
Abstract
Background:
The efficacy of tofacitinib (TOFA) in various rheumatic diseases has generated interest in its potential benefits for treating spondyloarthritis (SpA) associated with ulcerative colitis (UC).
Objectives:
RETUCAS (Real-world Effectiveness of Tofacitinib on Ulcerative Colitis-Associated Spondyloarthropathy) is the first study designed to evaluate the effectiveness of TOFA in UC-associated SpA.
Design:
This was a prospective, multicentre, single-arm, observational study promoted by the Italian Group for the Study of Inflammatory Bowel Disease. Effectiveness was assessed using standardized rheumatologic scores.
Methods:
Patients with UC and a confirmed diagnosis of active axial or peripheral SpA at baseline were enrolled. The primary endpoint was steroid-free joint response (SFJR) at weeks 8 and 52, defined as a decrease of ⩾1.1 units in Ankylosing Spondylitis Disease Activity Score-C-Reactive Protein (CRP) for axial SpA, or a decrease of >0.6 units in Disease Activity Score 28-CRP for peripheral SpA, without the use of corticosteroids.
Results:
A total of 44 patients were enrolled: axial SpA: 9.1%; peripheral SpA: 70.4%; mixed axial and peripheral SpA: 20.5% All but two patients had previous exposure to biologic therapies, with more than half having failed two or more biologics. At week 8, SFJR was achieved in 52.3% of patients, with a significant difference between those with peripheral SpA and those with axial or mixed forms (67.7% vs 15.4%; p = 0.001). At week 52, SFJR was maintained in 59.1% of patients overall, again with better outcomes in peripheral SpA compared to axial/mixed SpA (71.0% vs 30.8%; p = 0.01).
Conclusion:
This is the first prospective study specifically designed to assess Inflammatory Bowel Diseases-associated SpA. In patients with UC and refractory SpA—many of whom had previously failed multiple biologic therapies—TOFA demonstrated effectiveness, particularly in those with peripheral SpA.
Plain language summary
People with ulcerative colitis (UC) often experience joint inflammation, a condition known as spondyloarthritis (SpA). This study looked at whether a medication called tofacitinib, already used for UC and some joint diseases, could also help manage joint problems linked to UC. Researchers across multiple centers in Italy followed 44 patients with UC and active joint symptoms (either in the spine, limbs, or both) who started taking tofacitinib. They checked whether the patients’ joint symptoms improved without needing steroids after 8 weeks and again after 1 year. After 8 weeks, about half of the patients showed improvement without using steroids. The results were more positive in patients with joint problems in the limbs (called peripheral SpA) compared to those with spinal involvement (axial SpA). After 1 year, around 6 in 10 patients had improved, again with better results seen in peripheral SpA. This is the first study focused specifically on UC-related joint inflammation using rheumatology-specific tools. It suggests that tofacitinib can be effective for joint symptoms, especially in the limbs, in patients with UC who have not responded to other treatments.
Introduction
Tofacitinib (TOFA) is a JAK inhibitor that has demonstrated efficacy in patients with rheumatoid arthritis,1–3 psoriatic arthritis,4,5 and ankylosing spondylitis. 6 In the field of Inflammatory Bowel Disease (IBD), TOFA has been approved by both the FDA and EMA for the treatment of moderate-to-severe ulcerative colitis (UC) in patients who failed to respond, lost response, or were intolerant to either conventional therapy or biologic agents. 7 This approval was based on the efficacy demonstrated in the OCTAVE trials, 8 and its effectiveness in clinical practice has been confirmed by real-world studies. 9
However, the OCTAVE trials were not designed to evaluate TOFA’s efficacy in treating extraintestinal manifestations, which affect up to 50% of IBD patients.10–13 This high prevalence highlights the systemic nature of IBD, which extends beyond the gastrointestinal tract. Among extraintestinal manifestations, spondyloarthropathy (SpA) is the most common. Ankylosing spondylitis affects approximately 3% of IBD patients, sacroiliitis 10%, and peripheral arthritis 13%. 14
Given TOFA’s efficacy in rheumatologic diseases, there were high expectations regarding its potential benefit in UC-associated SpA. Expert panels have advocated its use for both axial and peripheral SpA. 15 However, data on its effectiveness in this setting remain limited. Current evidence is based on a small number of patients included in post-hoc analyses of the OCTAVE Induction 1, Induction 2, and Sustain trials. 16 anecdotal real-world reports,17–22 and a recent multicenter Spanish study. 23 Notably, none of these studies used rigorous scoring systems or validated indices to diagnose SpA or assess articular response.
