
Abstract
Introduction:
The patient–physician relationship is important in implementing appropriate management strategies. The Ulcerative Colitis (UC) Narrative Global Surveys examined patient and physician views on multiple aspects of living with UC. However, there are many other important undiscovered aspects of UC to consider for patients in Japan.
Aim:
The aim of these ad hoc analyses was to identify detailed practical issues for further optimal care.
Methods:
Patient and physician questionnaires covered broad aspects of living with UC and practical care. Results were compared to identify gaps. We conducted multifaceted ad hoc analyses on the responses from Japan.
Results:
In Japan, 210 patients with UC and 151 physicians were surveyed. Most (64%) patients felt they would be more successful if they did not have UC. Physicians were more likely to discuss treatment-related topics, including side effects as a proxy for medication satisfaction, than quality of life-related topics. Physicians underestimated the importance to patients of toileting accidents (28% vs 54%) and overestimated the importance of mucosal healing (59% vs 29%). Although 72% of patients felt comfortable raising concerns with their physician, 53% worried about asking too many questions, as they thought they would be seen as a difficult patient, and 66% wished they had talked more about medication fears. The majority (83%) of patients said they were honest with their physician when discussing their experiences with UC, although 45% regretted not telling them more. Some (26%) patients believed, and some (20%) were not sure, that if their symptoms were under control then their UC was not active. More positively, 65% of patients agreed that UC had made them more appreciative of the important things in life.
Conclusion:
This survey revealed notable gaps between patients’ and physicians’ perspectives. Consequently, the importance of patient–physician communication remains constant, even in the era of biologics and treat-to-target strategies.
Plain Language Summary
It is important to discover the different ways that ulcerative colitis (UC) can impact individual patients, and to identify differences in views between people with UC and the doctors treating them, to improve patient care. The UC Narrative is a global survey (containing two questionnaires, one for patients, and one for doctors) that gathers information on how UC impacts patients. The survey aims to identify differences between patients’ and doctors’ views on communication and disease management.
In this analysis, we report the results from 210 patients with UC and 151 doctors who completed the UC Narrative survey in Japan, between November 2017 and January 2018. Most patients (85%) were satisfied with their communication with their doctor. However, doctors underestimated patient satisfaction, as they believed that about 71% of their patients were satisfied with communication. Around two-thirds of patients (65%), and most doctors (82%), wanted more discussion about goals for managing or treating UC. Most patients (83%) said they were honest with their doctor when discussing their experiences with UC, although almost half of patients (45%) said they regretted not telling their doctor more. Three-quarters of doctors (75%) felt that their patients were honest with them. Doctors underestimated the importance of toileting accidents to patients and thought that healing the patients’ intestine would be more important to the patients than toileting accidents. Some patients had misconceptions about treatment. For example, only 69% of patients knew that it was not OK to stop taking their UC medications once they felt better. This survey shows that even though treatment options for UC have developed, sufficient communication between patients and doctors is very important for overall patient care.
Introduction
Ulcerative colitis (UC) is an idiopathic, chronic inflammatory bowel disease (IBD) that affects the mucosa of the colon and rectum.1,2 UC is most common in adults 30–40 years of age, and symptoms can include rectal bleeding, abdominal pain, fecal urgency, and fatigue. 1 The morbidity associated with UC can have a significant effect on quality of life (QoL), 3 and UC has been shown to heavily impact patients’ social, professional, and family interactions. 4
High annual incidence and prevalence of UC has been reported in Europe (incidence up to 57.9 per 100,000 person-years; prevalence up to 505.0 per 100,000 population) and North America (incidence up to 23.1 per 100,000 person-years; prevalence up to 286.3 per 100,000 population), based on a systematic review of the literature up to December 2016. 5 Although traditionally viewed as a Western disease, global patterns in the incidence and prevalence of UC have undergone changes in recent decades,5–7 and studies have shown that the incidence of UC is increasing in many Asian countries.8–10 In Japan, an almost 10-fold increase in the prevalence of UC has been observed, rising from 18.1 per 100,000 population in 1991 11 to 172.9 per 100,000 population in 2014. 12 This rise in the prevalence of UC highlights a need for Asian countries to implement strategies to improve care and meet patient expectations on the management of UC.
