
Abstract
Background:
The diagnosis of proximal small bowel involvement in Crohn’s disease (CD) can be challenging at magnetic resonance enterography (MRE). The inflammatory process in CD can be associated with peri-intestinal inflammatory reactions, including the presence of inflamed mesenteric lymph nodes.
Objectives:
To evaluate the significance of inflamed mesenteric lymph nodes adjacent to the jejunum at MRE in CD and the association with proximal bowel disease as detected by video capsule endoscopy (VCE).
Design:
This retrospective study was performed in two tertiary medical centres, and included 64 patients with CD who underwent MRE as well as VCE within 1 year.
Methods:
Data were collected for examinations performed between August 2013 and February 2021. MRE images were independently reviewed by radiologists who were blinded to the clinical data. Association between the presence of mesenteric lymph nodes adjacent to jejunum at MRE and disease activity according to VCE Lewis scores of proximal small bowel was examined.
Results:
VCE detected proximal disease in 24/64 patients (37.5%). Presence of regional lymph nodes in the jejunal mesentery was significantly associated with jejunal disease as seen on VCE (p < 0.001). Of the 20 patients who had proximal mesenteric lymph nodes at MRE, 15 (75%) had jejunal disease at VCE (sensitivity, 62.5%; specificity, 87.5%; and negative and positive predictive values, 79.5 and 75%, respectively). The number of regional lymph nodes was positively correlated with jejunal disease (mean: 2.63 ± 2.90 versus 0.78 ± 2.60, p = 0.01). Other MRE features of lymph nodes were not significantly predictive of jejunal CD.
Conclusion:
In patients with CD, inflamed regional lymph nodes in the jejunal mesentery at MRE can be valuable to suggest proximal small bowel disease, even when bowel wall features at imaging do not suggest disease involvement.
Plain language summary
The diagnosis of proximal small bowel involvement in Crohn’s disease (CD) can be challenging at magnetic resonance enterography (MRE). We analysed MRE examinations in patients with CD for the presence of lymph nodes adjacent to the proximal small bowel. We included 64 patients with CD who had MRE examinations and video capsule endoscopy (VCE) examinations within 1 year. Of 64 patients, 24 had proximal small bowel disease according to VCE. We found that of 20 patients who had regional mesenteric lymph nodes in the jejunal mesentery at MRE, 15 had proximal bowel disease involvement. We also found that patients with jejunal disease had a larger number of regional lymph nodes compared to patients without jejunal disease. All but one patient had normal appearing bowel at MRE. But, using regional mesenteric lymphadenopathy at MRE as an indicator for disease, 15/24 (62.5%) patients with proximal small bowel disease were detected. We therefore conclude that regional mesenteric lymph nodes assessment at MRE can aid diagnose proximal bowel disease, even when the proximal bowel looks normal at imaging. Presence of proximal mesenteric lymph nodes at MRE in patients with CD possibly warrant further investigation of the proximal small bowel by endoscopic measures.
Introduction
Crohn’s disease (CD) is an inflammatory bowel disease (IBD) that may affect any segment of the gastrointestinal tract. 1 The involvement of the proximal bowel is less common, accounting for up to 30% of cases.2,3 Proximal bowel disease, however, has a generally less favourable outcome compared with other locations. 4 In particular, it is associated with higher risk for strictures and penetrating complications, surgery, and postoperative recurrence.5,6
According to the European Crohn’s and Colitis Organisation and the European Society of Gastrointestinal and Abdominal Radiology guidelines, diagnostic assessment methods for proximal bowel involvement may include video capsule endoscopy (VCE), double balloon enteroscopy, magnetic resonance enterography (MRE), and intestinal ultrasound (US).7,8 Endoscopic methods are used more frequently compared to MRE and US for diagnosis.9,10 That is because endoscopic techniques are more sensitive for lesion detection in the proximal small bowel (20–40% higher sensitivity compared to imaging),2,11 MRE and US, although less sensitive for proximal lesions detection, have other advantages.12,13 These imaging modalities can detect trans-mural involvement as well as disease complications (e.g. strictures, fistulas, and abscesses).2,3
The inflammatory process in CD is usually associated with peri-intestinal inflammatory reactions. It has been suggested that the presence and features of mesenteric lymph nodes may correlate with early disease onset and disease activity.14,15 Thus, it is likely that proximal bowel disease detectable at VCE may be associated with regional mesenteric lymph node involvement, potentially detectable with imaging methods.
