
Abstract
Objective
Our aim was to prospectively assess bowel preparation in patients with inflammatory bowel disease (IBD) and to determine the impact of disease-related factors on preparation efficacy because few studies have addressed this issue.
Methods
We conducted a retrospective analysis of data collected from a cohort of patients with IBD enrolled at a tertiary center in Bucharest, Romania. Patients were evaluated every 12 months, with each study visit including collection of clinical, biological, and endoscopic data. We reviewed 348 colonoscopies from 169 consecutive patients prospectively followed for a median length of 2 (0–6) years.
Results
The median total Boston score and median score per bowel segment in our cohort were optimal at 6 (range 0–9) and 2 (maximum 3), respectively. There was no difference in bowel preparation between patients with endoscopic activity and patients with mucosal healing (median total Boston score 6). Disease- and patient-related parameters did not influence the quality of bowel preparation.
Conclusions
The quality of bowel preparation in patients with IBD was optimal for our cohort, and disease-related parameters did not significantly influence preparation efficacy.
Keywords
Introduction
Colonoscopy is indispensable in the management of inflammatory bowel disease and constitutes a critical tool for diagnostic and therapeutic decision-making. Colonoscopy is mandatory for initial diagnosis, monitoring the response to therapy, and colorectal cancer (CRC) surveillance. 3 Endoscopic examination is considered safe and has a low rate of adverse events, although the burden of bowel preparation and investigation in patients with inflammatory bowel disease (IBD) remain intractable issues. 4 Considering that patients with IBD undergo multiple endoscopies during their lifespan and that each of these investigations is of paramount importance for disease management, the evaluation of quality indicators is imperative.
Over the last decade, more than 40 performance measures have been identified; current European guideline recommendations comprise seven quality parameters, including the rate of adequate bowel preparation. Inadequate bowel preparation results in increased costs and inconvenience as the procedure has to be rescheduled or alternative investigations are needed. 5
Predictors of inadequate bowel preparation include patient-related factors (advanced age, male sex, obesity, previous inadequate bowel preparation, constipating medications), associated comorbidities (diabetes mellitus, stroke, dementia, Parkinson disease), and improper patient instruction (poor adherence to instruction, timing of purgative administration, waiting times for colonoscopy).6–8
Most published studies on poor bowel preparation have not evaluated the impact of concomitant conditions, such as IBD, on bowel preparation quality.1,2 When evaluated, there is no difference in preparation quality between patients with and without IBD. 9 The main objective of this study was to assess bowel preparation in patients with IBD and to determine the impact of disease-related factors on preparation efficacy.
Methods
Patients and methods
We conducted a retrospective analysis of data collected from a cohort of patients with IBD enrolled at a referral center for IBD (Colentina Clinical Hospital, Bucharest) from January 2013 to December 2018. We conducted a retrospective analysis of data collected in an observational study conducted among a cohort of patients with IBD at a tertiary center. The study was approved by the institutional review board. Informed consent was obtained from each patient.
All patients with a confirmed diagnosis of Crohn’s disease (CD) or ulcerative colitis (UC) who were older than 18 years of age were invited to participate in a cohort study, with annual visits for the assessment of disease activity, including colonoscopy. The diagnosis of IBD was based on clinical, endoscopic, and histological criteria, in accordance with existing guidelines. 10 Participants were evaluated every 12 months unless a relapse occurred, in which case unscheduled visits took place at the discretion of the attending physician. Each study visit included data collection and adjustment of treatment, if necessary. The main data collected were age; sex; smoking status; medical treatment; disease duration; and clinical, endoscopic and histological findings at the time of diagnosis and at subsequent visits. Additionally, patient quality of life was assessed at each study visit using the Short Inflammatory Bowel Disease Questionnaire. Summarized study activities are found in Figure 1.
