
Abstract
Background:
Patients with isolated anastomotic lesions (iAL) are common in postoperative Crohn’s disease (CD) and have heterogeneous prognosis.
Objectives:
To investigate the prognostic value of neutrophil-to-lymphocyte ratio (NLR) in CD patients with iAL.
Design:
A bicenter retrospective cohort study.
Methods:
CD patients who received ileocolonic resection from 2013 and 2020 and had a modified Rutgeerts score of i2a were recruited. NLR was determined within 1 week around the initial endoscopy after ileocolectomy. The primary outcome was clinical recurrence. Kaplan–Meier method and Cox hazard regression analysis were utilized to assess the association between candidate variables and outcomes of interest.
Results:
In total, 411 postoperative CD patients were preliminarily reviewed and 83 patients were eligible. In total, 36 (48.6%) patients experienced clinical recurrence with a median follow-up time of 16.3 (interquartile range, 9.7–26.3) months. NLR > 2.45 and age at surgery >45 years had higher cumulative incidence of clinical recurrence in the Kaplan–Meier analysis. After adjusted for potential confounders, NLR > 2.45 was the only independent risk factor for clinical recurrence, with an adjusted hazard ratio (HR) of 2.88 [95% confidence interval (CI), 1.39–6.00; p = 0.005]. Furthermore, a risk score based on NLR and age at surgery were built to further stratify patients. Compared to those who scored 0, patients with a score of 1 and 2 had an adjusted HR of 2.48 (95% CI, 1.22–5.02) and 6.97 (95% CI, 2.19–22.16) for developing clinical recurrence, respectively.
Conclusions:
NLR is a promising prognostic biomarker for CD patients with iAL. The utilization of NLR and the risk score to stratify patients may facilitate the personalized management in patients with iAL.
Keywords
Introduction
Crohn’s disease (CD) is a relapsing and chronic inflammatory disease which could affect the whole gastrointestinal tract. 1 More than 50% of CD patients, during the whole disease course, suffer from severe complications and require intestinal resection. 2 However, surgical therapy can rarely cure CD and new lesions can be observed by endoscopy within weeks of resection. The early endoscopic lesions in the neo-terminal ileum and anastomosis can predict the clinical progression when classified by Rutgeerts score. 3 According to Rutgeerts score, patients with no or <5 aphthous lesions in the neoterminal ileum are associated with having good prognosis, while those with diffuse inflammation or large ulcers are likely to develop rapid postoperative recurrence. Nevertheless, the prognosis of patients with isolated anastomotic lesions (iAL), which account for around 20% of all postoperative patients, is heterogeneous.4,5 It is still an intractable problem for clinicians to identify the patients with high risk for recurrence and perform personalized managements for patients with iAL. Therefore, it is important and urgent to discover reliable prognostic factors to stratify these patients and then to tailor approaches for postoperative recurrence prophylaxis.
Neutrophil-to-lymphocyte ratio (NLR) is a non-invasive, easily accessible biomarker that can reflect disease activity and provide information of prognosis in numerous inflammatory diseases.6–8 In CD, NLR is demonstrated to be a promising biomarker for predicting disease relapse, treatment escalation, and response to biologics therapy. 9 Moreover, NLR can predict postoperative complication in CD patients with intestinal resection. 10 However, it is still unknown whether NLR has prognostic value in postoperative CD patients with iAL.
Therefore, we conducted a bicenter cohort study to evaluate the ability of NLR for predicting postoperative recurrence in CD patients with iAL. Moreover, we developed a risk score including clinical characteristics and NLR to facilitate the stratification of patients with iAL.
Materials and methods
Study population
This was a bicenter retrospective cohort study, consecutively recruiting CD patients who received elective ileocolectomy and anastomosis in the First Affiliated Hospital of Sun Yat-sen University or the Sixth Affiliated Hospital of Sun Yat-sen University, from January 2013 to December 2020. Other inclusion criteria included the following: (1) patients with diagnosis of CD based on clinical manifestations, ileocolonoscopic, histopathologic, as well as radiologic evidences; (2) an initial endoscopy performed after ileocolectomy and showed iAL with or without <5 aphthous lesions at the neo-terminal ileum (equal to i2a in modified Rutgeerts score 11 ); (3) data of NLR were available within 1 week around the initial endoscopy; and (4) a recorded follow-up time of at least 3 months. Patients were excluded if they suffered postoperative infection or combined with other autoimmune diseases.
