
Abstract
Background:
Irritable bowel syndrome (IBS) is characterized by abdominal pain and altered bowel habits. Further, IBS patients experience a high degree of extraintestinal symptoms.
Objectives:
The aim of this review was to describe the relation between IBS and extraintestinal manifestations and mechanisms and treatments of these extraintestinal manifestations.
Design:
The study was performed as a systematic review.
Data Sources and Methods:
Search terms including extraintestinal manifestations or somatization and IBS were used to scrutinize for publications in Pubmed. In total, 630 publications were identified and 80 were finally included in this review.
Results:
About 50% of all IBS patients have extraintestinal manifestations in addition to gastrointestinal symptoms. Somatic pain, fatigue, and sleeping disturbances are most common, and most often described in women. Both extraintestinal manifestations and psychological distress are associated with exaggerated gastrointestinal symptoms, impaired quality of life, and difficulties to treat IBS symptoms. The extraintestinal manifestations render an excess of healthcare costs. Varying etiology and pathophysiology to IBS are discussed, and many patients express a general hypersensitivity. Extraintestinal symptoms are seldom documented at clinical healthcare or included in the assessment of treatment outcomes. A good patient-physician relationship and strengthening of coping mechanisms have rendered less gastrointestinal symptoms, psychological distress, and somatization. Altered lifestyle habits may improve both gastrointestinal and extraintestinal symptoms. Pharmacological treatment, including antidepressant drugs, should be considered when lifestyle advice fails. Teamwork between different specialists and healthcare providers may be of importance in the wide range of symptoms and extraintestinal manifestations.
Conclusion:
Extraintestinal manifestations are common in IBS patients and is associated with worse suffering and difficulties to treat symptoms. Evaluation and treatment of IBS patients should consider also extraintestinal manifestations and their treatment outcome. Establishment of good relationship, strengthening of coping mechanisms, and education in healthier lifestyle habits are crucial in the management of these patients.
Keywords
Background
Irritable bowel syndrome (IBS) is defined as abdominal pain at least once weekly, associated with defecation, altered stool frequency, and/or altered stool consistency. 1 IBS is the most frequent and well known of the disorders of gut–brain interaction (DGBI), with a worldwide pooled prevalence of 4.1% (range: 1.3–7.6%) according to the Rome IV criteria. 2 The prevalence of IBS was higher when Rome II and Rome III criteria were used to define the condition, 3 and the most studies in the literature reflect these former criteria. Female sex, lower middle age, stress, psychological factors, and certain lifestyle habits are associated with IBS. 4 The etiology to IBS is unknown but suspected to be multifactorial. Dietary intake of unabsorbed carbohydrates, gut microbiota dysbiosis, and low-grade inflammation are some factors that have been considered in the pathophysiology. 5 Visceral and somatic hypersensitivity has been widely discussed in IBS, 6 especially since IBS is associated with chronic fatigue, fibromyalgia, and other extraintestinal pain syndromes.7,8 A term often referred to in these circumstances is somatization disorders, a psychiatric diagnosis defined by explicit criteria. This should be distinguished from the tendency to report somatic complaints, measured by psychological tests of somatization. The present overview about extraintestinal manifestations in IBS is to report somatic complaints and not somatization disorders.7,8
IBS patients may be referred to several departments for their extraintestinal manifestations to undergo invasive investigations, before IBS is recognized, which may further aggravate their symptoms. 9 Thus, extraintestinal symptoms in IBS need to be recognized and handled appropriately. The aims of the present review were (a) to describe the comorbidity between IBS and extraintestinal manifestations; (b) to explore the mechanisms behind this comorbidity; and (c) to discuss the treatment of extraintestinal manifestations.