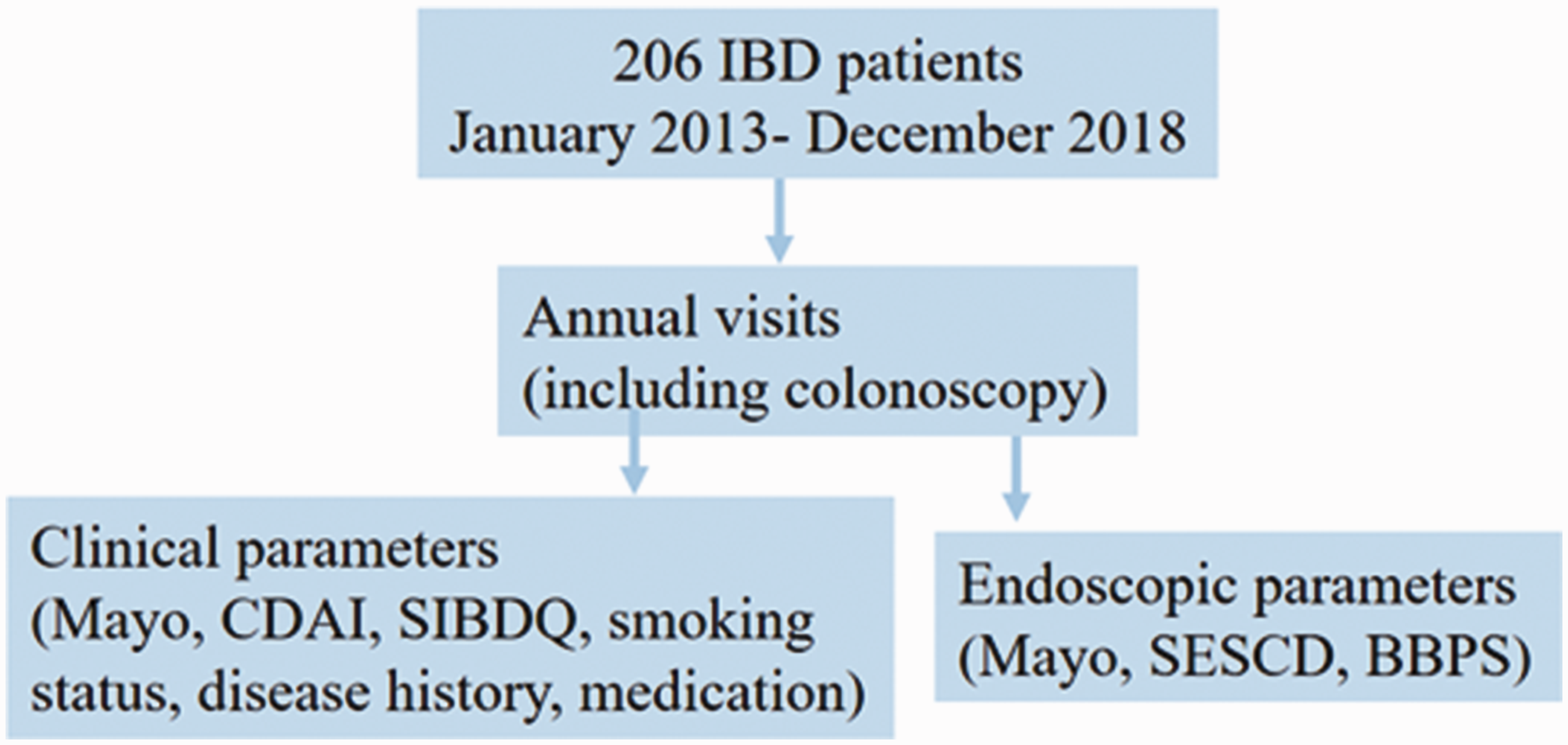
Summarized research activities.
Patients with a history of surgery for IBD, important comorbidities (cardiovascular, neurologic, renal, pulmonary or hepatic disease), and patients who could not undergo complete colonoscopy (i.e., because of severe disease activity or the presence of critical strictures in the colon) were excluded from this analysis.
Evaluation of disease activity
Colonoscopies were performed by four gastroenterologists with experience in IBD, using conscious sedation with midazolam at the discretion of the endoscopist. Disease activity was objectively assessed using C-reactive protein (CRP) measurement, the Mayo score, Crohn’s Disease Activity Index score, and Simple Endoscopic Score in Crohn’s Disease (SESCD). Mucosal healing was assessed using strict criteria, namely, a Mayo endoscopic subscore of 0 for patients with UC and a SESCD score of <3 for patients with CD.
