Non-conventional dysplasia incorporates multiple sub-types: hyper-mucinous dysplasia, crypt cell dysplasia, dysplasia with increased Paneth cell differentiation, goblet cell deficient dysplasia, SSL-like dysplasia, TSA-like dysplasia, and serrated dysplasia not otherwise specified. 15 . Despite being ‘low grade’ in morphology, non-conventional dysplasia appears to have higher malignant potential than conventional dysplasia and therefore requires careful recognition and follow up. 15 Based on pathological studies, IBD patients are at increased risk of acquiring conventional adenomas and SSLs 15 ; however, contradicting real-world data show a lower incidence of these neoplasia in IBD patients also exists. 12 Further clarification of such data would inform gastroenterologists of the benchmark lesion detection rate to aim for when performing colonoscopies in IBD patients and enhance key quality endoscopy indicators in IBD patients.
The evidence would suggest that the yield of chromoendoscopy is considered superior to high-definition white light endoscopy (HDWLE) 18 and it is recommended for dysplasia surveillance in IBD consensus guidelines.19–25 More recent data have shown mixed results, with HDWLE potentially rivalling the results obtained with chromoendoscopy.26–28 High-definition chromoendoscopy has performed better than HDWLE alone, when conditions were optimal for chromoendoscopy18,27,29; however, there are also real-world data and results of meta-analyses that contradict these observations.30,31 Poor adherence to chromoendoscopy recommendations for various factors such as inexperience and perceived time constraints limit its use. 32 Thus, there is a need for more real-world results on how the yield of chromoendoscopy with HDWLE compare with HDWLE alone in the surveillance of IBD patients.
Aims
We conducted a pragmatic real-world study with the primary aim of determining the yield of any significant lesions (ASLs, defined as polypoid and/or non-polypoid/flat dysplasia and SSLs including CSSPs) during colonoscopies performed for the primary intention of dysplasia surveillance in a cohort of tertiary IBD patients. The secondary aim was to identify the clinical predictors for neoplasia yield, with a focus on whether chromoendoscopy with HDWLE conferred a higher neoplasia yield.
Materials and methods
Inclusion criteria
The study was performed and reported in concordance with the STROBE guidelines. 33 Patients were included if they had a definite diagnosis of Crohn’s disease (CD) with colitis, ulcerative colitis (UC) or IBD-unspecified with colonic involvement for greater than 8 years. Complete colonoscopies performed with patient consent at the inception date for the purpose of dysplasia surveillance and any subsequent follow-up colonoscopies were included. A complete colonoscopy was considered one where caecal intubation occurred. Thus, those with stricturing disease were only included if strictures were passable and complete intubation to the caecum was achieved.
Patients were excluded if they had no formal IBD diagnosis, had an inadequate bowel preparation (as defined by the Aronchick scale ‘inadequate or poor’ 34 ), had isolated proctitis or isolated ileal CD. Patients who had macroscopically active inflammation evident on colonoscopic insertion, did not undergo chromoendoscopy. Instead, HDWLE was performed and standard segmental biopsies were taken as described below. Virtual chromoendoscopy (VCE) was not utilised during the study period as recommended by the SCENIC guidelines 19 at that time.
Clinical disease-related factors and demographics were extracted from a prospectively maintained IBD clinical registry. Colonoscopies were all performed by gastroenterologists, with the majority being subspecialist IBD physicians who have had specific training in chromoendoscopy. Patients that were allocated to a gastroenterologist list not trained in chromoendoscopy had, by default, HDWLE performed, with standardised biopsies taken in every segment which approximates to 4 biopsies for every 10 cm or 32 biopsies per colonoscopy.
Patients were selected consecutively following a keyword search on the hospital endoscopy reporting database, from 1 February 2015 to 31 January 2018. Search terms came from a free-text field, and typographical errors accounted for. Search terms used were as follows: ‘chromoendoscopy’, ‘chromo’, ‘chormo’ (to account for spelling errors), ‘blue’, ‘indigo’, ‘carmine’, ‘dysplasia’ and ‘surveillance’. The colonoscopy indication was searched using the terms, ‘f/u colitis or f/u Crohn’s disease’. Patients were followed for a minimum of 36 months and up to 72 months for additional follow-up colonoscopies via a chart review. Colonoscopies repeated for the same patient up to 31st of January 2021 were included in the study sample. All included patients had complete data for the variables of interest in this study.