Methods
A search was performed on 15 October 2021 in Pubmed with the research terms ‘extraintestinal symptoms and IBS’ which rendered 114 publications. The term ‘symptoms’ rendered more publications than ‘manifestations’ (20 publications), why the term symptoms was used. A new search strategy was performed on 21 October with the term ‘treatment of extraintestinal symptoms in IBS’ which rendered 49 publications. On 30 May 2022, the search strategies ‘somatization and irritable bowel syndrome’ rendered 261 publications, ‘extraintestinal symptoms and irritable bowel syndrome’ rendered 173 publications, ‘non-colonic symptoms and irritable bowel syndrome’ rendered 15 publications, and ‘extra-colonic symptoms and irritable bowel syndrome’ rendered 6 publications. Altogether, 618 articles were found in the search strategies. In all, 12 further publications were found from their reference lists or other sources. After scrutinizing titles and abstracts, 99 full-length-articles were read by the author and evaluated according to the Newcastle–Ottawa Scale for cohort and case–control studies when applicable. 10 Inclusion criteria were original or review articles written in English describing the presence of extraintestinal symptoms in IBS, mechanisms behind extraintestinal symptoms in IBS, and/or treatment of extraintestinal symptoms in IBS. Extraintestinal symptoms referred to somatic complaints including fatigue. Exclusion criteria were animal studies, articles not available in full length, conference abstracts, editorials, letters to the editor, or articles describing only psychological or psychiatric diseases. After removal of duplicates and publications not fulfilling the inclusion criteria, 80 remained which were finally included in the review (Figure 1). Articles describing the prevalence of extraintestinal manifestations in IBS cohorts are listed in Table 1. Other articles not including the prevalence of the manifestations in the cohorts are listed in Table 2.

Flow chart according to PRISMA.
Description of studies that report the prevalence of extraintestinal manifestations.

IBS, irritable bowel syndrome.
Description of the other studies included in the review.
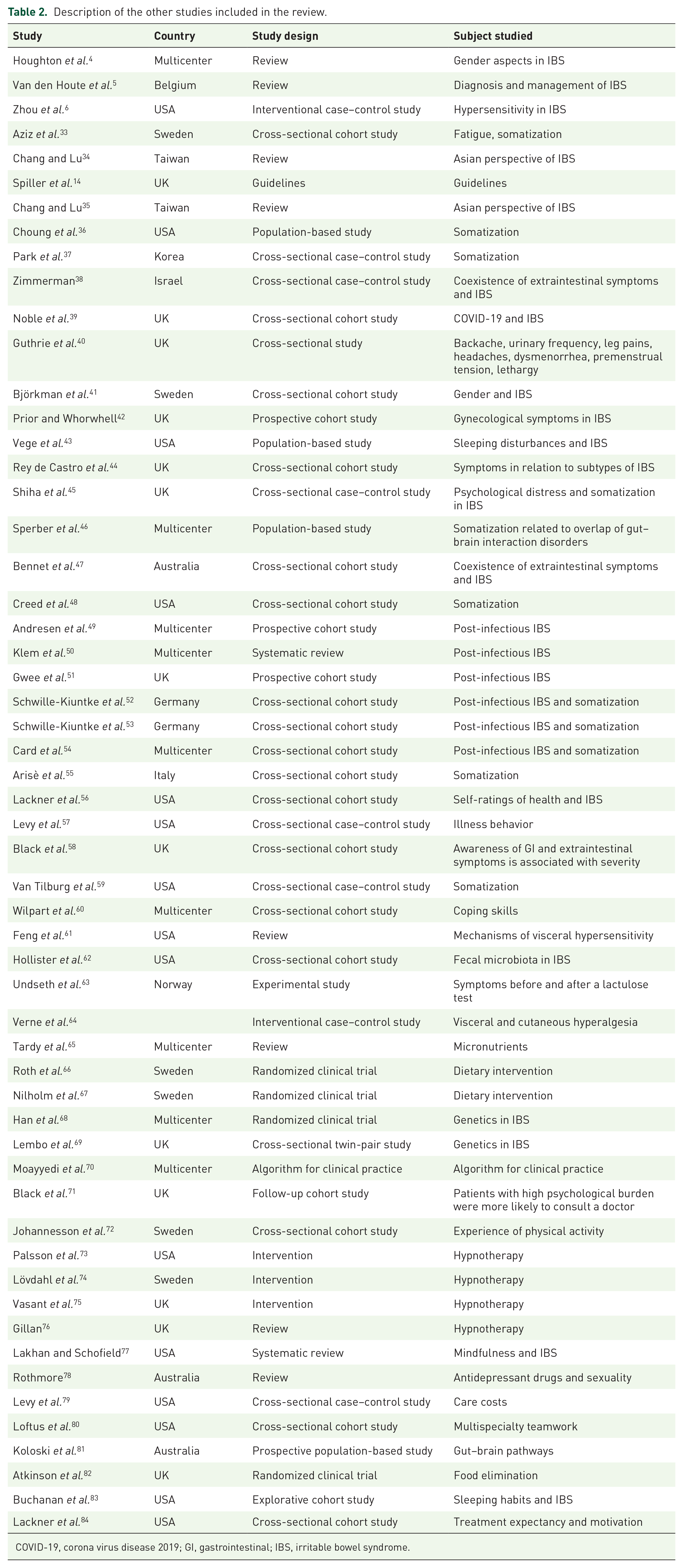
COVID-19, corona virus disease 2019; GI, gastrointestinal; IBS, irritable bowel syndrome.
