
Abstract
Background:
The COVID-19 pandemic led to the urgent implementation of telehealth visits in inflammatory bowel disease (IBD) care; however, data assessing feasibility remain limited.
Objectives:
We looked to determine the completion rate of telehealth appointments for adults with IBD, as well as to evaluate demographic, clinical, and social predictors of incomplete appointments.
Design:
We conducted a retrospective analysis of all patients with IBD who had at least one scheduled telehealth visit at the NYU IBD Center between 1 March 2020 and 31 August 2021, with only the first scheduled telehealth appointment considered.
Methods:
Medical records were parsed for relevant covariables, and multivariable logistic regression was used to estimate the adjusted association between demographic factors and an incomplete telehealth appointment.
Results:
From 1 March 2020 to 31 August 2021, there were 2508 patients with IBD who had at least one telehealth appointment, with 1088 (43%) having Crohn’s disease (CD), 1037 (41%) having ulcerative colitis (UC), and 383 (15%) having indeterminate colitis. Of the initial telehealth visits, 519 (21%) were not completed, including 435 (20%) among patients <60 years as compared to 84 (23%) among patients ⩾60 years (p = 0.22). After adjustment, patients with CD had higher odds of an incomplete appointment as compared to patients with UC [adjusted odds ratio (adjOR): 1.37, 95% confidence interval (CI): 1.10–1.69], as did females (adjOR: 1.26, 95% CI: 1.04–1.54), and patients who had a non-first-degree relative listed as an emergency contact (adjOR: 1.69, 95% CI: 1.16–2.44). While age ⩾60 years was not associated with appointment completion status, we did find that age >80 years was an independent predictor of missed telehealth appointments (adjOR: 2.92, 95% CI: 1.12–7.63) when compared to individuals aged 60–70 years.
Conclusion:
Patients with CD, females, and those with less social support were at higher risk for missed telehealth appointments, as were adults >80 years. Engaging older adults via telehealth, particularly those aged 60–80 years, may therefore provide an additional venue to complement in-person care.
Introduction
The start of the COVID-19 pandemic in March 2020 led to an increased rate of telehealth visits, promoted by the Department of Health and Human Services.1,2 Virtual visits, both over the phone and video, require patient capacity to virtually access the appointment, troubleshoot equipment, and communicate without in-person cues, which can be made even more difficult with hearing loss. 3 Furthermore, technological gaps may be particularly challenging to overcome as older adults (⩾65 years) are less likely to own requisite devices to access their appointments (i.e. 40% did not own smartphones, 45% did not own laptops/desktops, and 68% did not own tablets 4 ), know how to use their device, 5 or have internet access (25% did not use the internet 4 and 42% did not have in-home broadband access 6 ). Older adults may therefore be more vulnerable to missing appointments given cognitive, physical, and technological gaps. However, the incorporation of telehealth into patient care can also have significant benefits, as individuals can check-in with providers from remote locations, limiting geographic, transportation, and physical barriers to care.
Prior to the SARS-CoV-2 pandemic, telemedicine focus was on chronic conditions such as depression, diabetes mellitus, cardiovascular or pulmonary diseases. 7 Since the start of the pandemic however, there has also been a rapid shift to adopt telehealth in inflammatory bowel disease (IBD) care, 8 and in the field of gastroenterology more broadly. 9 As individuals with IBD comprised of Crohn’s disease (CD) and ulcerative colitis (UC) have chronic inflammation, it is critical to have frequent touchpoints with healthcare providers. 9 Telehealth visits may help facilitate this, as they often provide reduced out-of-pocket costs 10 and greater convenience for both patients and providers, 11 without a compromise in the quality of care. However, as the IBD patient population is aging, it is now essential to explore barriers to telehealth care, to both understand and improve current practices.
While prior data have shown increasing age, race, and non-commercial insurance increase the likelihood of missing or not using a telehealth visit, these studies have not considered additional social and medical factors (e.g. partnership status, comorbidity index) that can influence this risk. 8 Therefore, in this study, we aimed to understand a broader range of predictors of incomplete telehealth appointments, and to identify how these factors may differ based on age, within the context of the COVID-19 pandemic where there was widespread utilization of telehealth.