Bowel preparation
Patients followed a low-fiber diet 2 days before colonoscopy and a split regimen of 4 L of polyethylene glycol (PEG) solution (or a same-day regimen in the case of an afternoon colonoscopy) for bowel preparation, such that the time elapsed between the last dose of bowel preparation solution and the colonoscopy did not exceed 4 hours, as per recommendations of the European Society of Gastrointestinal Endoscopy. 11 The Boston bowel preparation scale (BBPS) was used to assess the quality of bowel preparation. This analysis included colonoscopies with BBPS scores ranging from 0 to 9.
Statistical analysis
All statistical analyses were performed using IBM SPSS version 20.0 for Windows (IBM Corp., Armonk NY, USA). Statistical analysis of the study data was performed by a biomedical statistician. Data analysis included descriptive statistics computed for continuous variables, including mean and standard deviation (SD). The comparison of clinical characteristics was performed using the chi-square test and independent t-test for continuous variables with normal distributions. Correlations between parameters were evaluated using Pearson correlation for continuous variables and the Spearman correlation coefficient for discrete variables. Linear regression analysis was used to determine the influence of different patient- and disease-related parameters on bowel preparation quality. The accepted significance level was a p-value <0.05.
Results
Patient demographic details are shown in Table 1. In total, 206 patients were enrolled in our study between 2013 and 2018 and were prospectively followed for a median of 2 (0–6) years. From 206 patients included in the cohort study, 169 patients (59 with CD, 110 with UC) totaling 348 study visits were included in this analysis. The sex distribution was relatively even and the mean patient age was 40 years (standard deviation 14.5 years); 71% of patients were active smokers at the time of their study visit. Regarding the extent of disease, according to the Montreal classification, 22 patients with UC (13%) had proctitis, 29 (17%) had left colitis, and 49 (29%) had extensive colitis. Among patients with CD, 16 (9%) had ileal disease only, 31 (18%) had colonic disease, and 17 (10%) had ileocolonic disease.
Characteristics of patients with inflammatory bowel disease at baseline.
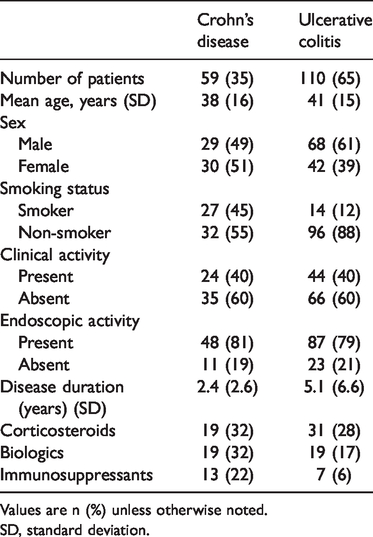
Values are n (%) unless otherwise noted.
SD, standard deviation.
Patient-related parameters and bowel preparation
Sex, smoking status, disease type (CD or UC), disease duration, ongoing treatments, and CRP levels did not influence bowel preparation quality (Table 2).
Influence of patient- and disease-related parameters on bowel preparation quality.

Disease activity and bowel preparation
The median total Boston score for all patients was 6 (≥6 is considered optimal; the maximum score is 9), and median scores per segment were 2 (left colon), 2 (transverse colon), and 2 (right colon); scores ≥2 per segment are considered optimal (the maximum is 3).
The percentage of patients with suboptimal bowel preparation was 28% (Boston score <6). Boston scores for each colon segment are shown in Table 3. At baseline, 88 (54%) of patients had clinical activity, and 134 (81%) had endoscopic activity. With respect to disease severity at baseline, 9.6% of patients with CD had an SESCD score >15, and 11.2% of patients with UC had a Mayo endoscopic score of 3 (indicating severe endoscopic activity).
Boston scores for each colon segment.

The percentage of patients in clinical remission improved over time (46% at the first visit vs. 68% at the second visit; p < 0.05, Mann–Whitney U test), and mucosal healing rates were significantly higher at subsequent study visits (19% at the first visit vs. 27% at the second visit; p < 0.05, Mann–Whitney U test).