Main text
Extraintestinal manifestations
The criteria and diagnosis of IBS are based on symptoms in the absence of organic alterations. IBS is divided into constipation-predominant IBS (IBS-C), diarrhea-predominant IBS (IBS-D), IBS with mixed bowel habits (IBS-M), and unclassified IBS. 1 The Rome criteria have changed over time, rendering some differences between IBS patients diagnosed at different time points. 2 Thus, IBS patients diagnosed according to Rome IV had increased severity of gastrointestinal (GI) symptoms, somatization, and fatigue than those diagnosed according to Rome III. 33 About 50% of all IBS patients have sole IBS; the rest have any kind of additional somatic and/or mental symptoms. 7 A list of common extraintestinal manifestations (syndromes and symptoms) in IBS is shown in Table 3.
Extraintestinal syndromes and symptoms reported in increased prevalence in IBS.
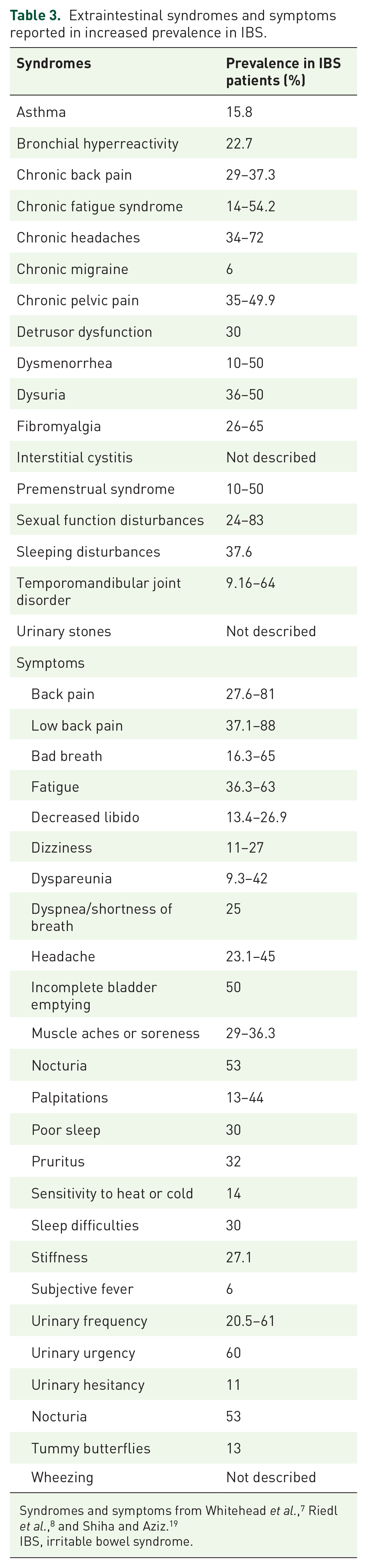
IBS, irritable bowel syndrome.