Definitions
In this study, given the inclusion of cases prior to the change in definition of serrated lesions in the WHO 2019 guidelines, 35 we defined ‘CSSPs’ as any hyperplastic polyps greater than 10 mm in size and/or proximal to the splenic flexure. ASL was defined as the total of any polypoid or non-polypoid flat dysplasia (including TAs, TVA, villous adenoma, traditional serrated adenomas (TS)), SSLs, and CSSPs. Invisible flat dysplasia was defined as dysplasia that was not identified on chromoendoscopy or HDWLE but on histopathological examination of a biopsy specimen. As prior areas of colonic inflammation were not always described, the focus of the study was on the totality of all neoplastic lesions rather than specific dysplastic lesions derived from areas previously affected by colitis. Colitis-associated dysplastic lesions specifically were impossible to determine retrospectively for all patients due to do endoscopists’ reporting variability.
Chromoendoscopy method
The chromoendoscopy was performed using high-definition colonoscopes (Olympus 190-series). We used methylene blue (1%, 5 ml ampoule diluted in 250 ml of water) or indigo carmine at a concentration of 0.5% administered via the foot pump. Targeted biopsies were taken of suspicious lesions and routine biopsies were taken of each segment to determine histological activity. Where possible, polypoid adenomatous-like lesions were resected whole or piecemeal with four peri-polyp biopsies taken of the flat mucosa around the polyp. Piecemeal resections were followed up with another colonoscopy to ensure complete resection within 3–6 months. Patients who only underwent a colonoscopy with HDWLE without chromoendoscopy had visible polyps removed and random biopsies taken at each colonic segment. Patients with a significant amount of active colitis did not undergo chromoendoscopic examination.
Statistical analysis
SPSS version 20 was utilised for statistical analysis. Tests for normality were performed. Medians were reported for non-parametric variables. Univariate and multivariate logistic regression analyses were performed to determine the predictors for finding neoplasia. The covariates of interest included in the multivariate model were those known to influence neoplasia risk, or if the univariate analysis yielded a two-sided p value < 0.2 for an increased risk of finding neoplasia. Covariates with a two-sided p > 0.05 were removed in a stepwise manner leaving only the significant factors at the end of multivariate adjustment.
Results
Baseline characteristics
In all, 2114 patients were identified from the reporting search. In total, 276 eligible colonoscopies in 126 patients were available for analysis after meeting the inclusion and exclusion criteria. Summary results are reported ‘per colonoscopy’. Figure 1 describes the criteria for case inclusion.

Case selection flow diagram.
Table 1 summarises the complete results for baseline patient characteristics. The median age at colonoscopy was 51 years [interquartile range (IQR): 42–58 years]. 71 of 126 (56%) of colonoscopies were performed in male patients, with 57 of 126 (45%) having UC, 68 of 126 (54%) CD and 1 of 126 (0.8%) IBD-unspecified. The median disease duration at the time of the colonoscopy was 16 years (IQR 12–23 years). 15 of 126 (12%) of patients had a family history of CRC and 10 of 126 (7.9%) had primary sclerosing cholangitis (PSC). One patient had a personal history of colonic polyps prior to IBD dysplasia screening commencing. 151 of 276 colonoscopies (55%) were performed with chromoendoscopy and targeted biopsies (±random biopsies) and the rest were performed with HDWLE with random segmental biopsies. 41 of 276 (15%) colonoscopy specimens had active histological inflammation on biopsies. 24 (8.7%) patients were on steroids at the time of procedure, 13 (4.7%) of which still proceeded to chromoendoscopy. The reasons for corticosteroid exposure at the time of the colonoscopy were mixed and variably reported on chart review. Most patients were on a short weaning course of prednisolone to ensure mucosal inflammation at the time of colonoscopy was minimal to maximise chromoendoscopy potential; with a few having had a flare of their IBD prior to their planned surveillance procedure.
Baseline characteristics.

1SSLs and CSSPs, TSAs total.
2Pre-WHO criteria change in 2019. 10
CD, Crohn’s disease; CSSPs, clinically significant serrated polyps; IQR, interquartile range; SSL, sessile serrated lesion; TSA, traditional serrated adenoma; TVA, tubulo-villous adenoma; UC, ulcerative colitis.