The significance of proximal mesenteric lymph nodes at imaging and association with disease activity has not been adequately investigated so far. We therefore aim to assess whether inflamed-appearing mesenteric lymph nodes adjacent to the jejunum at MRE are associated with proximal small bowel disease as detected by VCE.
Methods
Participant population
This retrospective study was conducted in two tertiary medical institutions in two countries. This study was reported according to the STARD list. 16 CD patients who underwent both MRE and VCE independently within 1 year, between August 2013 and February 2021 were included. Excluded were patients for whom MRE images or Lewis scores were not available, or in whom the examinations were more than 1 year apart. Clinical and demographic characteristics of patients were collected, including age, sex, duration of CD, smoking status, disease characteristics, and current treatment.
Imaging technique
In one institution, MRE was performed on a 1.5T GE Optima MR450w MRI with GEM Suite (GE Healthcare, Chicago, Illinois, USA). In the second institution, MRE was performed on a 1.5T Philips Achieva (Philips, Amsterdm, Netherlands). The MRE protocols, previously described, 17 are detailed in Supplemental Tables 1 and 2. Oral contrast media used was mannitol (360 ml Osmitrol 20% diluted in 1.5 l water) or polyethylene glycol (SELG-Esse diluted in 1.5 l water). Patients received an intravenous infusion containing 0.5 mg glucagon or N-butyloscopolamine. Liver acquisition with volume acquisition (GE LAVA or Philips THRIVE) sequences were acquired before and 40 s after injection of intravenous contrast medium (gadoterate meglumine, 0.5 mmol/ml by 0.2 ml/kg, or gadobutrol 0.1 ml/kg).
Imaging interpretation
MRE images were retrospectively reviewed by two radiologists in each institution. All radiologists were blinded to the clinical data including the Lewis scores at VCE. Disease activity was assessed at jejunum. Mesenteric lymph nodes at left upper quadrant (LUQ) were assessed regarding their number and size of the small diameter of the largest lymph node [short axis diameter (SAD)], contrast enhancement, T2-weighted intensity compared to the psoas muscle, and apparent diffusion coefficient (ADC). Counted and analysed were only lymph nodes larger than 0.5 cm.
VCE technique
VCE studies were performed with either a small bowel capsule (SB-III, Given Imaging, Yokne’am Illit, Israel) or a colonic capsule (PillCam, Given Imaging, Yokne’am Illit, Israel) in both centres. Analysis of the images was performed by board-certified two gastroenterologists, using RAPID 8 software (Given Imaging). Lewis scores were calculated for the jejunum separately (i.e. proximal small bowel tertile) using the common cut-offs. A score of less than 135 was considered as normal or clinically insignificant inflammation, values between 135 and 790 as mild inflammation, and above 790 as moderate to severe inflammation. 18
Statistical analysis
Data were tested for normality with the Shapiro–Wilk test. We conducted independent t-test to compare between continuous variables with a normal distribution, and chi-square test for categorical variables. Diagnostic values [sensitivity, specificity, and positive predictive value (PPV) and negative predictive value (NPV)] for regional lymph nodes at MRE as an indicator of jejunal disease were calculated. For that purpose, the presence of disease was defined according to VCE. Statistical analysis was performed using SPSS software for windows version 24.0 by IBM. p Values less than 0.05 on a two-sided test were considered statistically significant.