To address this gap, we designed a prospective, multicenter, observational 52-week study to assess the effectiveness of TOFA in UC-associated SpA. Articular response was evaluated using rheumatologic scores.
Materials and methods
Study design and patient population
Real-world effectiveness of tofacitinib on ulcerative colitis-associated spondyloarthropathy (RETUCAS) is a prospective, multicentre, single-arm, observational study evaluating the effectiveness of TOFA on UC-associated SpA over a 52-week period (Figure 1). This study was initiated and promoted by the Italian Group for the Study of Inflammatory Bowel Diseases (IG-IBD).
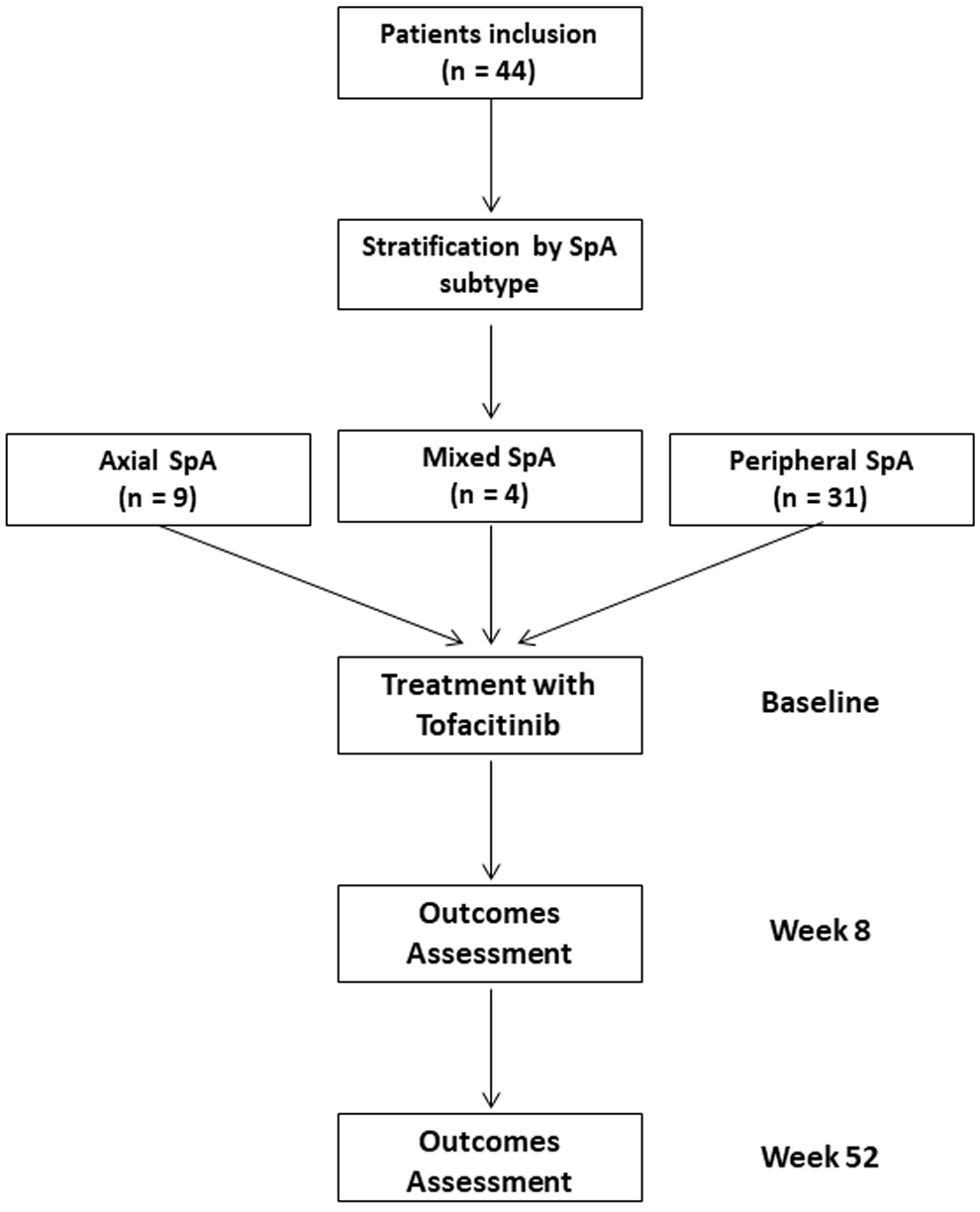
Study flow diagram.