Prevalence of neoplasia
The prevalence for ASLs was 75 of 276 colonoscopies (27%), an SSL was found in 20 of 276 colonoscopies (7.2%) and any serrated lesion (SSL, TSA or CSSP) was found in 43 of 276 colonoscopies (16%). No SSLs were found to be dysplastic. The histological breakdown of all lesions identified is summarised in Table 1. Importantly, no flat invisible dysplasia was detected (from random biopsies taken) in the entire cohort. Visible flat (non-adenomatous like) dysplasia or cancer was found in 4 of 276 colonoscopies (1.4%), and all 4 were detected in colonoscopies performed with chromoendoscopy and targeted biopsies. One of these patients had PSC and visible low-grade flat dysplastic changes on two sequential, annual colonoscopies, but was not further surveyed with subsequent colonoscopies due to a concurrent advanced cholangiocarcinoma. The second patient had a family history of bowel cancer and was an ex-smoker, with cancer being identified on a surveillance colonoscopy after having continuously active disease in the preceding year. The third patient had refractory inflammatory disease but no additional risk factors for malignancy. On two prior colonoscopies not included in the study time frame, he had multifocal flat low-grade dysplasia and on the third, and included colonoscopy, he progressed to multifocal high-grade dysplasia on histopathological examination that ultimately culminated in him having a colectomy.
Predictors for ASL and any serrated lesions
Any significant lesions (ASL)
Table 2 summarises the univariate and multivariate findings for any significant neoplastic lesions. The univariate analysis found that an increased age [odds ratio (OR): 1.03, 95% confidence interval (CI): 1.01–1.05, p = 0.02] was associated with a higher risk of finding ASL. Chromoendoscopy was associated with a non-significantly increased risk of detecting ASL compared to those who did not undergo chromoendoscopy (OR: 1.61, 95%: CI: 0.94–2.74, p = 0.08) on the univariate analysis.
ASL univariate and multivariate analyses.
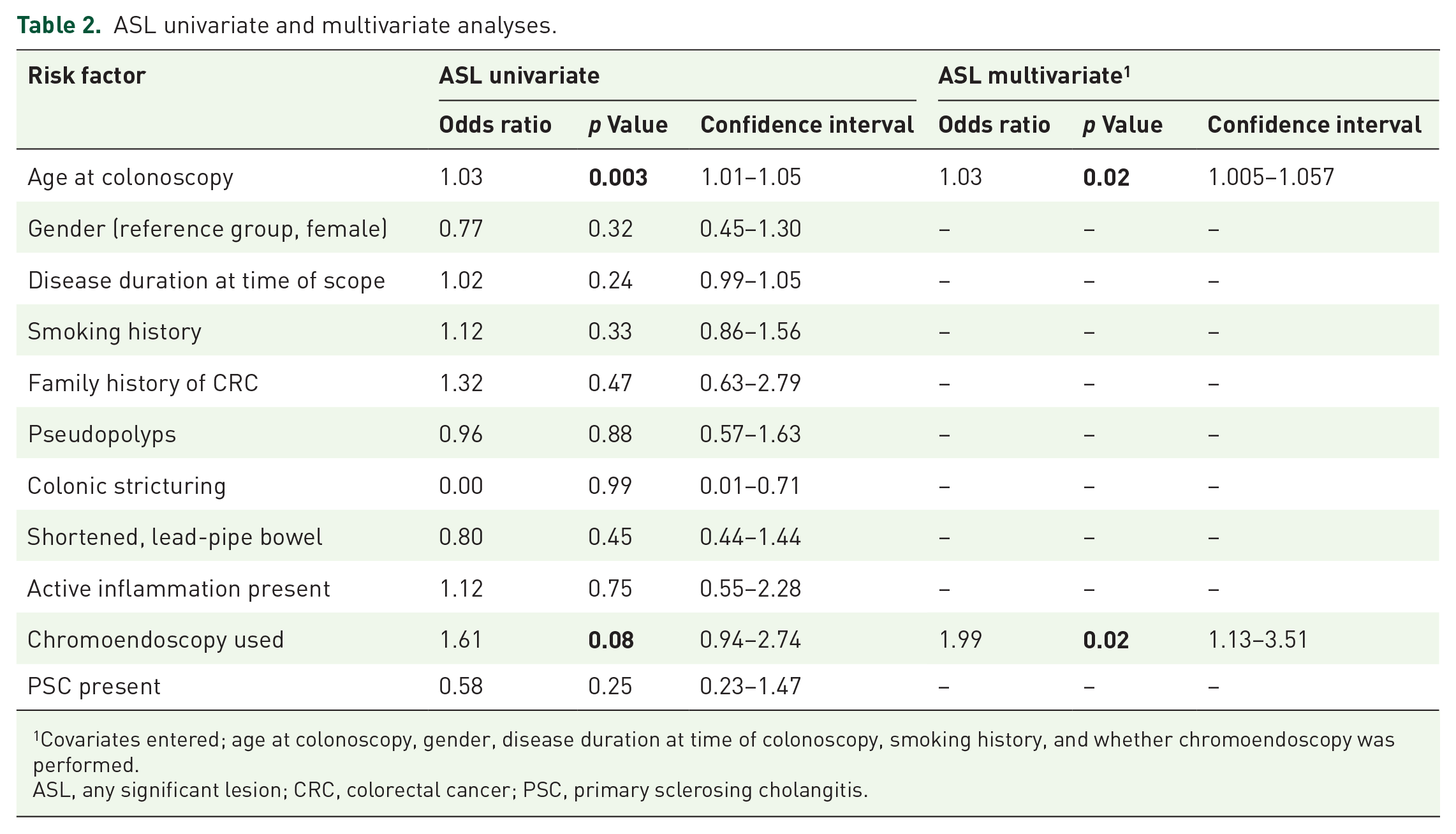
1Covariates entered; age at colonoscopy, gender, disease duration at time of colonoscopy, smoking history, and whether chromoendoscopy was performed.