Results
A total of 64 patients (53 from one institution, and 11 from the other) were included in the final analysis. Mean age was 33.9 years [standard deviation (SD): 13.5, range: 13–75, median: 31.0]. There were 35 (54.7%) male patients and 29 female patients (45.3%). Mean disease duration was 5.16 years (SD: 5.10, range: 0–23, median: 4.0). Patient demographic and clinical characteristics are detailed in Table 1. The different medical therapies in the two institutions are detailed in Supplemental Table 3.
Demographic characteristics of patients.
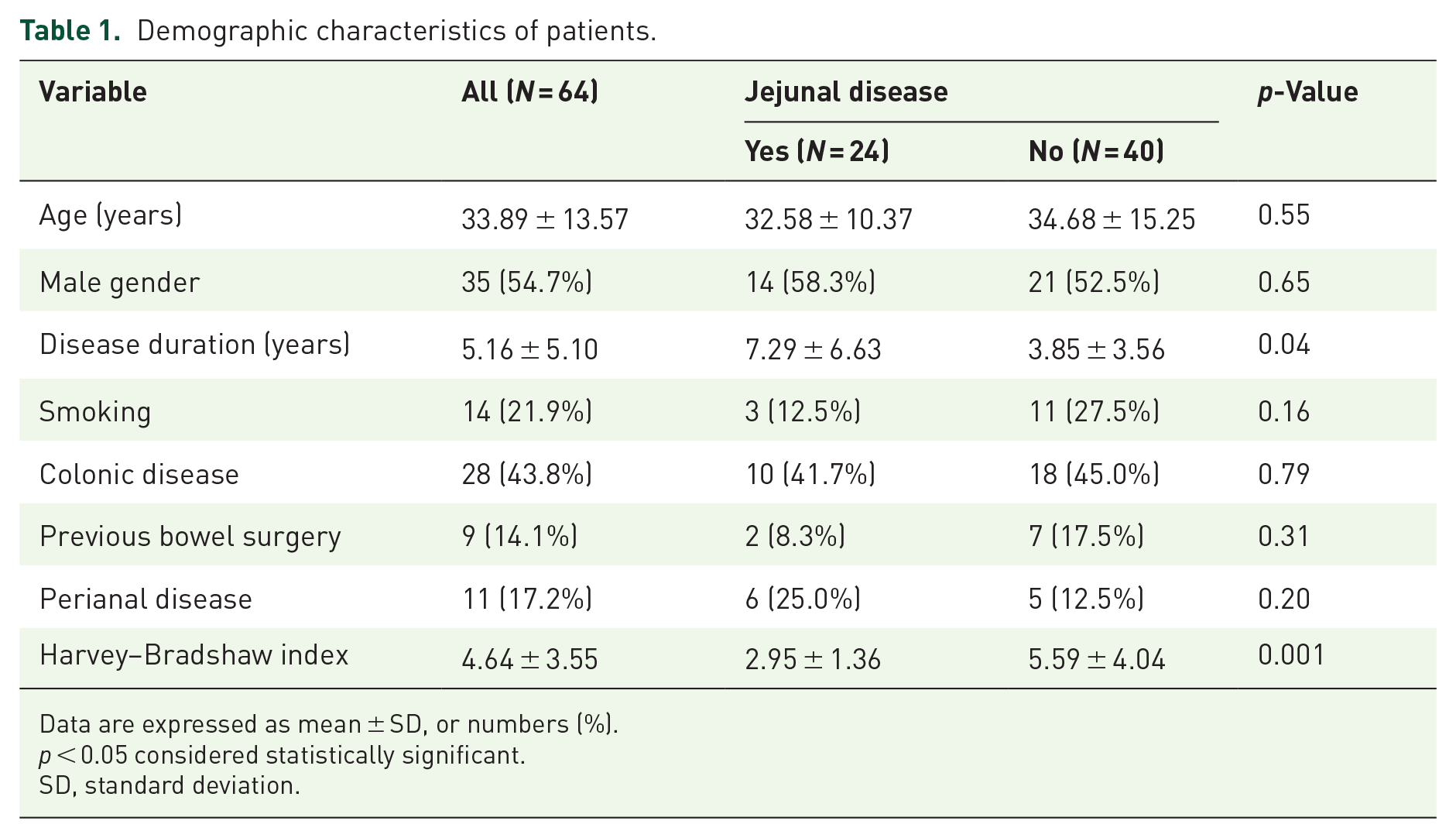
Data are expressed as mean ± SD, or numbers (%).
p < 0.05 considered statistically significant.