Patients were consecutively recruited at 14 IBD centers in Italy from March 2022 to March 2023. The inclusion criteria were: (I) age greater than or equal to 18 years; (II) an established diagnosis of active UC as previously described 24 ; (III) an established diagnosis of SpA strictly according to the Assessment of Spondyloarthritis International Society (ASAS) criteria.25,26 In particular, patients were stratified into three subgroups: (1) axial SpA, in case of predominant involvement of the axial skeleton, without peripheral symptoms; (2) peripheral SpA, in patients presenting primarily with arthritis, enthesitis, or dactylitis without axial involvement; (3) mixed SpA, in case of significant clinical features of both axial and peripheral involvement; (IV) indication for treatment with TOFA as a therapy for UC according to the clinical practice and summary of product characteristics; (V) active SpA at baseline assessed with an Ankylosing Spondylitis Disease Activity Score–C-Reactive Protein (ASDAS-CRP) ⩾1.3 in case of axial SpA, and with a disease activity score (DAS)28-CRP ⩾2.6 in case of peripheral SpA; (VI) capability to express a written informed consent for the study. Exclusion criteria were: (I) rheumatologic diseases other than UC-associated SpA; (II) inactive SpA at baseline; (III) contraindications to treatment with TOFA (pregnancy, risk factors for venous thromboembolism, and active infections).
Patients initiating TOFA received an induction regimen of 10 mg bi-daily (BID) for the first 8 weeks, followed by a maintenance treatment of 5 mg BID. In case of unsatisfactory response after 8 weeks, patients could receive TOFA 10 mg BID for an additional 8 weeks. Dose optimization (i.e., from 5 mg BID to 10 mg BID) in case of loss of response during maintenance was also allowed at the discretion of the treating physician. In line with the observational design of the study, no standardized protocol for steroid tapering was planned for patients who were on steroids at baseline.
At baseline, all enrolled patients underwent a detailed assessment including age, gender, duration of disease, smoking status, extension of disease (according to Montreal classification), clinical activity (assessed with the partial Mayo score), CRP values, fecal calprotectin, previous and concomitant therapies, data on active SpA (axial vs peripheral vs combined axial and peripheral (mixed) SpA, and assessment of ASDAS-CRP and/or DAS28-CRP).
The protocol was examined and approved by the local ethics committee (Palermo 2). All authors had access to the study data and reviewed and approved the final manuscript. Study data were collected and managed using REDCap electronic data capture tools. 27 The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement (Supplemental Material). 28
Definitions and outcome measures
The primary endpoint was the rate of patients achieving a steroid-free joint response (SFJR) at weeks 8 and 52. SFJR was defined by a decrease of ⩾1.1 units of ASDAS-CRP for axial SpA, 29 and a decrease of >0.6 units of DAS28-CRP for peripheral SpA compared with baseline 30 with no steroid use.
The secondary endpoints included the UC clinical response (CR—defined as a reduction of at least 3 points in the partial Mayo score for UC compared to baseline), and the UC steroid-free clinical remission (SFCR—defined as a partial Mayo score for UC ⩽2 without steroid use).
Statistics
Continuous variables were expressed as mean and standard deviation (SD) or median and interquartile range, and categorical variables were summarized as frequency and percentage. Univariate analyses were performed to identify factors predictive of SFJR at each time point. Comparisons between the subgroup of patients with peripheral SpA and the subgroup of patients with axial or mixed SpA were also performed. The analysis was conducted based on the intention-to-treat principle. All statistical analyses were performed using SPSS v. 28.0 for Macintosh (SPSS Inc., Chicago, IL, USA).