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. 12
Demographic and clinical characteristics
Demographic and clinical characteristics collected at baseline included sex, age at diagnosis, age at surgery, disease location, disease behavior, the presence of perianal involvement, CD-related surgical history, and smoking status. Montreal classification 13 was applied to categorize patients by disease location and behavior. Medications after the initial endoscopy were recorded and divided into three groups, unmedicated (no steroid, immunosuppressants, or biologics used before the event or the end of follow-up), immunosuppressant treated (a continuous use of immunosuppressants with or without 5-aminosalicylic acid), and biologics treated (application of biologics with or without immunosuppressant) for further analysis.
NLR
The blood sample was obtained within 1 week around the initial endoscopy procedure after the ileocolectomy. The detection of complete blood count was performed according to the standard scheme in the laboratory of the corresponding hospital. The prognostic value of primordial variable including serum neutrophil, lymphocyte, monocyte, and albumin concentration was assessed. Results revealed that only binarily categorized neutrophil and lymphocyte counts were significantly correlated with clinical prognosis (Supplemental Table 1). Given the inverse correlation between clinical prognosis and these two indicators, the ratio of them, NLR, was calculated and evaluated in the further analyses. NLR was calculated as follows:

Outcomes
The primary outcome of this study was clinical recurrence, which was defined as any occurrence of hospitalizations for disease exacerbation, medication escalation, re-operation, or endoscopic recurrence. Medication escalation included a demand for corticosteroids, alteration from immunosuppressant to biologics, and an increased dose or frequency of biological agents. The secondary outcome was endoscopic recurrence, which was defined as a modified Rutgeerts score ⩾ i2b. 11 Two researchers (C. Li and R. Chen), blinded for the clinical characteristics and level of inflammatory biomarkers, assessed all endoscopy results based on modified Rutgeerts score independently. Discordant cases were re-evaluated by another experienced endoscopist (S. Zhang) and confirmed with consensus of opinion.
Clinical and endoscopic recurrence-free survival time were determined by the interval from the initial ileocolonoscopy to the events. Only patients with at least one endoscopy examination during the follow-up time were included for the analysis of secondary outcome. Patients with no primary or secondary outcomes observed during follow-up were considered as right-censored.
Statistics analysis
Categorical and continuous variables were described as number (frequency) and median [interquartile ranges (IQR)], respectively. For continuous variables, the optimal cutoff values were determined by X-tile 3.6.1 software 14 (Yale University, New Haven, CT, USA). The Kaplan–Meier method was performed to calculate the cumulative incidences of clinical recurrence or endoscopic recurrence, and the log-rank test was used to compare the difference among groups. Time-dependent receiver operating characteristic curves (ROC) were simultaneously plotted to evaluate the prognostic value of each variable using the R package survivalROC. Univariate Cox proportional hazards regression was conducted to evaluate the hazard ratio (HR) and 95% confidence interval (CI) of both clinical characteristics and NLR for postoperative recurrence. Then, variables with a p ⩽ 0.10 were included in a multivariate Cox regression model to adjust for potential confounders including history of CD-related resection and medication during follow-up.15–17 A p value less than 0.05 was considered as statistically significant. The statistical analyses were conducted by SPSS 24.0 (SPSS Inc., USA).
Results
Study population
In all, 411 patients who received an ileocolonic resection from 2013 to 2020 were reviewed and 83 patients were finally eligible for this study (Figure 1). In this bicentral cohort study, 60 (72.3%) patients were male, 7 (9.5%) had upper gastrointestinal tract involvement, and 18 (24.3%) had previous CD-related surgery. The median (IQR) time from surgery to the initial endoscopy was 6.3 (4.2–11.6) months. According to postoperative medications, 43 (51.8%) and 34 (41.0%) patients received immunosuppressants and biologics, respectively. During the follow-up time, 69 (83.1%) patients had at least one endoscopy examination and were included for secondary outcome analysis. The patient characteristics of these patients (endoscopic recurrence cohort) were disclosed in Supplemental Table 2.