The prevalence of extraintestinal manifestations is much higher in IBS than in organic GI disorders,8,11 and about twice as common as compared to control groups in adults.7,12–19,34,35 Not only the prevalence of somatization is increased, also the severity of somatization is higher in IBS than in controls20,21,36 and in organic GI disorders. 37 The prevalence of extraintestinal manifestations is also much higher in children and adolescents with IBS compared to controls, especially in girls and in children exposed to stressful events.22,23 In a cohort of elder patients (65–94 years), the prevalence of extraintestinal symptoms was much higher in IBS patients than in other patient groups. 24 The intestinal symptom reflux was the strongest predictor of extraintestinal symptoms. 37 Both GI and extraintestinal symptoms were scored higher after the corona virus disease 2019 pandemic than prior to the pandemic. 38 In general, there is an increased risk for IBS individuals to develop any extraintestinal manifestations over time. 25 In accordance, both GI symptoms and extraintestinal symptoms are perceived more severe in chronic attenders to a tertiary center than in first-time attenders. 39 Not only the prevalence of IBS is more frequent in women than in men, also the prevalence and severity of extraintestinal manifestations in IBS is highest in women.4,37,40
Back pain, chronic fatigue, fibromyalgia, headache, pelvic pain, sleeping disturbances, and urogenital symptoms are the most common manifestations, occurring in 34–50% of IBS patients (Table 3).7,8,21 Many IBS patients attend to a gynecologic department because of pelvic pain, without having any gynecologic diagnosis. 41 Fatigue is by some authors suggested to be the most common extraintestinal manifestation and has great impact on GI symptoms, psychological stress, and quality of life. 26 Fatigue is more common in IBS patients from tertiary centers than from primary centers, and more common in females and at younger age. 26
On the other hand, patients with chronic fatigue syndrome have a 35–92% prevalence of IBS.18,27 Fibromyalgia was associated with a 1.54-fold increased risk of having IBS according to a national database, 19 whereas a review showed that 32% of women with fibromyalgia had IBS. 18 Up to 40% of patients with chronic pelvic pain fulfilled diagnostic criteria for IBS, and patients with migraine had IBS twice as often than those without migraine.17–19 Patients with endometriosis have a two- to three-fold increased risk of IBS compared with controls and patients with interstitial cystitis have an 11-fold increased risk to have IBS compared with controls. 19 About half of the patients with sexual dysfunction also suffered from IBS.18,19 Furthermore, 40–50% of patients attending a urologic department also suffered from IBS, in addition to urologic symptoms. 85 Asthma patients reported a 20% increase in the incidence of IBS, whereas patients with anxiety and depression have a two-fold increased risk for the onset of IBS. 19 In a population-based study, those reporting sleeping disturbances had an IBS prevalence of 33% compared to 13% in the others. 42
Most studies have shown that the distribution of extraintestinal manifestations is equal between subgroups,23,28,43 whereas one study reported that somatization was most pronounced in IBS-M, 21 and one study showed that sleeping disturbances were associated with IBS-D but not IBS-C. 42 One study showed that IBS patients had a greater number of somatic symptoms and higher somatization level than patients with functional constipation and functional diarrhea. 44 IBS diagnosed according to Rome IV criteria exhibited more severe disease and more somatoform symptoms than IBS diagnosed by a physician. 86 Overlap of DGBI-affected GI regions was associated with extraintestinal symptoms.45,84 In line with this, extraintestinal manifestations were predictive for the combination of functional dyspepsia and IBS. 46 IBS patients at tertiary centers have more severe disease and other comorbidities compared with IBS patients at primary care. 26 The patients with highest degree of somatization were older with less education and were more likely to be unemployed compared with those IBS patients with lower scores of somatizations. 47
Infectious enteritis is a well-known risk factor to develop IBS. Somatization at the time point for the infection was associated with an increased risk to develop post-infectious IBS in two studies48,49 but not in a third study. 50 In follow-up of patient cohorts with infectious enteritis, those who had developed IBS scored higher in somatization than those who had not developed IBS.51,52 Patients with post-infectious IBS had higher somatization scores than other IBS patients, and those post-infectious IBS patients with high somatization scores had lower recovery rates than those with low somatization scores. 53
The more comorbidity, the worse quality of life and psychological distress; and the more extraintestinal and psychiatric comorbidity, the more GI symptoms and difficulties to successfully treat the IBS symptoms.7,8,18,27,29,47,54 The patients’ self-ratings of health were associated with fatigue and the number of medically unexplained somatic complaints. 55 The high levels of symptom burden render twice as many healthcare visits for IBS patients compared with age-matched controls, and 78% of extra healthcare visits from IBS patients depend on extraintestinal manifestations and not GI symptoms.36,56
Mechanisms of extraintestinal manifestations
Etiology
The etiology behind IBS and extraintestinal manifestations are multifactorial. Several hypotheses have been proposed to explain the overlap and comorbidity between IBS and other syndromes. One hypothesis is that they are all vague syndromes with overlapping symptoms but without specific organic characteristics. A visit to a gastroenterologist renders the IBS diagnosis, but a visit to another specialist renders another diagnosis.