Results
Patients
From March 2022 to March 2023, a total of 44 patients met the inclusion criteria and were enrolled in the study. Baseline characteristics are presented in Table 1. Active axial SpA was reported in 4 patients (9.1%), active peripheral SpA in 31 patients (70.5%), and mixed SpA in 9 patients (20.5%). At baseline, the mean ASDAS-CRP was 2.4 ± 0.7, and the DAS28-CRP was 3.5 ± 0.6. Notably, all but two patients were biologic-experienced, with more than half having undergone two or three previous biologic treatments. In addition, 38.6% of patients were receiving systemic steroids at baseline. Based on the partial Mayo score, 16 patients (36.4%) had mild disease activity, 26 patients (59.1%) had moderate activity, and 2 patients (4.6%) had severe luminal disease at baseline.
Patients’ characteristics at baseline.
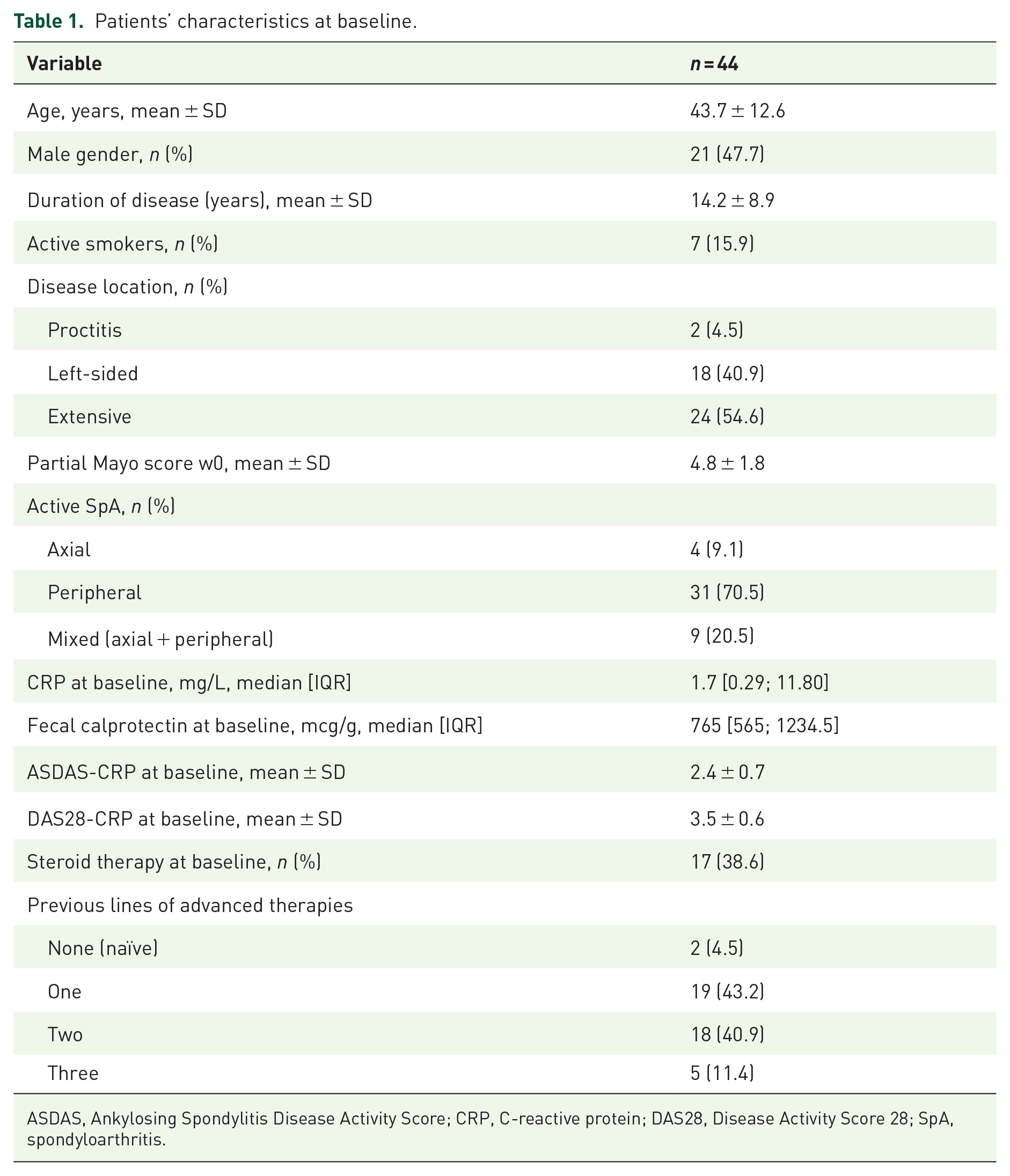
ASDAS, Ankylosing Spondylitis Disease Activity Score; CRP, C-reactive protein; DAS28, Disease Activity Score 28; SpA, spondyloarthritis.