ASL, any significant lesion; CRC, colorectal cancer; PSC, primary sclerosing cholangitis.
The covariates that were entered into the multivariate logistic regression analysis included age at colonoscopy, gender, disease duration at time of colonoscopy, smoking history, and whether chromoendoscopy was performed as these either had a p value of <0.2 at univariate analysis or are known to be associated with neoplasia development in non-IBD cohorts. After adjusting for these covariates, a similar narrative was seen on the multivariate analysis whereby an increased age (OR: 1.03, 95% CI: 1.005–1.057, p = 0.02) was associated with a higher risk of finding neoplasia. In addition, chromoendoscopy was found to confer twice the odds of finding any neoplasia than if chromoendoscopy was not performed (OR: 1.99, 95% CI: 1.13–3.51, p = 0.02), Table 2.
Any serrated lesions (any of SSL, TSA or CSSP)
The univariate analysis revealed that chromoendoscopy was once again numerically associated with an increased odds of serrated lesion detection; however, it did not reach statistical significance (OR: 1.68, 95% CI: 0.94–2.75, p = 0.08). The multivariate analysis did not find any risk factors associated with serrated lesion detection (Table 3).
Univariate and multivariate analyses for finding any serrated lesions.

CRC, colorectal cancer; PSC, primary sclerosing cholangitis.
Discussion
Colonic inflammatory disease is an established risk factor for CRC.1–3 This risk begins at approximately 2% after 8 years and increases at approximately 0.5–1% per year of disease. There is also an increased risk with a greater extent of colonic involvement.1,22,36,37 Concomitant PSC, being a smoker, an older age, the presence of colonic strictures and a family history of colorectal carcinoma are also known risk factors for a higher incidence of CRC in inflammatory colitis patients.3,22,36,38–41 Active inflammation has been shown to be a driver of carcinogenesis in IBD.42,43 Chronic inflammatory burden, however, is difficult to quantify. Surrogate clinical markers of more active disease may include the need for higher intensity immunosuppressive treatments and a longer disease duration.39,44 It is unknown if chronic inflammation also drives the development of conventional adenomatous neoplasia and SSLs in IBD patients. The existing literature comparing the prevalence of neoplasia in IBD patients with the general population is sparse, as comparative studies are difficult to conduct. Real-world studies on the prevalence of neoplasia in the IBD surveillance cohort show mixed and contradictory results.12,15,17 Thus, further study is needed to determine neoplasia detection rates in surveillance colonoscopies performed in IBD patients and to determine if chromoendoscopy, in the era of HDWLE, increases the yield of neoplasia.
Our study identified the prevalence of ASL to be 27% and any serrated lesion to be 16% of colonoscopies performed in a tertiary IBD surveillance cohort. Our results are in line with previous studies reporting neoplasia detection rates of 13–59% in IBD populations.12,29,45 Age was associated with a higher risk of finding ASL statistically, as did the utilisation of chromoendoscopy. Our findings add weight to the existing literature that chromoendoscopy increases neoplastic yield in surveying IBD patients despite the skill, endoscopy time and therefore costs incurred.