Due to the chronic nature of UC and the significant impact of the disease on QoL,3,4,13 the relationship between a patient and their physician is important in understanding and implementing appropriate management strategies.14–16 Improving the patient–physician relationship can lead to greater adherence to therapy, foster a shared decision-making environment, and improve outcomes.17,18
The UC Narrative is a collaborative, global initiative, which examined perspectives on multiple aspects of UC through two related surveys: one patient-based and one physician-based. Global findings from the UC Narrative have been summarized, including the communication gaps and agreement between patients and physicians, 19 as well as the impact of living with UC. 20 Here, we present survey responses, including information not captured by the global surveys, from patients and physicians in Japan, using multiple questions that explored aspects of living with UC, including day-to-day disease impact, disease management, goal setting, and communication. Unlike previous surveys exploring disease impact or shared decision-making,21–24 the UC Narrative used mirrored surveys to compare the perspectives of both patients and physicians across a broad spectrum of issues and opinions relating to the daily clinical management of UC and the impact it has on patients’ lives.
The aim of the current ad hoc analyses of the UC Narrative Survey was to reveal practical issues that could be addressed by detailed analyses of the responses from Japan, for further optimal care. Identifying these areas of unmet need could lead to improvement in care for patients.
Materials and methods
Study design and populations
The UC Narrative is a collaborative, global initiative, sponsored by Pfizer Inc, under the direction of an advisory panel comprised of adults living with UC, gastroenterologists, IBD nurses, a psychologist, and representatives of IBD patient advocacy organizations from 10 countries: Australia, Canada, Finland, France, Germany, Italy, Japan, Spain, the United Kingdom, and the United States. The goal of the UC Narrative was to improve outcomes for patients living with UC internationally, by identifying common and country-specific barriers to better care, and proposing solutions to overcome these barriers. This has been achieved through two related global surveys (one patient-based and one physician-based). Full details of the survey methodology, including participant recruitment, eligibility criteria, and survey questions, have been reported previously,19,20 and are briefly described below.
The surveys were designed to assess multiple aspects of UC and its management, in addition to standard demographic information. To ensure the swift recruitment of a sufficient number of participants for all the countries included in the UC Narrative study, participating physicians were not treating the patients who participated in the study. The questions that were used in the survey were carefully predefined to identify several aspects of the gaps between the patients’ and physicians’ perspectives.19,20 The physician questionnaire mirrored the patient questionnaire to cover the same issues and allow for comparison with one another, where applicable. In the UC Narrative from Japan, patients answered around 60 questions and physicians answered around 40 questions. The number of questions answered could vary for patients and physicians, based on their responses throughout the surveys. The Japanese versions of the surveys are provided in the Supplemental Material. After publishing global data,19,20 we planned original detailed analyses to exhibit unreported practical issues for further optimal care. To perform multifaceted and non-prescriptive analyses, we used responses from Japan. Previous studies have presented data that compared results among different countries; however, because the social and medical environment in each country may have influenced the results, we performed several ad hoc original analyses that included previously unreported data from Japan.Patient- and physician-based surveys were conducted between November 2017 and January 2018 by the Harris Poll (a global consulting and market research company). Physicians were recruited online from a database collated through various channels (traditional market research methods and online recruitment (medical websites, online medical newsletters, or other online medical channels)). The research partner for physicians in Japan was Medefield (a global company specializing in online fieldwork services). Respondents were verified as practicing physicians using both automated and manual methods. Respondents who had opted into the research panel received an email invite with a link to the survey. In Japan, qualifying physician specialties included gastroenterology internist, gastroenterology surgeon, and internist with a gastroenterology focus, as part of the real-world data. To meet inclusion criteria, physicians were required to see ⩾5 patients with UC per month, and at least 10% of their current patients had to be taking a biologic for their UC. The government in Japan provides a special financial support system to treat patients with IBD. Physicians were asked to base their survey responses on their experiences of treating patients for whom they considered the severity (not determined by disease activity) of their UC to be classed as moderate to severe (defined as those who had ever taken more prescription medications than just 5-aminosalicylates for their UC to demonstrate the severity of clinical course; survey responses for other prescription medications included ‘corticosteroid’, ‘anti-tumor necrosis factor biologic’, ‘immunosuppressant’, and ‘another prescription medication for UC’). Patients were recruited from databases (held by the Harris Poll and partners) of individuals who agreed to participate in market research studies after being recruited online (e.g. social media, targeted banner advertising).