Primary endpoint: SFJR
At 8 weeks, SFJR was reported in 52.3% of patients, with a significant difference between patients with peripheral SpA compared with the subgroup of patients with axial and mixed SpA (67.7% vs 15.4%; p = 0.001; Figure 2). Patients with CR had a higher rate of SFJR compared with those who did not achieve CR at 8 weeks (65.4% vs 33.3%; p = 0.04). At 52 weeks, SFJR was reported in 59.1% of patients (peripheral SpA: 71.0% vs axial and mixed SpA: 30.8%; p = 0.01; Figure 2). Again, patients with CR had a higher rate of SFJR compared with those who did not achieve CR at 52 weeks (74.2% vs 23.1%; p = 0.002). The univariate analysis of factors associated with SFJR at weeks 8 and 52 is reported in Table 2. Mean values of ASDAS and DAS-28 CRP overall decreased from baseline to week 8 and then to week 52 (Figure 3).

SFJR rates at weeks 8 and 52 in patients with UC-associated SpA treated with tofacitinib. Bars represent the percentage of patients achieving SFJR.
Variables associated with SFJR at week 8 and at week 52.

ASDAS, Ankylosing Spondylitis Disease Activity Score; CRP, C-reactive protein; DAS28, Disease Activity Score 28; SFJR, steroid-free joint response; SpA, spondyloarthritis; UC, ulcerative colitis.
Values are bold beacuse they are statistically significant (p < 0.05)
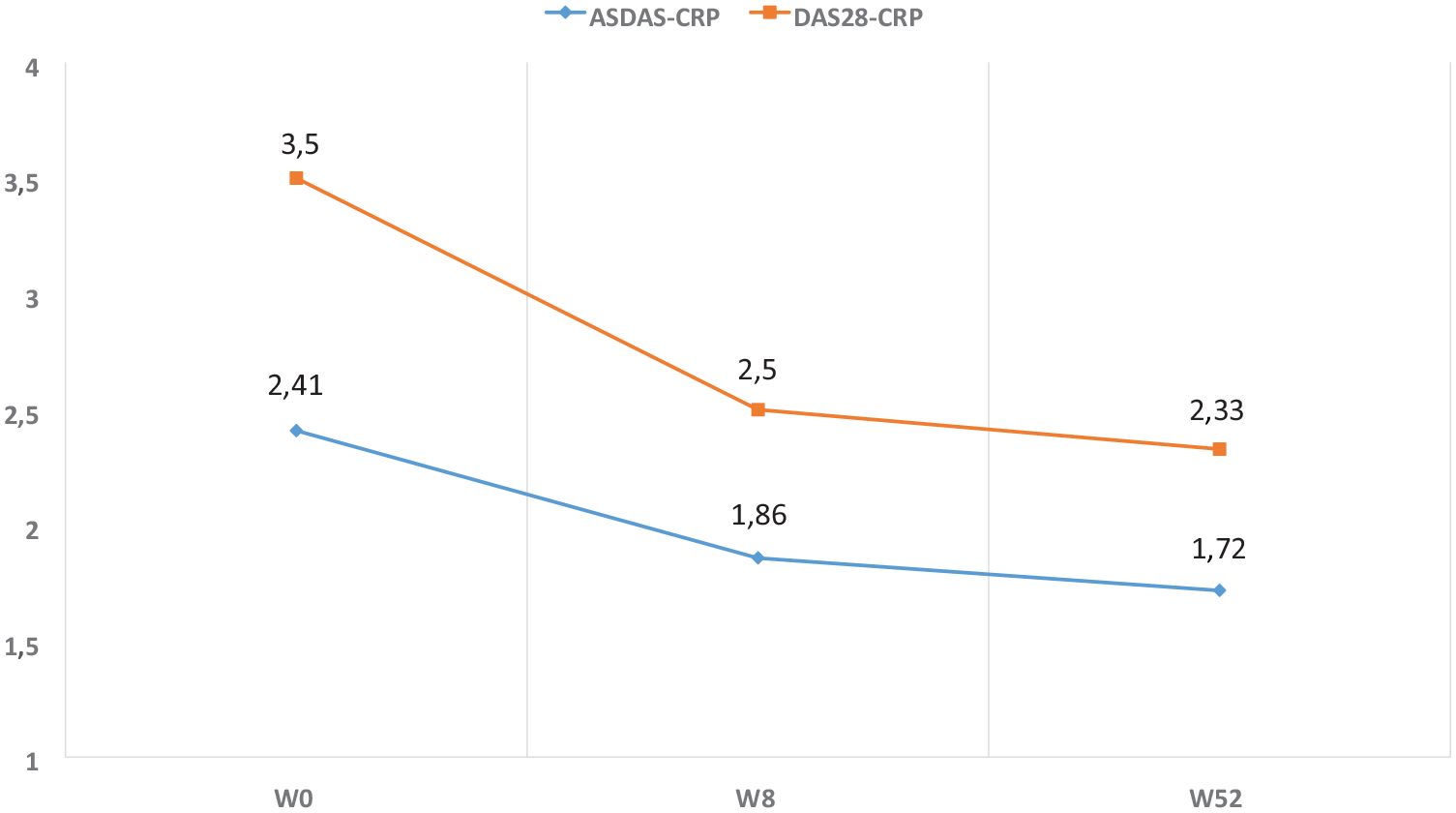
Mean values of ASDAS-CRP and DAS28-CRP at baseline, week 8, and week 52 in patients with UC-associated SpA treated with tofacitinib. Values represent disease activity scores for axial and peripheral SpA, respectively.
Secondary endpoints: CR and SFCR
CR was reported in 59.1% of patients at 8 weeks, and in 70.5% of patients at 52 weeks, with SFCR achieved by 34.1% at 8 weeks, and 45.5% at 52 weeks. At 8 weeks, CR was associated with being an active smoker (p = 0.02). Three adverse events were reported: one case of mild hypercholesterolemia, one case of mild elevation of transaminase levels, and one case of fever and malaise, which