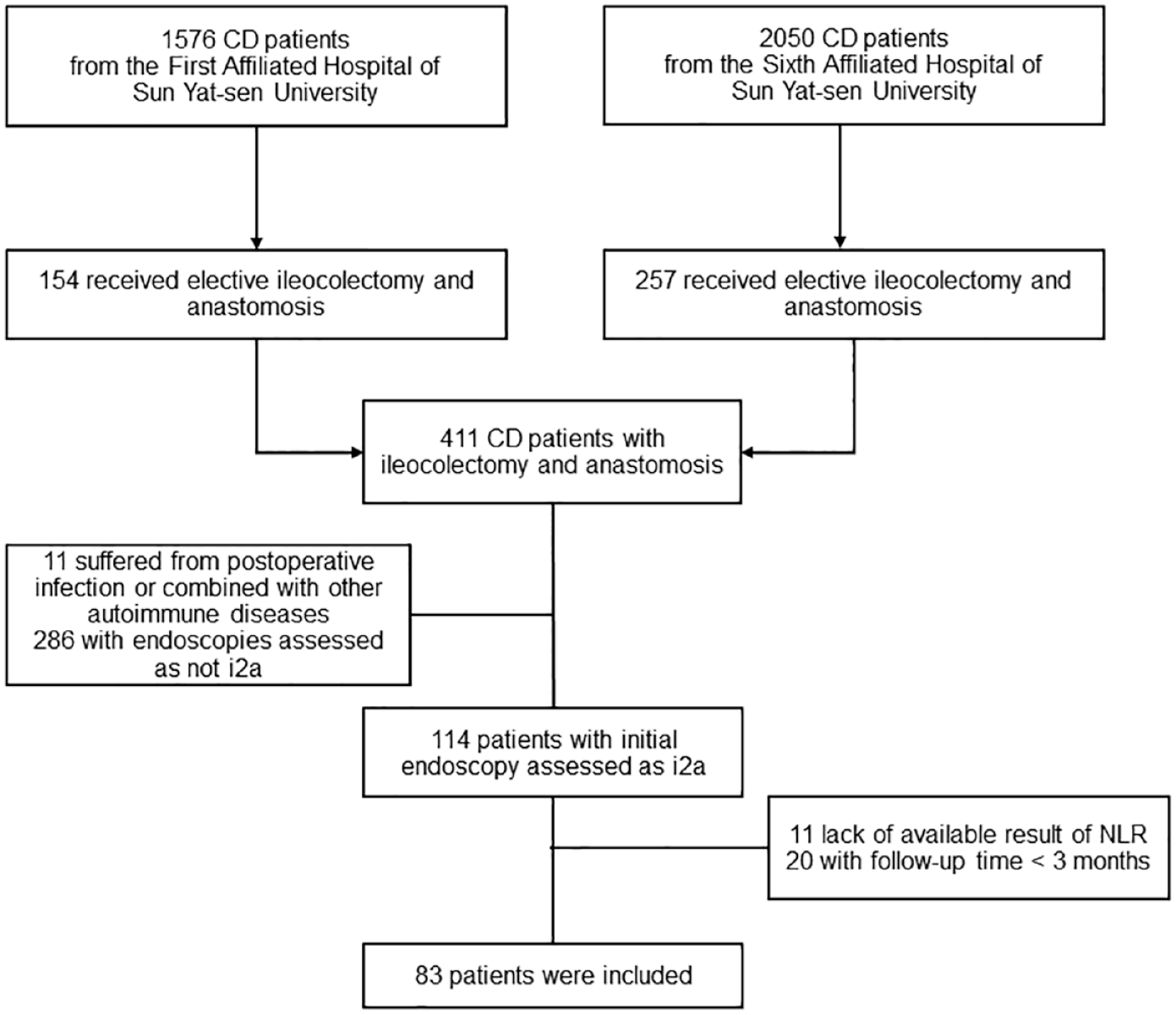
Flow chart.
NLR for predicting clinical recurrence
In all, 36 (48.6%) patients experienced clinical recurrence with a median follow-up time of 16.3 (IQR, 9.7–26.3) months (Figure 2(a)). Patients with NLR > 2.45 (p = 0.004; Figure 2(b)) or age at surgery >45 years (p = 0.037; Figure 2(c)) had shorter time to develop clinical recurrence. The area under ROC of the prediction of NLR for 1- and 2-year recurrence-free survival was 0.627 and 0.718, respectively (Supplemental Figure 1A and 1B) (Table 1). As shown in Table 2, the unadjusted HR of NLR and age at surgery were 2.58 (95% CI, 1.33–5.00; p = 0.005) and 2.49 (95% CI, 1.02–6.05; p = 0.044), respectively. After adjusting potential covariates, including surgery history and medications after colonoscopy, NLR > 2.45 was the only independent risk factor for clinical recurrence, with an adjusted HR of 2.88 (95% CI, 1.39–6.00; p = 0.005; Table 2).