Patients with endoscopic activity had the same median total Boston scores as patients with mucosal healing (median total Boston score of 6 in both groups; p < 0.01 Mann–Whitney U test). Disease extent, disease severity, and clinical activity did not influence the quality of bowel preparation in patients with UC in the chi-square test.
Additionally, in patients who did not have IBD undergoing colonoscopy in our unit, the median overall BBPS scores were the same as in patients with IBD (median BBPS score of 6 for 210 consecutive analyzed procedures).
Bowel preparation at follow-up colonoscopies
Each patient underwent an annual endoscopic evaluation (and additional evaluations in the case of relapse). We registered two study visits for 86 patients, three for 44 patients, four for 27 patients, five for 13 patients, and six for 8 patients. No correlation was found between BBPS and the number of follow-up study visits using Spearman correlation.
The median total Boston score of 6 remained the same at follow-up visits, as did the median scores per segment (score of 2 for each segment). Variation in the total Boston score over time is shown in Figure 2.

Variation in Boston score over time.
Discussion
Colonoscopy plays a crucial role in the management of IBD, as part of the initial diagnostic work-up and as part of the assessment of disease activity over time, guiding therapeutic decisions and facilitating cancer surveillance in patients with long-standing IBD. Considering neoplasia surveillance colonoscopies alone for an average 40-year-old patient in the low-risk category, at least six colonoscopies are expected during the patient’s lifespan.12,13 Suboptimal bowel preparation is a leading cause of missed lesions, repeat procedures, and increased overall procedure-related costs. 14 Thus, adequate bowel preparation is one of the main quality indicators for colonoscopy, as recommended by the current guidelines. 5
Our study is among largest reports on the efficacy of bowel preparation in a cohort of patients with IBD. Furthermore, owing to the availability of multiple colonoscopies at different time points, we were able to analyze the relationship between disease activity and bowel preparation in a very thorough manner. Our results indicate that bowel preparation was adequate in a large number of patients (with 72% having a BBPS of at least 6), in accordance with the current guidelines. 1 In addition, there was no difference in the quality of BP between patients with active disease and those with mucosal healing, suggesting that optimal preparation is possible even in patients with poor disease control.
These findings are in accordance with previously published data. 4 Reported predictors for poor bowel preparation in the general population, such as advanced age and male sex, 8 were not found to be relevant predictors in this study. Patient-related parameters, including age, sex, and smoking status, did not influence bowel preparation.
A notable result concerns BBPS scores not changing over time, with follow-up visits showing consistently good bowel preparation scores. This is an important finding because patient compliance with multiple colonoscopies can be expected to decrease, leading to suboptimal bowel preparation at subsequent visits.
A study investigating the burden of elective colonoscopy by examining specific variables, such as taste, volume, or social dimension, identified a negative impact on more than 20% of patients. 6 However, a study targeting patients with IBD found that most patients considered colonoscopy bearable and would have the procedure as frequently as required if their physician felt it appropriate, 15 which seems to be consistent with the findings in our cohort in which patient compliance was quite high and stable over time. Perceived doctor–patient relationship and satisfaction should be examined in further studies, to improve patient compliance and overall primary care. 16
A few remarks are necessary regarding study limitations. The main limitation is that the patients with IBD in our cohort study were evaluated using a clear and strict study protocol (including standard bowel preparation with high-volume PEG solution), which might not accurately reflect daily practice in real life. Furthermore, we could not investigate the impacts of comorbidities and polypharmacy on colon cleansing, which are factors that have a negative impact. 7 These categories of patients were excluded from our study. Additionally, patients with a history of IBD-related surgery were excluded, which might influence the rate of adequate bowel preparation because published data suggest that a history of abdominal surgery is a risk factor for poor preparation.17,18
Despite these limitations, we believe that our study presents robust data in support of patients with IBD being able to be adequately prepared for colonoscopy using standard bowel preparation regimens and that disease activity does not negatively impact the success of bowel preparation.
In conclusion, patients with IBD should not be regarded as a difficult subgroup of colonoscopy patients, even when considering multiple successive examinations during the course of their disease.