led to the withdrawal of TOFA after 3 days of administration. By the end of follow-up, 10 patients discontinued the treatment: 9 due to lack of efficacy and 1 due to the aforementioned adverse event. In addition, an extended induction period (TOFA 10 mg BID for 16 weeks) was required in 5 patients, while 6 patients underwent dose intensification during maintenance therapy (increasing from 5 mg to 10 mg BID).
Discussion
The pathogenesis of IBD-associated SpA involves a combination of genetic, immune, and environmental factors. 10 However, the exact mechanisms driving its development in IBD patients remain unclear. One hypothesis suggests that shared epitopes between the gut and joints may contribute to disease onset. 31
In patients with UC, TNF inhibitors have proven effective in managing extraintestinal manifestations involving the musculoskeletal system, skin, and eyes. 32 Nevertheless, about one-third of UC patients experience primary nonresponse to TNF inhibitors, and 23%–46% of responders eventually lose efficacy over time. 33
TOFA is a JAK inhibitor that has shown efficacy in several rheumatologic diseases as well as in UC. It primarily inhibits JAK1 and JAK3, with less activity against JAK2, modulating the signal transduction of multiple inflammatory cytokines. 7 Given the central role of the JAK-STAT pathway in inflammatory joint diseases, 34 the rationale for TOFA’s use in SpA is well supported.
When IBD and SpA coexist, therapeutic strategies must consider both intestinal and musculoskeletal symptoms. An evidence-based, personalized approach is essential, requiring close collaboration between rheumatologists and gastroenterologists to ensure optimal care. 15 Despite this need, most guidelines and position papers focus primarily on intestinal outcomes, reflecting the endpoints typically assessed in IBD clinical trials. As a result, current evidence on IBD-associated SpA is largely extrapolated from studies conducted in rheumatologic settings.