Kaplan–Meier curves of clinical recurrence-free survival for (a) all patients, (b) patients with NLR >2.45 versus NLR ⩽ 2.45, and (c) patients with age at surgery >45 years versus age at surgery ⩽45 years.
Patient characteristics.

Continuous and categorical variables were described as median (interquartile range) and number (%), respectively.
CD, Crohn’s disease.
Prognostic factors for clinical recurrence.

Adjusted by previous CD-related surgery and medications during follow-up. The bold font represents statistical significance at p<0.05.
CD, Crohn’s disease; CI, confidence interval; HR, hazard ratio; NLR, neutrophil-to-lymphocyte ratio.
NLR for predicting endoscopic recurrence
The secondary outcome (endoscopic recurrence) analysis included 68 patients with a median follow-up of 15.1 (9.3–28.6) months (Supplemental Figure 2A). The cumulative incidence of endoscopic recurrence in patients with NLR > 2.45 was higher than those with low level of NLR (p = 0.089; Supplemental Figure 2B). The area under ROC of the prediction of NLR for 1- and 2-year recurrence-free survival was 0.590 and 0.648, respectively (Supplemental Figure 1C, D). In the multivariate Cox regression analysis, patients with NLR > 2.45 had a 4.54-fold risk (95% CI, 1.07–19.3; p = 0.040; Table 3) for endoscopic recurrence than those with NLR ⩽ 2.45. Moreover, patients with older age at surgery also had higher risk for endoscopic recurrence in the Kaplan–Meier analysis (p = 0.002; Supplemental Figure 2C). However, the adjusted HR of age at surgery (1.86, 95% CI, 0.38–9.04; p = 0.442) was not significant in the multivariate Cox regression model.
Prognostic factors for endoscopic recurrence.

Adjusted by previous CD-related surgery and medications during follow-up. The bold font represents statistical significance at p<0.05.
CD, Crohn’s disease; CI, confidence interval; HR, hazard ratio; NLR, neutrophil-to-lymphocyte ratio.
A risk score for postoperative recurrence
NLR > 2.45 and age at surgery >45 years were associated with postoperative recurrence in univariate analysis. To further stratify patients with iAL, we built a simple risk score attributing one point for NLR > 2.45 and one point for age at surgery >45 years. According to the Kaplan–Meier analysis, patients with a higher risk score had a shorter recurrence-free survival time (p < 0.001 for clinical recurrence and p = 0.002 for endoscopic recurrence; Supplemental Figure 3). The median clinical recurrence-free survival time of groups scored 0, 1, and 2 was 34.1, 17.9, and 7.7 months, respectively. According to endoscopic recurrence, the median survival time for the group with a risk score of 0 could not be calculated while the median for group with risk score of 1 and 2 was 40.1 and 24.3 months, respectively. As shown in Table 4, patients with a risk score of 2 had a 6.97-fold risk for clinical recurrence (adjusted HR, 6.97; 95% CI, 2.19–22.16; p = 0.001) and a 10.54-fold risk for endoscopic recurrence (adjusted HR, 10.54; 95% CI, 2.28–48.59; p = 0.003), when compared to those with a score of 0. In addition, patients with a score of 1 also developed clinical recurrence more rapidly (adjusted HR, 2.48; 95% CI, 1.22–5.02; p = 0.012) than those scored 0.
A risk score for postoperative recurrence.

Risk score: 0 (without NLR > 2.45 nor age at surgery >45 years); 1 (with NLR > 2.45 or age at surgery >45 years); 2 (with NLR > 2.45 and age at surgery >45 years).
Adjusted by previous CD-related surgery and medications during follow-up.
aHR, adjusted hazard ratio; CI, confidence interval; NLR, neutrophil-to-lymphocyte ratio.
Discussion
Although the Rutgeerts score or modified Rutgeerts score is widely applied in postoperative patient management in CD, patients with iAL have distinct prognosis, and the question concerning how to stratify these patients still remains.18,19 In this bicenter cohort study, we demonstrated that NLR was a promising biomarker to predict postoperative recurrence in patients with iAL. Patients with NLR > 2.45 were at higher risk of postoperative recurrence compared to those who had a low NLR. Moreover, a simple risk score based on NLR and age at surgery succeeded in identifying patients with different risk of postoperative recurrence. Together, we found a novel biomarker and developed an effective scoring system to facilitate the risk stratification in patients with iAL.