Methods
Study population
We conducted a retrospective analysis of all patients with IBD who had at least one scheduled telehealth visit at the Inflammatory Bowel Disease Center of NYU Langone Health between 1 March 2020 and 31 August 2021. To ensure patients with more frequent telehealth appointments would not be disproportionately represented, only the patient’s first telehealth appointment within the study period was considered. Furthermore, to help eliminate selection bias, we ran a sensitivity analysis restricting our study to include a period when only telehealth appointments were being conducted (1 March 2020 and 31 March 2021).
International Classification of Diseases (ICD)-9-CM and ICD-10-CM diagnosis codes for ulcerative colitis (UC: K51.x) and Crohn’s disease (CD: K50.x), as well as being seen by an IBD provider, were used to identify patients with IBD. In addition, 5% of charts were randomly sampled and manually reviewed to confirm >95% accuracy. The reporting of this study conforms to the STROBE statement. 12
Primary outcome
The primary outcome was telehealth appointment completion status, classified categorically as complete or incomplete. An incomplete visit was defined as discontinued before being seen, a cancellation, or no-show. To limit potential misclassification of patients who were able to access the system, we performed a sensitivity analysis excluding those who left before being seen, as these patients demonstrated an ability to log in to the visit. Furthermore, to assess the possibility of technical difficulties contributing to a missed telehealth appointment, we performed an additional analysis assessing age as a predictor of a missed second telehealth appointment among a subgroup of patients who successfully completed their first telehealth appointment.
Of note, prior to a telehealth appointment at the NYU IBD center, all patients are provided the same step-by-step guide on how to connect to their visit. In addition, the electronic health record software automatically performs an audio and visual capability test of the user’s registered device prior to the visit.
Exposures of interest
We collected electronic health record information pertaining to demographic, social, and medical factors. Demographics included age (defined as a binary variable, <60 or ⩾60 years), sex, and preferred language (classified as a binary variable, English or other). Social factors assessed were partnership status (defined as a binary variable based on whether or not the patient had partner information listed in their chart), as well as level of emergency contact relationship (classified as a categorical variable: spouse, first-degree relative, other (e.g. friend, uncle, neighbor) or none; Supplemental Table 1). Income was determined using state-level data pertaining to median income per zip code, and then classified as a binary variable of above or below the NY State Federal Income Guidelines for a four-member household (~$50,000/year). 13
Medical information was extracted from the electronic health record pertaining to IBD subtype (classified as UC, CD, or indeterminate colitis, with indeterminate colitis being defined as patients who had ICD codes for both UC and CD), current or past history of biologic or small molecule inhibitor use (including adalimumab, infliximab, ustekinumab, vedolizumab, tofacitinib, and ozanimod), and comorbidities. Using comorbidities identified in the Charlson comorbidity index, patients were then categorized as having 0, 1, ⩾2 comorbid conditions.
When assessing predictors of telehealth completion solely among older adults (⩾60 years) with IBD, we included the same demographic, social, and medical exposures as in the overall population, and incorporated age, stratifying patients by decade (60–70, 71–80, and >80 years). In addition, we captured in-person versus telehealth appointment completion status for older adults with IBD to understand overall behavioral patterns during our time frame of interest.
Statistical approach
All variables were reported as counts and percentages, and assessed using chi-square analysis. Variable selection was then performed in which covariates with a p value of ⩽0.2 on univariable analysis, as well as age which we included a priori, were included in a multivariable logistic regression model to determine the independent predictors of completing a telehealth appointment. 14 To identify important factors for telehealth completion among older adults, multivariable logistic regression was also performed among individuals with IBD who were ⩾60 years of age. All analyses were performed on RStudio, and statistical significance was considered at the alpha 0.05 level with two-sided testing.
Results
Demographics
There was a total of 3495 unique patients with IBD seen at the NYU IBD center between 1 March 2020 and 31 August 2021. Of these patients, 2508 (72%) had at least one telehealth visit scheduled during this time. Of the 2508 who had a telehealth visit scheduled, 51% were female, 1037 (41%) had UC, 1088 (43%) had CD, and 383 (15%) had indeterminate colitis (Table 1). Overall, the average age was 40 years (SD ± 15.5), with the majority being primarily English speakers (99%; 2480).