Both physiological and cognitive/psychological processes may give rise to GI and extraintestinal symptoms. IBS patients and other patients with extraintestinal manifestations have a high degree of psychological distress and psychiatric diseases, which can affect the experience of different somatic symptoms.7,8,27,29 The tendency to report or experience both GI and extraintestinal symptoms seems to be the central driver to severity of IBS symptoms. 57 The tendency of somatization may depend on social and behavior learning during childhood, which play a great role in these conditions. 7 Children to mothers with IBS had higher somatization scores than children to mothers without IBS. 58 However, the occurrence of several IBS cases within the same family may also include genetic components.87,88 Different subgroups may have varying etiology, but the body may react similarly to several different stimuli. On the other hand, all patient groups may get anxiety and depression secondary to other symptoms. Theoretically, there may be a more obvious biological etiology to IBS without comorbidity, and more psychological etiology to IBS with symptoms from multiple organs. However, this dualistic mind–body dichotomization is complex, and many researchers are approaching a more holistic biopsychosocial view. Phenomenon in the central nervous system involved in central sensitization involves etiological mechanisms that might explain multisystem symptoms, which can not only be viewed as psychological features.
Studies report that IBS patients with several extraintestinal manifestations have more often a history of sexual or physical abuse than IBS patients with sole GI symptoms.7,8 Coping is defined as a process of efforts to manage stressful life events. 89 Coping resources are both individual psychological resources within the subject and interindividual resources in the form of social support and acceptance, and the possibility to practice activities that gain the health, like exercise and healthy lifestyle habits. Coping mechanisms may be adaptive or maladaptive. Impaired coping mechanisms have been reported in IBS patients, with more escape-avoiding strategies than planful problem solving. 90 Anxiety, GI-specific anxiety, and depression were associated with less efficient coping mechanisms. 59
Pathophysiology
Regarding the pathophysiology, several biological models have been suggested, such as low-grade inflammation, altered microbiome, increased intestinal permeability, and motility disturbances.1,5 Activation of nociceptive receptors is a physiological protection from harm. The International Association for the Study of Pain 91 defines pain as an unpleasant sensory and emotional experience associated with actual or potential tissue damage, which means that experience of pain does not necessarily mean a true tissue damage. Afferent signals are transmitted through the dorsal horn and further trunks into the cortex. In cortex, the information is interpreted in relation to other sources of information and cognitive and psychological factors. 30 Efferent pain trunks then inhibit or facilitate the afferent transmission of pain, to modulate the nociceptive pathways at different levels.92,93 Higher levels of anxiety, stress, and pain catastrophizing are associated with reduced conditioned pain modulation in IBS. 30 When normal stimulus is experienced as pain, it is called allodynia, whereas exaggerated pain is called hyperalgesia. Hypersensitivity is a collective description of abnormal pain modulation and may be peripheral, due to increased excitability (i.e. sensitization) of nociceptors, or central, the latter divided into spinal cord processes or descending pain modulation.6,92,94 Low-grade inflammation is described in multiple studies of IBS, which may render peripheral hypersensitivity through neuroendocrine and immunological imbalance that may influence pain modulation and perception. 60 Pro-inflammatory and lipotoxic lipids, mast cells and their products, enteroendocrine cells, and mononuclear phagocytes are involved, and among many neurotransmitters, substance P, calcitonin gene-related peptide, 5-hydroxytrytamine, transient receptor potential vanilloid, and glutamate deserve to be mentioned. 60 Other mechanisms may be traumatic neuropathy or myopathy. Even extraintestinal manifestations, for example, fatigue is associated with low-grade inflammation and related biomarkers.26,31 Associations have also been found between increased urgency and extraintestinal pain and lower microbial diversity and richness in feces in women with IBS. 61 Nevertheless, studies have failed to explain the increased extraintestinal symptoms after a lactulose test to be caused by mucosal damage. 62