SD, standard deviation.
According to the VCE results, 24/64 (37.5%) of patients had jejunal disease, with a mean regional Lewis score of 691.5 (SD: 935.2, range: 135–3756, median: 450.0). When evaluating the bowel at MRE, proximal bowel disease was detected in only one patient, while distal bowel disease was detected in 42 patients. Mesenteric lymph nodes in LUQ were present in 20/64 (31.2%) patients. Their mean SAD was 0.80 cm ± 0.23, and the mean number of lymph nodes in LUQ was 1.47 ± 2.84. In contrast, mesenteric lymph nodes were present in the right lower quadrant in 41 patients, mean SAD 0.77 cm ± 0.27, and mean number of lymph nodes 2.98 ± 3.63.
Regional lymph nodes at MRE were significantly associated with jejunal disease at VCE (p < 0.001). Of the 20 patients who had mesenteric lymph nodes at LUQ, 15 (75%) had jejunal disease at VCE. Out of 44 patients who did not have mesenteric lymph node involvement at LUQ, 35 (79.5%) did not have jejunal disease at VCE. LUQ mesenteric lymph node involvement therefore had 62.5% (15/24) sensitivity, 87.5% (35/40) specificity, 75% (15/20) PPV, and 79.5% (35/44) NPV for detection of jejunal CD.
The number of regional lymph nodes was positively correlated with jejunal disease (mean: 2.63 ± 2.90 versus 0.78 ± 2.60, p = 0.01). Frequency of T2-weighted hyperintensity (14/15 versus 5/5, p = 0.55) and enhancement (11/15 versus 5/5 p = 0.13) were not associated with jejunal disease. SAD and ADC values did not reveal a significant correlation to disease (mean SAD: 0.8 ± 0.24 cm versus 0.82 ± 0.22 cm, p = 0.87; mean ADC: 1.57 ± 0.50 versus 1.17 ± 0.11, p = 0.20). The MRE features of regional lymph nodes in patients with and without jejunal disease are detailed in Table 2.