Baseline demographics for 2508 patients with IBD who had a telehealth visit between March 2020 and August 2021.

Poverty line defined as median income in zip code is less than the NY state federal income guidelines for a four-member household (~$50,000/year).
Indicates missing values in category: for emergency contact relationship, 1 patient did not have a value and for income 24 patients did not have a value.
CD, Crohn’s disease; IBD, inflammatory bowel disease; UC, ulcerative colitis.
When considering social factors, 47% (1180) indicated they had a partner. In total, 986 (39%) had a spouse listed as an emergency contact, whereas 46% (1147) listed a first-degree relative as an emergency contact, 12% (305) listed other, and 3% (69) had no emergency contact (Table 1). 92% (2302) of patients lived in a zip code where the median income was greater than the poverty line. In addition, 66% (1656) had a current or past history of biologic or small molecule inhibitor use, and 80% (2022) had no underlying comorbid conditions.
Factors associated with a missed telehealth appointment
Of the 2508 initial telehealth visits for patients with IBD, 21% (519) were not completed, including 20% (435) among patients under the age of 60 years as compared to 23% (84) among patients 60 years and older (p = 0.22).
On univariable analysis, IBD subtype was associated with an increased risk of missed telehealth appointments. 23% of patients with CD did not complete their first telehealth appointment as compared to 18% of UC patients and 20% of patients with indeterminate colitis (p < 0.01). In addition, females were more likely to miss a telehealth appointment as compared to males (23% versus 19%, respectively, p = 0.01). Furthermore, not having a spouse or first-degree relative listed as an emergency contact was also associated with decreased telehealth completion status (18% for spouse versus 22% for first-degree relative versus 26% for other versus 25% for none, p = 0.01; Table 1). In addition to age 60 years and above, variables not associated with a missed telehealth appointment included partnership status, preferred language, income, the presence of comorbidities, and current or past history of biologic/small molecule inhibitor use.
On multivariable analysis, all variables that had a significant association with missed telehealth appointment on univariable analysis – IBD subtype (p < 0.01), sex (p < 0.05), and emergency contact relationship (p < 0.05) – remained significant predictors on multivariable analysis. Specifically, on multivariable logistic regression, patients with CD had higher odds of an incomplete telehealth appointment as compared to patients with UC [adjusted odds ratio (adjOR): 1.37, 95% confidence interval (CI): 1.10–1.69], as did females as compared to males (adjOR: 1.26, 95% CI: 1.04–1.54; Table 2). In addition, patients who did not have a first-degree relative listed as an emergency contact also had significantly higher odds of an incomplete appointment as compared to those who had a spouse listed (adjOR: 1.69, 95% CI: 1.16–2.44). On sensitivity analysis, when excluding those who left before being seen, we saw similar results – notably that females, patients with CD, and those with limited social support were more likely to miss a scheduled telehealth appointment (Supplemental Table 2).
Multivariable analysis examining predictors of missed telehealth appointments for patients with IBD.


 Demographic and social factors.
Demographic and social factors.
 Health factors.
Health factors.
 Social support factors.
Social support factors.
Adjusted for all variables listed in the table.
CD, Crohn’s disease; CI, confidence interval; IBD, inflammatory bowel disease; UC, ulcerative colitis.
Additional sensitivity analysis considering the time when only telehealth appointments were being offered, also showed similar results (Supplemental Table 3). However, in this analysis, age ⩾60 years was also significantly associated with missing a scheduled telehealth appointment. On subsequent analysis, when assessing the likelihood of an incomplete second telehealth appointment after successful completion of the first telehealth appointment, we found that age (<60 versus ⩾60 years) was not significantly associated with appointment completion rate (p = 0.66).
In-person versus telehealth appointments among older adults
During the time when both telehealth and in-person appointments were offered, 61% of older patients (⩾60 years) scheduled an initial telehealth appointment versus 39% who scheduled an initial in-person visit. Furthermore, 36% of patients 60 years and older did not schedule a telehealth visit during this time period. When comparing visit completion status, we noted older adults, however, were more likely to miss their in-person appointment as compared to their telehealth appointment (35% versus 18% respectively, p < 0.01).