NLR, with advantages of non-invasion, affordability, and availability, is a widely used biomarker in clinical practice, especially in predicting prognosis. The prognostic value of NLR in inflammatory bowel disease has been exhibited by several studies. For instance, NLR is able to predict mucosal healing in ulcerative colitis patients 20 and abscess formation in CD patients. 21 Moreover, a higher level of NLR is associated with the occurrence of postoperative complications in CD.10,22 Similarly, we demonstrated that a high level of NLR indicated a high risk of postoperative recurrence in CD patients with iAL. A potential interpretation of why a high level of NLR is associated with poor prognosis is that NLR is an indicator of a disordered immune system. In inflammatory bowel disease, neutrophils act as first effector cells and exert a crucial role in inflammation as well as tissue injury. 23 Meanwhile, neutrophil activation, migration, and degranulation are shown to be vital immunity mechanisms of gut damage. 24 Furthermore, there are several studies demonstrating that an imbalance in T-cell subsets such as T helper cells is a significant contributor to disease progression. 25 A recent study implicated that baseline percentages of T-cell subsets including CD3+, CD4+, and regulatory T cells were related to disease activity and disease course. 26 In this study, we found that a higher neutrophil concentration but a lower lymphocyte concentration in peripheral blood was related to worse clinical prognosis. Therefore, NLR, the integrated marker from two white blood cell subtypes, may represent the activity of both innate and adaptive immune pathways. Furthermore, NLR was shown to correlate with other lymphocyte based predictors, including platelet-to-lymphocyte ratio, lymphocyte-monocyte ratio, and Onodera prognostic nutrition index, which were associated with postoperative complication in CD.22,27 Although further researches focusing on which subtypes of lymphocytes are representative for poor prognosis in CD patients with iAL are warranted, it is reasonable and impactful to use NLR as an index to stratify patients with iAL and then guide the prophylaxis of postoperative recurrence.
Despite the broad application of NLR, it remains an unsettled issue according to the cutoff selection which shows high heterogeneity among different studies. In a systematic scope review, the cutoff value of NLR to distinguish CD patients from healthy controls ranged from 2.13 to 2.85 while the interval of NLR for differentiation clinical disease activity of patients with CD is 1.57–5.35. 9 Ulteriorly, Kang et al. 22 reported a cutoff value of 4.1 for the prediction of postoperative complication. Considering the unparallel pathological mechanisms among postoperative recurrence, postoperative complications and natural disease progression without surgical invention, it is indispensable to independently determinate the cutoff value of NLR. In our study, we determined the cutoff value of NLR by X-tile software which is validated and widely utilized for the cutoff selection. 14 The cutoff of 2.45 could effectively stratify patients for predicting both clinical and endoscopic recurrence. Therefore, we believed that 2.45 was a reliable cutoff of NLR to predict postoperative recurrence.
Besides NLR, we also evaluated the prognostic values of clinical characteristics in patients with iAL. Age at surgery >45 years is the only clinical variable associated with postoperative recurrence in our study. A multicenter study conducted by Joustra et al. also found that older age at surgery was a risk factor for endoscopic recurrence in all postoperative CD patients. 4 In addition, the American Gastroenterological Association Institute Guideline recommended older age at surgery (over 50 years) as one of the indicators to stratify postoperative CD patients. 28 Therefore, although studies with larger sample sizes and prospective designs are warranted, we considered this indicator may be important for stratification in patients with iAL. Furthermore, we created a risk score based on NLR and age at surgery. The finding that the risk score can stratify the risk of postoperative recurrence in CD patients with iAL precisely is exciting. We believe that after confirming the performance and generalization of this simple risk score, the utilization of it will facilitate patient management and tailor the prophylaxis of postoperative recurrence.
Furthermore, selection of medication strategies was discovered as an independent factor in our endoscopic recurrence cohort. There are several researches investigating the efficacy of biologics and immunosuppressants on preventing postoperative recurrence of CD, but with no consensus accepted. In one pooled analysis of six trials, anti-TNF-α is demonstrated to be superior to thiopurine prophylaxis in the area of preventing endoscopic and clinical postoperative recurrence after ileocolonic resection. 17 However, a significant discrepancy between biologics and immunosuppressant was not confirmed in our study in either the clinical and endoscopic prognosis cohorts, with only a trend present. Meanwhile, a randomized controlled trial reported that infliximab can decrease endoscopic, but not clinical recurrence in CD patients compared to placebo, 29 which is the same as our findings. Furthermore, anastomotic configuration may be another treatment-related predictor for postoperative recurrence in CD. A recent systematic review revealed that Kono-S anastomosis is a protective factor for postoperative recurrence, when compared mesenteric excision 30 ; however, the evidence in this review was mostly poor. Thus, high-quality studies including all potential treatment-related indicators and adjusting confounders are required to investigate the roles of treatment methods in recurrence prophylaxis.