MRE regional lymph nodes features.

Data are expressed as mean ± SD, or numbers (%).
p < 0.05 considered statistically significant.
ADC, apparent diffusion coefficient; LUQ, left upper quadrant; MRE, magnetic resonance enterography; No., number; SAD, short axis diameter; SD, standard deviation.
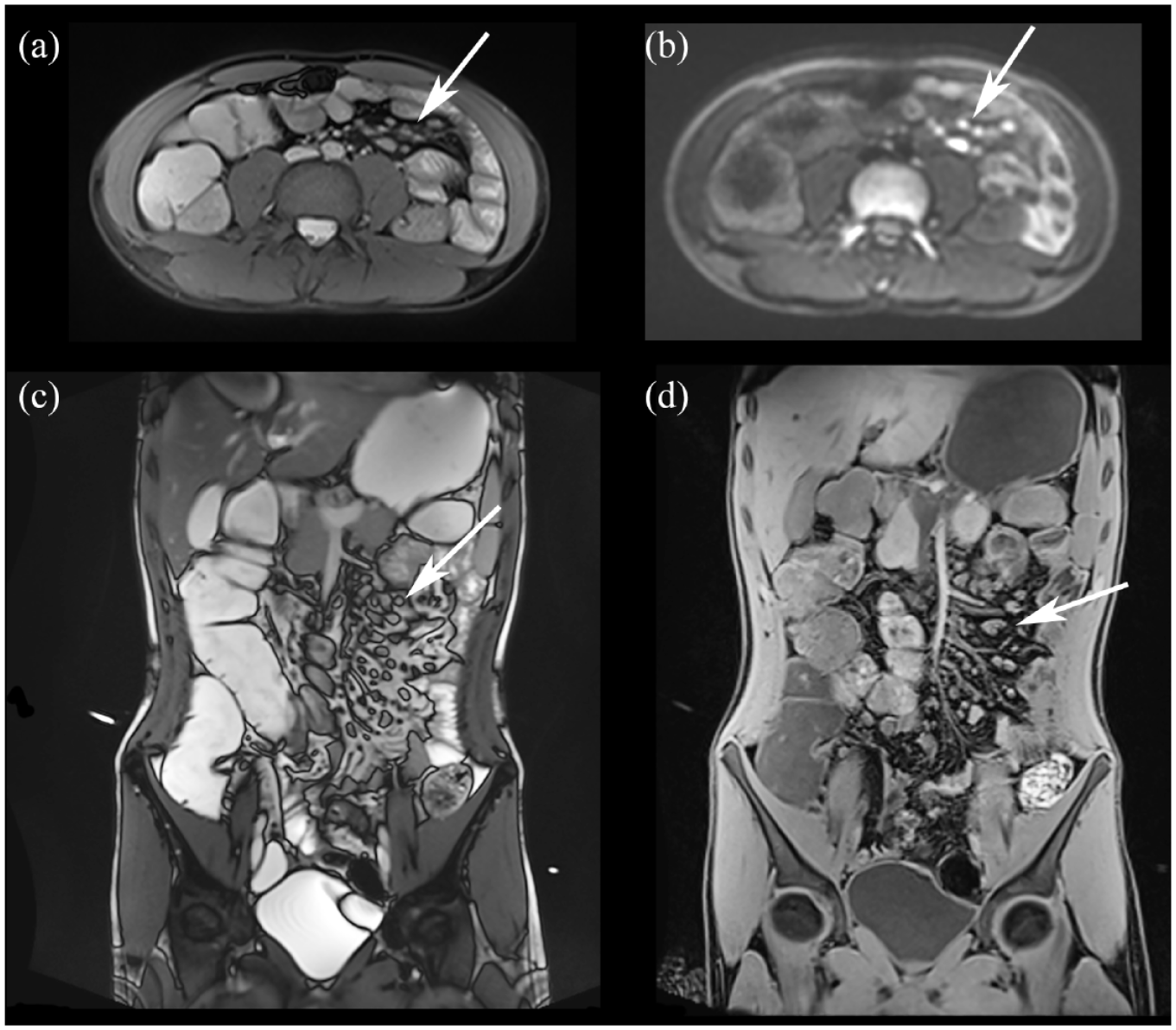
No significant association was found between mean regional Lewis scores at VCE and regional lymph nodes at MRE (mean Lewis score: 886.07 ± 1138.68 versus 367.22 ± 237.16, p = 0.11). Figures 1 and 2 demonstrate the examples of MRE exams in patients with jejunal CD according to VCE.

Thirty-one-year-old male with jejunal involvement of CD according to VCE. Coronal T1-weighted images without (a) and with (b) fat suppression demonstrate mesenteric lymphadenopathy in LUQ adjacent to jejunal bowel segments (black arrows). Note the thickening of a jejunal loop wall. Diffusion (c) and ADC maps (d) demonstrate restriction in the mesenteric lymph nodes (arrows).
Nineteen-year-old male with jejunal CD. Axial T2-weighted image demonstrates multiple mesenteric lymph nodes adjacent to jejunal loops (a. arrow). On diffusion sequence restriction can be seen (b. arrow). Coronal T2-weighted (c) and T1-weighted post-contrast injection (d) demonstrate multiple small lymph nodes in LUQ adjacent to jejunum (arrows).