Our study is the first prospective investigation specifically designed to assess IBD-associated SpA using validated rheumatologic scores. The cohort included primarily difficult-to-treat patients, most of whom had undergone multiple prior biologic therapies. Overall, our findings suggest that TOFA is effective in treating UC-associated peripheral SpA. In contrast, the benefit for axial SpA was less evident. Due to the small number of patients with axial or mixed SpA, definitive conclusions are limited. However, our results align with previously reported response rates in non-IBD axial SpA.35,36
Moreover, our data are consistent with and build upon findings from a recent Spanish multicenter study, which reported joint symptom improvement or remission in patients with UC and SpA treated with TOFA. 23 That study, however, did not use standardized outcome measures for joint disease, relying mainly on physician- or patient-reported improvement. This limits interpretability. In contrast, our study applied validated indices (ASDAS-CRP and DAS28-CRP) to assess articular response and distinguish between steroid-dependent and steroid-free clinical benefit. This approach adds robustness and clinical relevance to our findings and supports the possibility that TOFA may induce true remission in a subset of patients with UC-associated SpA.
Importantly, we observed a differential response based on SpA phenotype. Patients with peripheral SpA had significantly higher rates of SFJR compared to those with axial or mixed disease. These differences may reflect distinct pathogenic mechanisms. Peripheral SpA appears more influenced by type 3 immunity and cytokines, such as IL-23 and IL-17, which may respond better to JAK inhibition. Axial SpA, on the other hand, may involve a different immune profile and be less dependent on JAK-STAT signaling.
A key strength of our study is its prospective design, which specifically focused on joint response. The use of rheumatologic scores—easily calculable using online tools—allowed for objective evaluation. Furthermore, the robustness of our findings is supported by the fact that most patients had previously failed multiple biologic therapies.
We acknowledge that the main limitation is the small sample size, particularly regarding patients with axial or mixed SpA. Although lower joint response rates were observed in this subgroup, the small numbers prevent firm conclusions. This limitation is related to the study’s strict inclusion criteria, which required active SpA at baseline rather than a historical diagnosis. Endoscopic data would have strengthened the connection between gut and joint inflammation. Unfortunately, endoscopy was not part of the study protocol. This omission is particularly relevant in UC, where mucosal healing may influence systemic immune pathways involved in extraintestinal manifestations. This highlights the need for future prospective studies integrating endoscopy, histology, and inflammatory biomarkers to better understand the gut-joint axis in UC-associated SpA.
We used DAS28-CRP to assess peripheral SpA, despite it being designed for rheumatoid arthritis. While rheumatoid arthritis and peripheral SpA are distinct, no gold standard exists for IBD-associated peripheral SpA. Another limitation is the non-mandatory presence of a rheumatologist. At the time of study design, this choice was made to encourage broader participation. However, most participating centers are tertiary referral hospitals with shared gastro–rheumatology clinics, so it is likely that patients were assessed by both specialists. In addition, the rheumatologic scores used are relatively simple to apply.
Conclusion
This is the first prospective study specifically designed to assess IBD-associated SpA. In patients with UC and multiple prior therapeutic exposures, TOFA was effective for peripheral SpA. Additional studies are needed to better evaluate its role in axial SpA.
Supplemental Material
sj-doc-1-tag-10.1177_17562848251367559 – Supplemental material for Real-world Effectiveness of Tofacitinib on Ulcerative Colitis-Associated Spondyloarthropathy: a multicenter prospective study from the Italian Group for the Study of Inflammatory Bowel Diseases (IG-IBD)
Supplemental material, sj-doc-1-tag-10.1177_17562848251367559 for Real-world Effectiveness of Tofacitinib on Ulcerative Colitis-Associated Spondyloarthropathy: a multicenter prospective study from the Italian Group for the Study of Inflammatory Bowel Diseases (IG-IBD) by Fabio Salvatore Macaluso, Mauro Grova, Fabrizio Bossa, Sonia Carparelli, Daniela Pugliese, Giuseppe Cuccia, Maria Cappello, Stefano Muscarella, Simone Saibeni, Cristina Bezzio, Alessandro Armuzzi, Antonietta Gerarda Gravina, Raffaele Pellegrino, Flavio Andrea Caprioli, Andrea Sorge, Alessandra Soriano, Davide Giuseppe Ribaldone, Stefano Festa, Angela Variola, Concetta Ferracane, Sara Onali, Massimo Claudio Fantini and Ambrogio Orlando in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.