Eligible, consenting adult (⩾18 years of age) patients with UC who resided in Japan and self-reported that they had received an endoscopy-confirmed diagnosis of UC, had not had a colectomy, had visited a gastroenterologist or internist in the past year, and had ever taken prescription medications for their UC were included (see the Supplemental Material). A flare was defined as a period with a dramatic increase in symptoms of bloody diarrhea or stool frequency compared with those ordinary symptoms experienced in remission. Self-reported treatment history was used as a proxy for disease severity (see the Supplemental Material). Over 80% of patient respondents to the survey had to have UC with the severity classed as moderate to severe, as these patients had experienced a greater number of the obstacles faced by someone living with UC and were therefore more likely to be in need of the support and resources that the survey could help better identify. This approach helped to identify the widest range of challenges faced by patients with UC. Having a better understanding of this population, and the strategies that help them overcome disease management barriers, allows those learnings, tools, and resources to ultimately be of benefit to the entire UC population. As the UC Narrative was set up to understand all patients with UC, the survey also included a minority of patients with mild UC, capped at 20% of total survey respondents, for comparison with patients with moderate to severe UC. We performed the present investigation in accordance with the Consensus-Based Checklist for Reporting of Survey Studies (CROSS) guidelines.
Analyses of patient and physician surveys
Patient and physician survey responses were analyzed, as previously described by Rubin et al. (see the Supplemental Material). 19 Briefly, questions on both the patient and physician questionnaires required respondents to provide a numeric response using a Likert-type scale, to select a single option or multiple options from a list, or to indicate their level of agreement with a statement (from ‘strongly disagree’ to ‘strongly agree’). Any respondents who did not complete the full survey were excluded from the analysis. Descriptive statistics were used to assess patient and physician responses. Inferential statistics, including hypothesis testing, were not analyzed, because the UC Narrative is a fact-finding survey.
Ethical considerations
All respondents provided their consent before completing the questionnaire and were remunerated by the sponsor, on behalf of the investigators, for their participation in the survey. The surveys were not intended to provide clinical data for treatment decisions, and were not conducted as a clinical trial for any endpoints; ethics approval was therefore not required.
Results
Survey respondents
A total of 210 patients with UC completed the patient survey in Japan. Details of patient characteristics (per patient responses to survey questions) are provided in Supplemental Table S1. The mean age of patients with UC was 44.3 (standard deviation (SD), 11.6; median, 44) years, 73% were male, and 76% were employed. The length of time between first symptoms and diagnosis was <1, 1, or 2 years in 79%, 11%, and 4% of patients, respectively; a small proportion (6%) of patients reported the length of time between first symptoms and diagnosis to be ⩾5 years. The severity of UC in most (84%) patients was moderate to severe. Patients reported a mean of 2.5 (SD, 4.1) separate flares in the past 12 months. Overall, 65% of patients felt they spent more time in the bathroom than anywhere else. Patients reported a mean of 3.3 (SD, 3.0) visits to the bathroom (to pass stool, air, blood, or mucus) on their best day; on their worst day, this rose to a mean of 9.6 (SD, 6.0) visits.
Most (75%) patients considered themselves to be in remission for disease activity (severity not determined clinically) (Supplemental Table S1), defined as controlled with few to no symptoms; in contrast, physicians only thought that a mean of 47.8% (SD, 24.8) of their patients were in remission. Patients who self-described remission for their disease activity (defined as the patient’s disease is controlled with few to no symptoms) still experienced disease symptoms and impacts upon their QoL (Supplemental Table S1).
In Japan, a total of 151 physicians completed the physician survey. Details of physician characteristics (per physician responses to survey questions) are provided in Supplemental Table S2. The mean age of physicians was 42.8 (SD, 9.7) years, physicians had been in their specialty practice for a mean of 16.3 (SD, 8.1) years, and 94% were male. Over half (55%) of physicians practiced in an IBD center/clinic. Overall, 51% of medical practices had a specialist IBD nurse; only 23% of patients thought their physician’s practice had a specialist IBD nurse. Interestingly, of those physicians who said they worked at an IBD center/clinic, 78% said their medical practice had an IBD nurse, compared with only 18% of physicians who did not work at an IBD center/clinic. At the time of the survey, nearly all (99%) of the physicians surveyed had personally initiated a biologic treatment in their patients with UC.