Discussion
In this study, we evaluated the relationship between regional lymph nodes MRE features and their possible predictive value of jejunal CD. There are several important findings: (1) Presence of inflamed regional lymph nodes in patients with CD was significantly associated with jejunal involvement at VCE. (2) Without assessing lymph node involvement, MRE had low sensitivity to detect proximal bowel involvement. (3) There was no significant association between regional lymph nodes and disease activity according to Lewis scores at VCE.
One of the challenges in MRE when evaluating CD is proximal small bowel disease detection. This is usually due to the suboptimal distention of jejunal loops. It specifically applies to early disease characterized by mucosal changes only. Improving the ability of non-endoscopic methods for proximal disease detection is an unmet need in IBD diagnostics. Here, using lymph nodes MRE features, additional 14 cases of proximal disease were accurately detected, increasing the detection rate of proximal bowel disease at MRE from 4% to 62%.
Radmard et al. 15 were the first to suggest that lymph node features at MRE can be predictive of disease activity. In their study, however, only five patients had jejunal disease. One possible reason to explain the association between regional lymph nodes and CD is the paradigm that the primary pathology in CD involves altered intestinal permeability, bacterial translocation, and inflammation in draining lymph nodes. 19 The impaired regulation of the lymphatic system on inflammation and the immune response contribute to the pathogenesis of CD.20–22 It is therefore possible that regional lymph node imaging features could be more sensitive for disease detection, although less specific, compared to bowel imaging features.
The lack of a significant association between regional lymph nodes at MRE and CD activity according to VCE scores concurs with previous results obtained when using intestinal US. Cohort studies and prospective longitudinal studies have shown that the presence of mesenteric regional lymph nodes does not correlate with clinical and biochemical disease activity in CD. Lymph nodes may persist in CD patients who went into clinical remission after therapy, even after the normalization or improvement of bowel wall thickening.14,23 The presence of regional lymph nodes may therefore be more of an indicator for disease than a reliable parameter of its activity. This feature could be useful to hint on disease localization. It is important to note that mesenteric lymph nodes are non-specific for CD. Other common inflammatory and infectious diseases, such as celiac disease and bacterial enteritides may have enlarged mesenteric regional lymph nodes. On the other hand, MRE in those cases can be the first modality to suggest proximal small bowel disease and justify further investigation of the proximal small bowel by endoscopic measures. Furthermore, it may be valuable to suggest proximal involvement in cases resistant to medical treatment, for follow-up on the evolution of disease in this location, and although non-specific, to suggest the possibility of new IBD diagnosis.
This study has several limitations. First, it is based on a retrospective analysis and results should be interpreted accordingly. Second, we did not evaluate distal bowel disease or compared between proximal and distal disease MRE parameters, as this was not the focus of the current study. Third, difference between imaging techniques and devices exists between the two institutions as described. There were also differences in medical therapies between the institutions as detailed. Fourth, an interval of up to 12 months between the MRE and VCE studies was allowed. Finally, we defined Lewis scores at VCE as our standard reference for presence of disease as well as disease activity. Although considered to have high sensitivity and specificity, proximal disease can be missed or misdiagnosed by VCE.
Conclusion
To conclude, regional mesenteric lymph node assessment at MRE can be valuable to suggest the possibility of proximal bowel disease in patients with CD, even when the proximal bowel looks normal at imaging. Thus, the presence of inflamed-appearing proximal mesenteric lymph nodes at MRE in patients with CD possibly warrants further investigation of the proximal small bowel by endoscopic measures.
Supplemental Material
sj-docx-1-tag-10.1177_17562848221118664 – Supplemental material for Diagnostic significance of mesenteric lymph node involvement in proximal small bowel Crohn’s disease
Supplemental material, sj-docx-1-tag-10.1177_17562848221118664 for Diagnostic significance of mesenteric lymph node involvement in proximal small bowel Crohn’s disease by Giovanni Maconi, Vera Sorin, Uri Kopylov, Oranit Barzilay, Francesca Ferretti, Silvia Innamorati, Massimo Tonolini, Rami Eliakim and Michal Marianne Amitai in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.