Factors associated with a missed telehealth appointment among older adults
When assessing predictors of missed telehealth appointments solely among the 361 older adults with IBD, sex (p = 0.03) and age stratified by decade (p = 0.01) were found to be associated with missed telehealth appointments on univariable analysis (Table 3). Partnership status (p = 0.11), comorbidities (p = 0.51), and emergency contact relationship (p = 0.44), however, were no longer significantly associated with appointment completion. On multivariable analysis, only age was an independent predictor of appointment completion status, as patients who were >80 years of age had higher odds of an incomplete appointment as compared to patients 60–70 years (adjOR: 2.92, 95% CI: 1.12–7.63; Table 4).
Baseline demographics for 361 patients with IBD who had a telehealth visit between March 2020 and August 2021, and who are ⩾60 years of age.
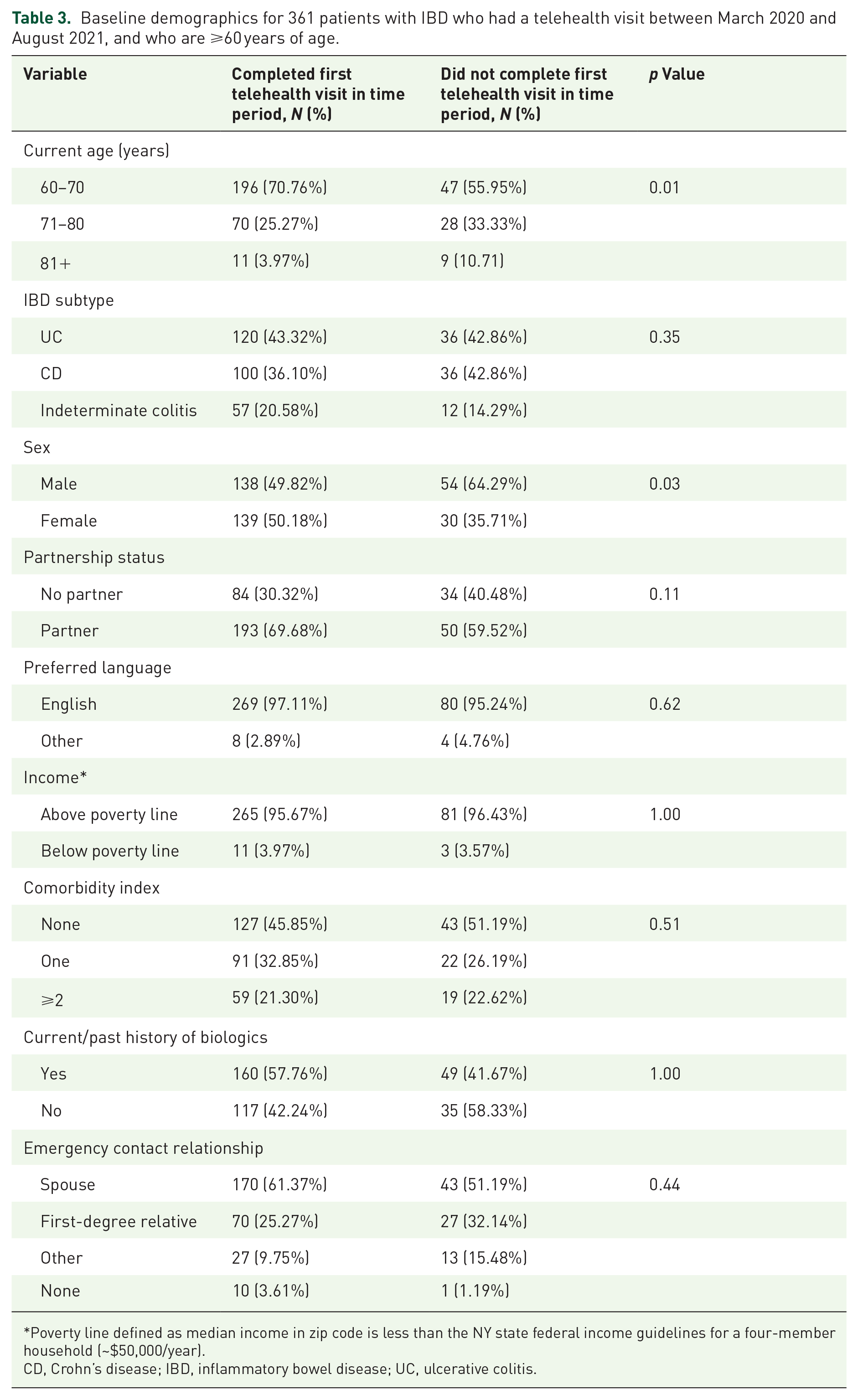
Poverty line defined as median income in zip code is less than the NY state federal income guidelines for a four-member household (~$50,000/year).