Patient perceptions on the impact UC has on their lives
Patients gave their views on the impact UC has on their lives (shown in Figure 1). The majority (82%) of patients reported that their UC was mentally exhausting, and most (64%) felt they would be more successful if they did not have UC (shown in Figure 1a). Around two-thirds of patients felt it was possible for a UC medication to give them back their old life (67%), or that UC had made them more appreciative of the important things in life (65%). Patients reported experiencing several different emotions during a UC flare, most commonly fatigue and restlessness, which were reported by 56% and 51% of patients, respectively (shown in Figure 1b). Nearly, a third (32%) of patients reported family impacts as a result of their UC; the most common responses were ‘postponed having children’ (14%) and ‘deciding not to have any/more children’ (11%) (shown in Figure 1c). The majority (78%) of patients reported work impacts as a result of their UC; the most common reasons were taking time off work due to treatment (40%) or their disease/symptoms (37%) (shown in Figure 1d). The difference between the male and female perception of the impact UC has on their lives is shown in Supplemental Figure S1. Of note, a higher proportion of male vs female patients found their UC mentally exhausting (84% vs 75%), felt they would be more successful if they did not have UC (67% vs 57%), and felt their UC made them more resilient (49% vs 38%). A lower proportion of male vs female patients had a family impact as a result of their UC (30% vs 38%), felt more fatigued during a flare (53% vs 63%) and changed job due to their UC (24% vs 38%). Patients also expressed their views on the impact of UC on their work (shown in Supplemental Figure S2). Nearly, half (45%) reported that they had not told their employer about their UC for fear of repercussions.
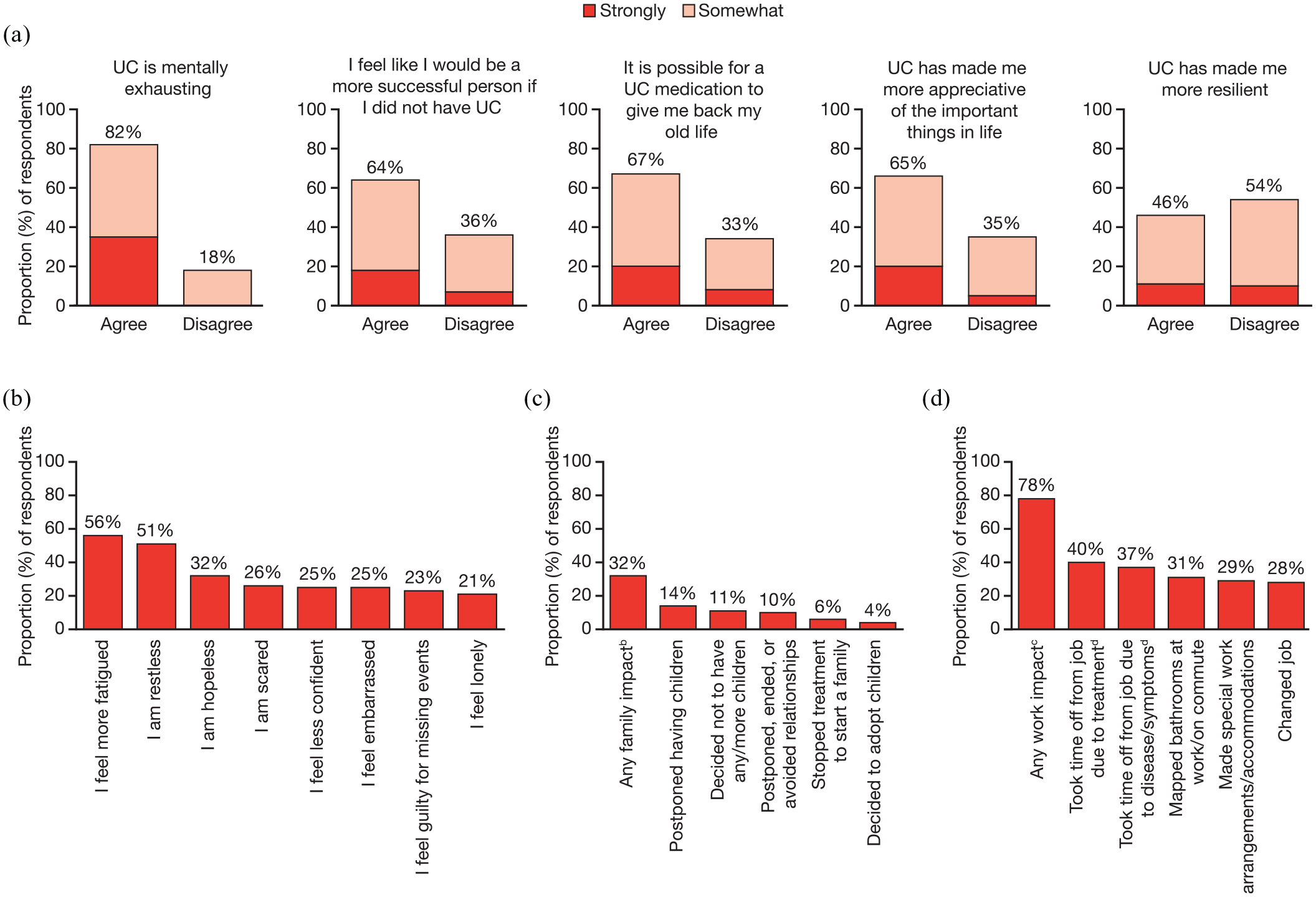
Patient perceptions on the impact of UC: (a) patient perceptions on the impact of UC, (b) emotions experienced during a UC flarea, (c) family impacts as a result of UCa, and (d) work impacts as a result of UCa.