Serrated polyposis syndrome is now the most common polyposis syndrome, and serrated polyps have been identified in 15–27% of a non-IBD, CRC screening cohort. 46 In our IBD cohort, serrated lesions were seen in 16% of the cohort, with 7.2% having an SSL by the WHO definition pre-dating the 2019 change. 35 Previous published studies have found the prevalence of SSLs in IBD cohorts to vary. Johnson et al. 11 and Lee et al. 12 have found it to be lower than the general, non-IBD population at 0.2–1.4%; however, these results were prior to the WHO definition alteration for SSL in 2019, and may have under-estimated the true prevalence of SSLs. On the other hand, Iacucci et al. in 2014 identified the incidence of SSLs in IBD patients to be similar to our rate at 16%. 13 Whether there is an increased prevalence of SSLs in the IBD population compared to the general population remains unanswered as there are no prospective studies comparing the yield of chromoendoscopy in an IBD cohort matched with a non-IBD or average risk cohort. These results show our IBD cohort to have at least similar rates of serrated lesions as population studies of non-IBD patients and concur with other studies of serrated lesion prevalence in IBD patients. 13 Gastroenterologists performing surveillance colonoscopies in IBD patients should therefore aim for similar serrated lesion detection rates, despite the younger median age of the IBD cohort.
Chromoendoscopy is regarded as the gold-standard for dysplasia detection in IBD 19 ; however, excellent bowel preparation and adequate time allocation are paramount. In our cohort, all colonoscopies were performed with high-definition white light colonoscopes, which have been shown to improve dysplasia detection compared to standard definition colonoscopies. 19 Chromoendoscopy was performed in 55% of the cohort, with bowel preparation quality and macroscopically visible inflammation being the main drivers for not proceeding with the chromoendoscopy. Our results intimate in favour of chromoendoscopy over white light examination in concordance with results that have been published elsewhere.27,29 Our relatively small cohort and possibly underpowered sample size still detected a significant benefit in detecting any significant lesions with twice the odds of finding a lesion compared to if chromoendoscopy was not used. VCE is not performed at our centre; however, the technology continues to evolve in this area and data are mixed to date, but holds promise.47,48
A strength of this study was the real-world nature of the data acquired. The pragmatic nature of our results offers great relevance to the practising gastroenterologist dealing with IBD patients. Data were extracted from electronic medical records and a prospectively maintained registry that was up to date and considered complete. This study was carried out in a busy tertiary IBD centre with a cohort of patients that had multiple years of follow-up. The retrospective nature also removes the effect of observer bias which might confound prospective open label studies in endoscopy and demonstrate that despite the challenges of time restriction in real-world clinical practice, chromoendoscopy can be still be performed successfully with a high yield.
Several limitations in this study should be acknowledged. First, data were retrospectively accessed, introducing the risk of information as well as selection bias. Free-text reporting in colonoscopy reports limited the ability to remove information bias. Importantly, we lacked details surrounding previously affected areas of colitis to differentiate colitis-associated dysplasia and spontaneous adenomas. We felt, however, the pragmatic nature of the study made this lack irrelevant, as the totality of all lesions detected was the focus of this study. Second, no specific data were expressly collected regarding specific endoscopist factors, but all were specialist gastroenterologists, and the majority sub-specialised in treating IBD. The number of random biopsies taken, however, were variable among the endoscopists, which may have influenced the yield of invisible dysplasia, albeit insignificantly. Third, inter-observer variability in neoplasia detection rates requires consideration. Fourth, our cohort was relatively small thus the magnitude of any findings may have been diminished from being underpowered. Finally, pathology definitions for SSLs are continuing to evolve, with the most recent change being in 2019. 35 This change corresponds to variability in histopathology reporting between 2015 and 2021, a significant time segment of our cohort. Funding was not available to enable histopathologists to retrospectively review the specimens; thus, we utilised the expanded definition of CSSP to account for the potentially misclassified lesions according to current definitions.
Conclusion
Significant neoplastic lesions were detected in 27% and serrated lesions in 16% of all colonoscopies in IBD patients undergoing a dysplasia surveillance program. Our data add to the literature on the expected neoplastic yield targets when surveying a patient with colonic IBD and supports the practice of performing chromoendoscopic surveillance.
Supplemental Material
sj-docx-1-tag-10.1177_17562848231167280 – Supplemental material for The yield of dysplasia and serrated lesions in a single-centre tertiary inflammatory bowel disease cohort
Supplemental material, sj-docx-1-tag-10.1177_17562848231167280 for The yield of dysplasia and serrated lesions in a single-centre tertiary inflammatory bowel disease cohort by Fiona Yeaman and Lena Thin in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.