Cognitive functions, mood disorders, and fatigue are more involved in central than in peripheral hypersensitivity.26,30 Widespread hypersensitivity in IBS with comorbidity and extraintestinal manifestations suggest central rather than peripheral hypersensitivity. However, almost all chronic complaints are initiated by peripheral sensory neurons. 60 Central hypersensitivity is characterized by an increased membrane excitability, a facilitated synaptic strength, and/or a decreased inhibitory influence on dorsal horn neurons and contributes to abnormal responsiveness to noxious and innocuous stimuli and a tenderness in several visceral and somatic organs.92,94 Functional magnetic resonance imaging has described involvement of augmented pain processing also in cortical and subcortical structures, 94 and associations between fatigue and connectivity within a mesocorticolimbic network. 31
In IBS, both widespread visceral and somatic hypersensitivity may be present,6,60 and somatization is associated with more visceral hypersensitivity 95 and anxiety and depression. 54 When examining cold and heat pain, pressure pain, and ischemic pain, IBS patients could be divided into one group with normal pain thresholds and one group with reduced thresholds. Interestingly, the thresholds were lower in foot than in hand, and the lower cold and ischemic thresholds were accompanied with higher systolic blood pressure and higher circulating levels of corticotrophin and cortisol. 6 Associations between blood pressure, cortisol, and hypersensitivity suggest a disturbed hypothalamic–pituitary–adrenal axis in IBS patients, 96 possibly due to a higher stress level. The coexistence of hypersensitivity in several visceral organs, that is, cross sensitization, along with somatic hypersensitivity, is explained by the proximity between visceral organs and the organization of the enteric nervous system, and a viscerosomatic convergence at the spinal cord level and at higher brain centers. 97 The more pronounced hypersensitivity in lower extremities may be explained by more afferent convergence at spinal cord level with colon and lower extremities than with upper extremities. 63
Several animal models have shown that high intake of fat and/or sugar has led to hyperglycemia, insulin resistance, metabolic disturbances, and histopathological changes with nerve super excitability. 98 Recently, poor dietary habits have been described in IBS patients in several countries.65,99–101 Vitamins and minerals act as cofactors in multiple processes in the cells. It is well described how micronutrient deficiency leads to impaired cognitive and psychological functions, including mental and physical fatigue, weakness, and muscle pain. 64 Improvement of dietary habits in IBS with lower intake of candies and sugar rendered lower levels of weight, GI symptoms, extraintestinal symptoms, and levels of C-peptide, insulin, gastric inhibitory polypeptide, and leptin,66,100,102 in parallel with reduced weight and improved endocrine and metabolic profile during a similar diet in type 2 diabetes. 103 Thus, the painful syndromes may depend on neuropathy secondary to disturbed homeostasis in the nerves and surrounding tissues. 98
Even if the extraintestinal manifestations are not primarily explained by genetic influences, there is evidence of a genetic component in the associations between IBS and extraintestinal symptoms. 67 The associations between IBS and extraintestinal manifestations in twins may depend on both genetic and environmental conditions.32,68 Recently, a genome-wide analysis of 53,400 subjects with IBS showed shared genetic pathways for IBS, anxiety, depression, and neuroticism. 104
Treatment of extraintestinal manifestations
Classification systems of IBS and treatment guidelines do not consider extraintestinal or psychological symptoms in their statements.1,69 Although it has been shown that both presence of extraintestinal manifestations and psychological comorbidity are associated with more severe GI symptoms,7,8,29,85 few studies assess the effect of the treatment on extraintestinal manifestations in addition to the GI symptoms. 19 Most studies only use GI symptoms to measure the outcome of efficiency, but many also include psychological assessments. Furthermore, the varying definitions of IBS and extraintestinal manifestations, as well as varying evaluation scores of extraintestinal manifestations, may complicate the conclusions of efficiency of different treatments. 26 The parallel severity between GI and extraintestinal symptoms suggest that treatments improving GI symptoms should also improve extraintestinal symptoms. However, this must be proven. In prospective follow-up studies, it has been shown that about half of the IBS patients remained in their original clusters over time, when the clusters were stratified by stool pattern. 70 On the contrary, 84% of IBS patients in the cluster with a high psychological comorbidity remained in this cluster at follow-up, with more severe GI symptoms and a higher number of consultations and treatments commenced. 70 Still, very few of these patients are considered for psychological treatment in daily practice.