CD, Crohn’s disease; IBD, inflammatory bowel disease; UC, ulcerative colitis.
Multivariable analysis examining predictors of missed telehealth appointments for patients with IBD and who are ⩾60.
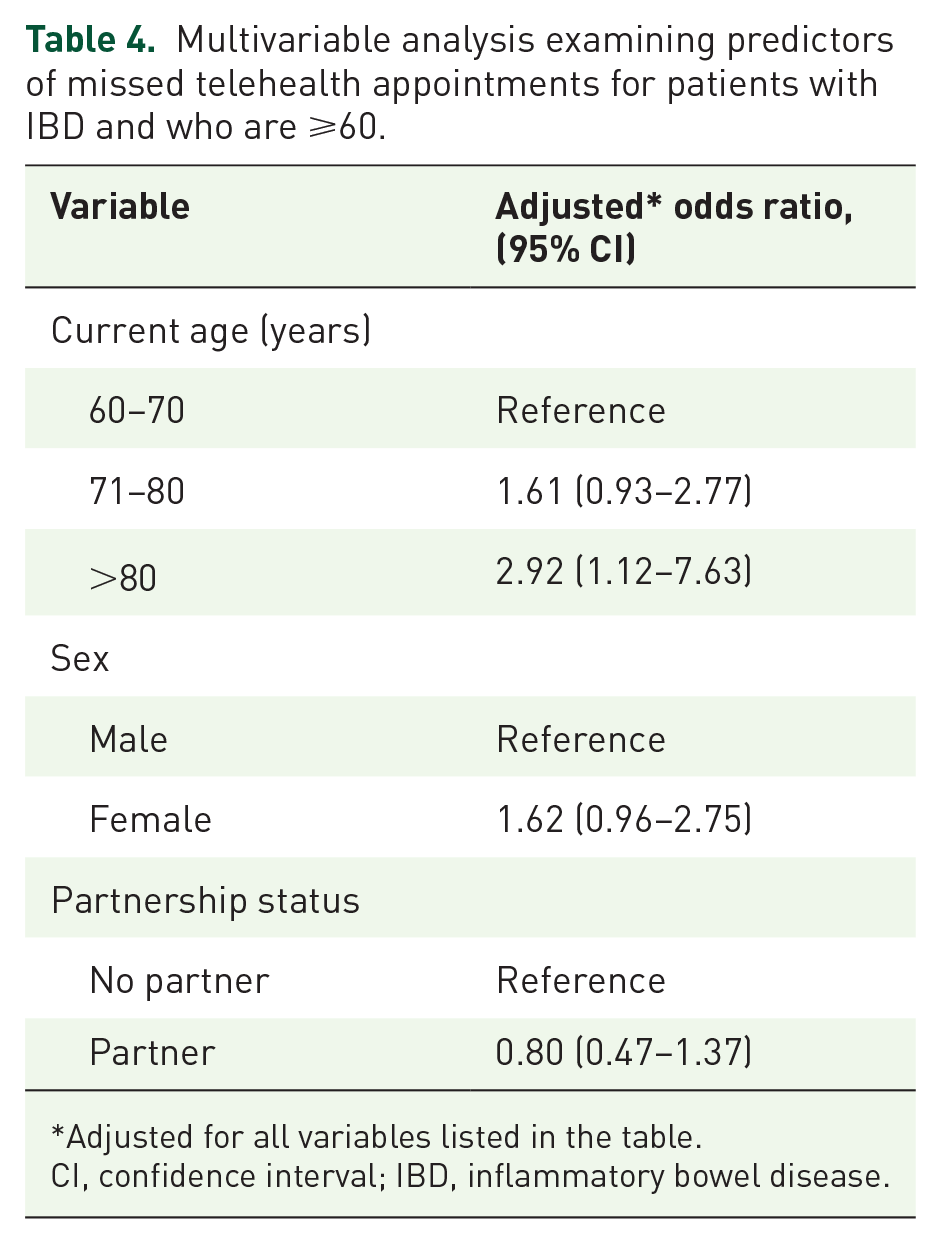
Adjusted for all variables listed in the table.