To the best of our current knowledge, our work is the first to reveal the prognostic value of postoperative recurrence in CD, while there were some limitations in our study. The main limitation was the retrospective design. Although there is inherent risk of bias in a retrospective cohort, we excluded patients with a short follow-up time, limited the time of NLR results within 1 week around the endoscopy examinations to reduce potential bias. Second, we did not assess the prognostic value of fecal calprotectin, which is one of the most promising biomarkers in CD. 31 Because iAL (equal to i2a) is not defined as endoscopic recurrence according to the modified Rutgeerts score, patients with iAL are not regularly tested for the concentration of fecal calprotectin in our centers. Despite lacking data of fecal calprotectin, we found NLR, an easily available and reliable biomarker, could predict postoperative recurrence in patients with iAL independently. Moreover, we intend to perform a prospective study to investigate the prognostic value of fecal calprotectin in postoperative CD patients in the near future. Third, patients were unevenly divided into three groups based on the risk score we built and the small sample sizes of patients with score 2 resulted in the wide CIs surrounding the risk estimates. The small sample size and broad definition for clinical recurrence may also restrict the statistical and clinical significance. Therefore, a much larger cohort is needed to reinforce and validate the risk score.
In conclusion, we demonstrated NLR as an independent prognostic factor of postoperative recurrence in CD patients with iAL and developed an effective risk score to stratify these patients. Our findings may contribute to the personalized management and treatment selection in CD patients with iAL. For limited as a relatively small retrospective cohort, prospective researches are needed to verify these findings.
Supplemental Material
sj-docx-1-tag-10.1177_17562848231165129 – Supplemental material for Neutrophil-to-lymphocyte ratio for predicting postoperative recurrence in Crohn’s disease patients with isolated anastomotic lesions
Supplemental material, sj-docx-1-tag-10.1177_17562848231165129 for Neutrophil-to-lymphocyte ratio for predicting postoperative recurrence in Crohn’s disease patients with isolated anastomotic lesions by Rirong Chen, Chao Li, Kang Chao, Yizhe Tie, Jieqi Zheng, Huili Guo, Zhirong Zeng, Li Li, Minhu Chen and Shenghong Zhang in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-tif-2-tag-10.1177_17562848231165129 – Supplemental material for Neutrophil-to-lymphocyte ratio for predicting postoperative recurrence in Crohn’s disease patients with isolated anastomotic lesions
Supplemental material, sj-tif-2-tag-10.1177_17562848231165129 for Neutrophil-to-lymphocyte ratio for predicting postoperative recurrence in Crohn’s disease patients with isolated anastomotic lesions by Rirong Chen, Chao Li, Kang Chao, Yizhe Tie, Jieqi Zheng, Huili Guo, Zhirong Zeng, Li Li, Minhu Chen and Shenghong Zhang in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-tif-3-tag-10.1177_17562848231165129 – Supplemental material for Neutrophil-to-lymphocyte ratio for predicting postoperative recurrence in Crohn’s disease patients with isolated anastomotic lesions
Supplemental material, sj-tif-3-tag-10.1177_17562848231165129 for Neutrophil-to-lymphocyte ratio for predicting postoperative recurrence in Crohn’s disease patients with isolated anastomotic lesions by Rirong Chen, Chao Li, Kang Chao, Yizhe Tie, Jieqi Zheng, Huili Guo, Zhirong Zeng, Li Li, Minhu Chen and Shenghong Zhang in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-tif-4-tag-10.1177_17562848231165129 – Supplemental material for Neutrophil-to-lymphocyte ratio for predicting postoperative recurrence in Crohn’s disease patients with isolated anastomotic lesions
Supplemental material, sj-tif-4-tag-10.1177_17562848231165129 for Neutrophil-to-lymphocyte ratio for predicting postoperative recurrence in Crohn’s disease patients with isolated anastomotic lesions by Rirong Chen, Chao Li, Kang Chao, Yizhe Tie, Jieqi Zheng, Huili Guo, Zhirong Zeng, Li Li, Minhu Chen and Shenghong Zhang in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.