The most important in all IBS treatment is to establish a strong patient–physician relationship. 69 It is important to inform the patient about the physiological and pathophysiological mechanisms, and to explain the mechanisms in a patient-friendly way. Better physical coping was associated with less GI symptoms, and lower levels of physical and psychological coping were associated with more extraintestinal symptoms, mediated through anxiety and depressive symptoms. 59
Next step is to penetrate lifestyle habits and give advice about healthy dietary habits and physical activity. In the IBS-severity scoring system (IBS-SSS) questionnaire, also 10 extraintestinal symptoms are measured, namely, nausea, early satiety/difficulty to eat a whole portion, reflux/heartburn, belching/excess wind, headache, back pain, thigh pain, muscle/joint pain, urinary emergency, and tiredness/lethargy.66,105 In a clinical trial with starch and sucrose-reduced diet, 74% of the patients were responders regarding GI symptoms. In addition, the total IBS-SSS for extraintestinal symptoms was reduced in the intervention group compared with the control group, as were the individual symptoms belching/excess wind, muscle/joint pain, urinary emergency, and tiredness/lethargy. 66 The improvement of extraintestinal symptoms correlated with the improvement of total GI symptoms and psychological well-being. Decreased cereal intake correlated with decreased belching/excess wind, and decreased intake of sweets/soft drinks correlated with decreased belching/excess wind and tiredness/lethargy. 66 Treatment with low Fermentable Oligo-, Di-, Mono- saccharides And Polyols has shown similar results in the effect on fibromyalgia. 19 Physical activity has documented effect both on GI and on extraintestinal symptoms. 71
If lifestyle advice is not enough, pharmacological treatment could be prescribed; the choice of treatment depending on the most prominent symptom. 69 Antidepressants are widely used to treat abdominal pain, global IBS symptoms, and several extraintestinal manifestations.8,69
A comprehensive self-management (CSM) intervention model in IBS covered the topics education, diet, relaxation, and cognitive-behavioral strategies. The effect of this intervention on extraintestinal pain, fatigue, and sleep disturbances was studied in a randomized controlled trial. CSM led to almost as large effects on backache, headache, and joint pain, as well as decreased fatigue and sleeping disturbances as on GI symptoms. 28
The use of individual hypnotherapy has been shown to be efficient to decrease extraintestinal symptoms and somatization, although performed without any control group.72–74 In a systematic review of group and self-help hypnotherapy, only one of the found studies had assessed the outcome on extraintestinal symptoms and could not demonstrate any effect of hypnotherapy on somatization or extraintestinal symptoms. 75 Mindfulness-based therapy has been found to be efficient in several entities: GI symptoms in IBS, fibromyalgia, and fatigue. 76 Psychological treatment of somatic complaints is more effective in patients at tertiary healthcare centers than in the community, 14 and most efficient in IBS patients with the highest scores of somatization and symptoms. 47
Regarding the treatment of fibromyalgia, exercise, psychological therapy, pharmacotherapy, and/or multimodal rehabilitation programs are suggested by rheumatic guidelines. 19 Observational studies have proposed fecal transplantation as a treatment of fatigue, 19 but the close relationship between fatigue and eating habits and low physical activity suggests changes in lifestyle habits as an important treatment option. 26 Patients with both temporomandibular disorders and IBS have high levels of anxiety, depression, fatigue, and sleeping disturbances, and a multidisciplinary treatment is more successful than separate treatments. 19 Concerning interstitial cystitis, a multidisciplinary team involving urologists, gastroenterologists, and psychologists is recommended. 19 IBS is many times treated with antidepressants, which may lead to sexual dysfunction. 77 Thus, withdrawal of medicals may be the first treatment option in sexual dysfunction. Due to a relationship between poor sleeping quality and visceral hypersensitivity, a low dose of tricyclic antidepressants may be efficient against sleeping disorders. 19
Future treatment
Independent of etiology and pathophysiology, we must handle these patients without any organic abnormalities at routine care examinations but with a general high level of stress and pain. These conditions render a high degree of suffering from the patients, and they constitute a great part of healthcare costs. Since extraintestinal manifestations have greater impact on quality of life and treatment responsiveness than GI symptoms,27,29 and most of the excess in healthcare costs for IBS patients resulted from care not directly related to GI symptoms, 78 it is of great interest both for the patients and for the society to consider extraintestinal manifestations as well as GI symptoms. 15