CI, confidence interval; IBD, inflammatory bowel disease.
Discussion
In our study, we found that among all patients with IBD using telehealth, females, patients with CD, and those with limited social support were more likely to miss a scheduled telehealth appointment. In contrast, older age (⩾60 years) was not a significant risk factor for a missed telehealth appointment, with the exception of individuals older than 80 years, who were at higher risk for a missed appointment.
As the IBD patient population is increasing in prevalence and aging, there are concerns relating to equitable access to care, as physical (e.g. visual acuity and hearing loss) and cognitive limitations, 15 technological access and know-how, 16 and demographic and socioeconomic status can all significantly limit an individual’s ability to participate in a telehealth appointment.8,17 In a recent single-center study of patients with IBD, Shah et al. found that increasing age increased the likelihood of a video encounter failure. 8 In our study however, which has also been shown in non-IBD patient populations, we found that adults 60 years and older were not more likely to miss a telehealth appointment.18,19 One possible explanation for this difference may be the disparate age categorizations, as the study by Shah et al. compared individuals 50 years and older to individuals 18–30 years. 8 In addition, this difference may also reflect the prior study’s inclusion of all telehealth visits, perhaps overrepresenting a select group of patients. Last, we adjusted for social support factors, including socioeconomic, emergency contact, and partnership status, possibly contributing to the differences in results seen.
Furthermore, in our study, we found that although older adults were more likely to schedule an in-person appointment in comparison to a telehealth appointment, they were also more likely to miss an in-person appointment. This may be due to transportation or other barriers and emphasizes the positive role telehealth may play among individuals that can successfully complete the appointment.
However, we did find that age over 80 years was an independent predictor of missed telehealth appointments when accounting for additional social support factors, as almost half of patients in this age category missed their telehealth appointments. This finding is congruous with previous studies which have shown that the oldest age brackets have most difficulty completing telehealth appointments.20,21 This finding suggests that at the older extremes of age, technological challenges (e.g. small font size, difficulty with navigation, perception on technology) may play a role in telehealth appointment completion. Thus, to improve telehealth completion rates in this subgroup, special engagement by health systems may be considered when scheduling and preparing individuals 80 years and older for their telehealth appointments. A study in the Department of Medicine outpatient clinics across Vanderbilt University Medical Center found that a structured pre-visit telephone call, which included topics such as guidance on the technical steps for starting a visit and best practices for a visit, significantly increased the likelihood of a successful telehealth visit. 20
In addition, we found that having social support (a spouse or first-degree relative as an emergency contact) significantly improved the odds of completing a telehealth appointment. Analogous to prior findings, a lack of social support is often a key driver for missed appointments. One large study of 3188 participants aged 70 years and older found that technical support was a significant and independent predictor of telehealth usage, as individuals living with family or friends or in an assisted living facility were more likely to utilize telehealth. 22 This is not only important among older adults, but also among all adults with IBD, as we found a lack of social support to be associated with incomplete telehealth appointments for all patients with IBD.
When considering sex as an independent predictor of incomplete telehealth appointments, prior studies assessing use in the IBD setting did not show sex as being a significant predictor. 8 Our study, like a study from the University of Pennsylvania exploring telemedicine outpatient cardiovascular care, 23 showed that females were approximately 25% more likely to miss telehealth appointments as compared to males. 19 Although the reasons for this finding are unknown, prior studies have postulated that the differences observed may be due to a disproportionate distribution of childcare or employment constraints, making females less likely to be able to complete their telehealth appointments. 23 This, however, is an area that is in need of future investigation and research.