A clear discrepancy between the patients’ experience of symptoms and the physicians’ views of the symptoms is at hand.4,106 The most important in the handling of the patients is to confirm the patient and mediate that the patient’s symptoms are taken seriously. 107 All mental and somatic symptoms must be considered, documented, and borne in mind when planning the treatment.27,29,105,108 A holistic approach with a team representing different professions is needed to objectively assess the most troublesome symptom/disease and to create a proper therapeutic attitude toward the patients. 107 Not only specialists in gastroenterology should be involved, also specialists in gynecology, neurology, psychiatry, and rheumatology may be of importance to create a full picture of the patient’s need. 79
The question is whether we are talking about one disease with several different aspects and modes of presentation, or whether we are talking about different diseases. The explanations of sensitization and hypersensitivity point to a common, generalized increase in experience of pain and discomfort. Central sensitization, mood disturbances, learned behavior, the autonomic nervous system, the immune system, and the gut–brain axis may be involved.6,7,30 The presence of concomitant multiple disorders characterized by pain and subjective experiences point to psychological influences in the etiology. 7 Even if some of the extraintestinal manifestations have independent etiologies, they must have something in common since they overlap to such a high degree regarding female predominance, fatigue, sleeping disturbances, and anxiety. 7 The important question is what comes first, IBS or psychological discomfort. In efforts to prospectively study these mechanisms in IBS, independent gut-to-brain and brain-to-gut pathways have been described. Both anxiety and depression at baseline were predictors to develop IBS, and IBS patients without anxiety and depression at baseline reported higher levels of these conditions at follow-up. 80 The common genetic pathways to IBS and mood disorders may explain the coexistence of IBS and psychological discomfort. 32 Apart from different subgroups of IBS, 1 there are also differences between IBS patients depending on the mode of recruitment and inclusion in clinical trials, and whether the patients are recruited from primary or tertiary healthcare centers.2,26,86
A dietary intervention with less sugar and starch improved both GI symptoms and extraintestinal symptoms, as well as psychological well-being.65,66 Elimination of foods, which the patients expressed directed antibodies against, also reduced both GI and extraintestinal symptoms. 81 Furthermore, increased physical activity has also led to improvement of extraintestinal symptoms. 71 These improvements stress how important it is to improve poor lifestyle habits described in the IBS populations with low intake of important nutrients,65,99–101 especially before more potential investigations and treatments are prescribed. In the future, more efforts must be done to enhance the knowledge about healthy lifestyle habits, which is crucial for the general health in the whole society. Thus, exclusion of malnutrition, especially micronutrients, is of great importance in these entities. 64
The efficacy of group and self-help hypnotherapy on extraintestinal manifestations in IBS has not been settled. 75 Reductions in extraintestinal symptoms may indirectly improve GI symptoms, since for example, sleep measures predict next-day symptoms of IBS. 82 The effect of cognitive behavioral therapy and mindfulness have not been studied sufficiently but could be of interest to improve coping mechanisms, since the most predictive factors for a positive treatment were interpersonal support, motivation for improvement of symptoms, and expectancy of improvement.76,83 Thus, more efforts should be put into treatments to strengthen the individual coping mechanisms and enhance the motivation for self-management.28,59
Linaclotide, efficient in constipation treatment, also normalized the bladder function through indirect inhibition of bladder afferents in a mouse model, 109 supporting the concepts that pharmaceutical treatments may inhibit cross-organ sensitization through common sensory pathways. Further studies are warranted in this area to prove evidence in clinical practice.
Conclusion
Future research studies and healthcare must consider not only GI symptoms, but also extraintestinal manifestations in IBS, and assess both the magnitude of extraintestinal symptoms and the effect of interventions on these symptoms. Both the subjective experience for the patients and the healthcare resources and costs for the society are considerable for extraintestinal manifestations and must be considered. Good relationship between caregivers and patients and support of coping mechanisms in the patients are crucial. More efforts are needed to bring the society into a healthier lifestyle regarding diet and physical activity to prevent or improve IBS and related extraintestinal manifestations. The efficiency of pharmacological treatment on extraintestinal manifestations must be evaluated.
Supplemental Material
sj-docx-1-tag-10.1177_17562848221114558 – Supplemental material for Extraintestinal manifestations in irritable bowel syndrome: A systematic review
Supplemental material, sj-docx-1-tag-10.1177_17562848221114558 for Extraintestinal manifestations in irritable bowel syndrome: A systematic review by Bodil Ohlsson in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.