Last, we also found that IBD subtype was a significant driver of missed telehealth appointments. While the prior study by Shah et al. did not find a significant difference in telehealth completion status by IBD subtype, 8 we observed that individuals with CD were more likely to miss their telehealth appointments as compared to patients with UC. Although the reason for this finding remains unknown, we hypothesize that this may be due to the underlying differences in presenting symptoms between patients with UC versus CD. More specifically, patients with UC often have symptoms of urgency and hematochezia that are accompanied by frequent bowel movements, perhaps prompting them to seek and engage in a more expedited evaluation. 24
Strengths of our study include a large cohort of IBD patients at a major tertiary IBD center that serves a diverse patient population within New York City. In addition, IBD status was systematically determined using ICD codes in addition to being seen by an IBD provider, with 5% of charts manually reviewed to ensure >95% accuracy. The study also looked beyond demographic factors and explored social and economic factors known to influence whether a patient completes an appointment.
Given the retrospective nature of study, there are inherent limitations which should also be noted. First, race and ethnicity, socioeconomic and employment status, among other variables, are often omitted in the electronic health record, limiting our ability to accurately capture this information. Second, although we have a large sample of patients from a tertiary medical center and were able to adjust for a multitude of demographic, health, and social support factors additional cofounders may still exist. Third, our data come from a single tertiary referral health system in New York City. As such, telehealth utilization practices may not be reflective of the broader US population, with further data needed to assess this. Furthermore, we did not have access to the reasons for why patients missed their appointment (e.g. due to scheduling conflict, technological issues) and thus could not obtain specific reasons for an incomplete visit (e.g. scheduling conflict, technological issue).
In addition, the possibility of misclassification exists among individuals who logged in but left before being seen, as these individuals likely demonstrated an understanding of how to access the telehealth system. To account for this possibility, we performed a sensitivity analysis excluding these individuals, with similar results seen. Furthermore, when limiting the possibility of technical difficulties by only evaluating individuals who completed the first telehealth appointment, we observed analogous results; older age was not associated with increased odds of missing a second telehealth appointment.
Finally, selection bias is also possible, in that only patients who opt-in for a telehealth visit were considered, and thus may reflect a population of IBD patients who are more comfortable with this practice. To address this, we ran an additional sensitivity analysis considering the time period when only telehealth appointments were offered. Overall similar results were seen, though notably adults 60 years and older were more likely to have a missed telehealth appointment during this timeframe. These results suggest that older adults who have successfully completed a prior telehealth visit or who opt-in for a telehealth visit may be more likely to complete the visit, and that older adults for whom it is their first telehealth visit or who tend to defer virtual visits may need additional support should a virtual visit be required.
In sum, we found that females, patients with CD, and those with limited social support were more likely to miss a scheduled telehealth appointment. In addition, our results suggest that among individuals with IBD ages 60–80 years of age who schedule a telehealth visit, concerns about missing appointments may be overstated, suggesting that engaging older adults via telehealth may provide an additional venue to complement in-person care. These results can help inform how health systems assess appropriateness of telehealth versus in-person appointments, as well as point to potential interventions to decrease incomplete telehealth appointments (e.g. through more robust multi-channel reminders, practice sessions with the telehealth system, or dedicated patient navigators). Future studies should explore which interventions are most effective at supporting patients, and further assess the social, socioeconomic, including current employment status, and demographic reasons leading to missed telehealth appointments. Our study lays the framework for which future prospective work can be based upon, particularly focusing on patient-stated barriers and additional socioeconomic and technological factors that may impact the completion of a telehealth appointment.
Supplemental Material
sj-docx-1-tag-10.1177_17562848231158231 – Supplemental material for Risk factors for incomplete telehealth appointments among patients with inflammatory bowel disease
Supplemental material, sj-docx-1-tag-10.1177_17562848231158231 for Risk factors for incomplete telehealth appointments among patients with inflammatory bowel disease by Katherine L. Stone, Emma Kulekofsky, David Hudesman, Samuel Kozloff, Feza Remzi, Jordan E. Axelrad, Seymour Katz, Simon J. Hong, Ariela Holmer, Mara A. McAdams-DeMarco, Dorry L. Segev, John Dodson, Aasma Shaukat and Adam S. Faye in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.