Patient and physician alignment on topics relating to the management of UC during an outpatient visit in the exam room
Overall, around two-thirds (65%) of patients wished they had more time at appointments with their physician, and just over half (52%) of patients said their physician rarely had time to address all their questions and concerns. These concerns were more likely to be voiced by men than women (more time at appointments, 69% of men and 54% of women; rarely has time to address questions, 56% of men and 41% of women). The majority (79%) of physicians also wished they had more time at appointments.
Physicians’ views on their patients’ top priorities for UC management were slightly misaligned with patients’ views (shown in Figure 2a). Physicians underestimated the importance to patients of avoiding toileting accidents (28% vs 54%), reducing their risk of cancer (34% vs 49%), and reducing their fatigue (24% vs 41%), and they overestimated the importance of healing their mucosa (59% vs 29%) and avoiding hospitalization (56% vs 38%). However, physicians were generally aware of their patients’ top worries (shown in Figure 2b). Both patients (65%) and physicians (82%) wished for more discussion about goals for managing or treating UC (shown in Figure 2c). Although only 57% of patients (61% of men and 45% of women) wished for earlier/more discussion on treatment options, the majority (85%) of physicians felt this was important (shown in Figure 2d). When asked about treatment nonadherence, 55% (59% of men and 43% of women) of patients said they were hesitant to tell their physician if they do not take their medication exactly as prescribed (shown in Figure 2e); however, most (79%) physicians believed that over 50% of their patients did adhere to treatment, and a strong majority (94%) wished their patients would talk to them before stopping their medications (shown in Figure 2f).

Patient and physician alignment on what is important to patients when managing their UC: (a) top patient priorities for the management of UCa, (b) top patient worries due to UCb, (c) wished for more discussion about goals for managing/treating UCb, (d) wished for earlier/more discussion on treatment optionsd, (e) patient perceptions on nonadherence, and (f) physician perceptions on nonadherence.
Less than half of patients felt comfortable talking to their physician about their emotional concerns (48%) or their sex life and personal relationship concerns (40%; shown in Figure 3a, b). Physicians agreed that about half (54%) of their patients felt comfortable talking about their emotional concerns; however, they underestimated how many of their patients felt comfortable talking about their sex life and personal relationship concerns (19%; shown in Figure 3b). Although most (72%) patients said they felt comfortable raising concerns and fears with their physician (shown in Figure 3c), of those who were comfortable, 66% wished they had talked more about their fears of medical treatments, 53% worried that if they asked too many questions they would be seen as a difficult patient, and 51% said their physician rarely had time to address all of their concerns (shown in Figure 3d).

Patient and physician perceptions on discussions relating to personal topics: (a) patients are comfortable discussing emotional concerns with their physicians, (b) patients are comfortable discussing sex life and personal relationship concerns with their physicians, (c) patients—I feel comfortable raising concerns and fears with my physician, and (d) yet those who say they feel comfortable raising concerns and fears with their physician still say.
Patient–physician communication
The majority (85%) of patients were satisfied with the communication they have with their physician; physicians slightly underestimated patient satisfaction, believing that, on average, 71% of their patients were satisfied with their communication (shown in Figure 4a). Physicians also slightly underestimated patient satisfaction with UC medications; most (83%) patients were satisfied with their current medications, although physicians felt that only 67% of their patients were satisfied (shown in Figure 4b). However, physicians were more likely to overestimate patient desire for discussion about fears of medical treatments, with 84% of physicians desiring more discussion on this topic, compared with 59% of patients (shown in Figure 4c).
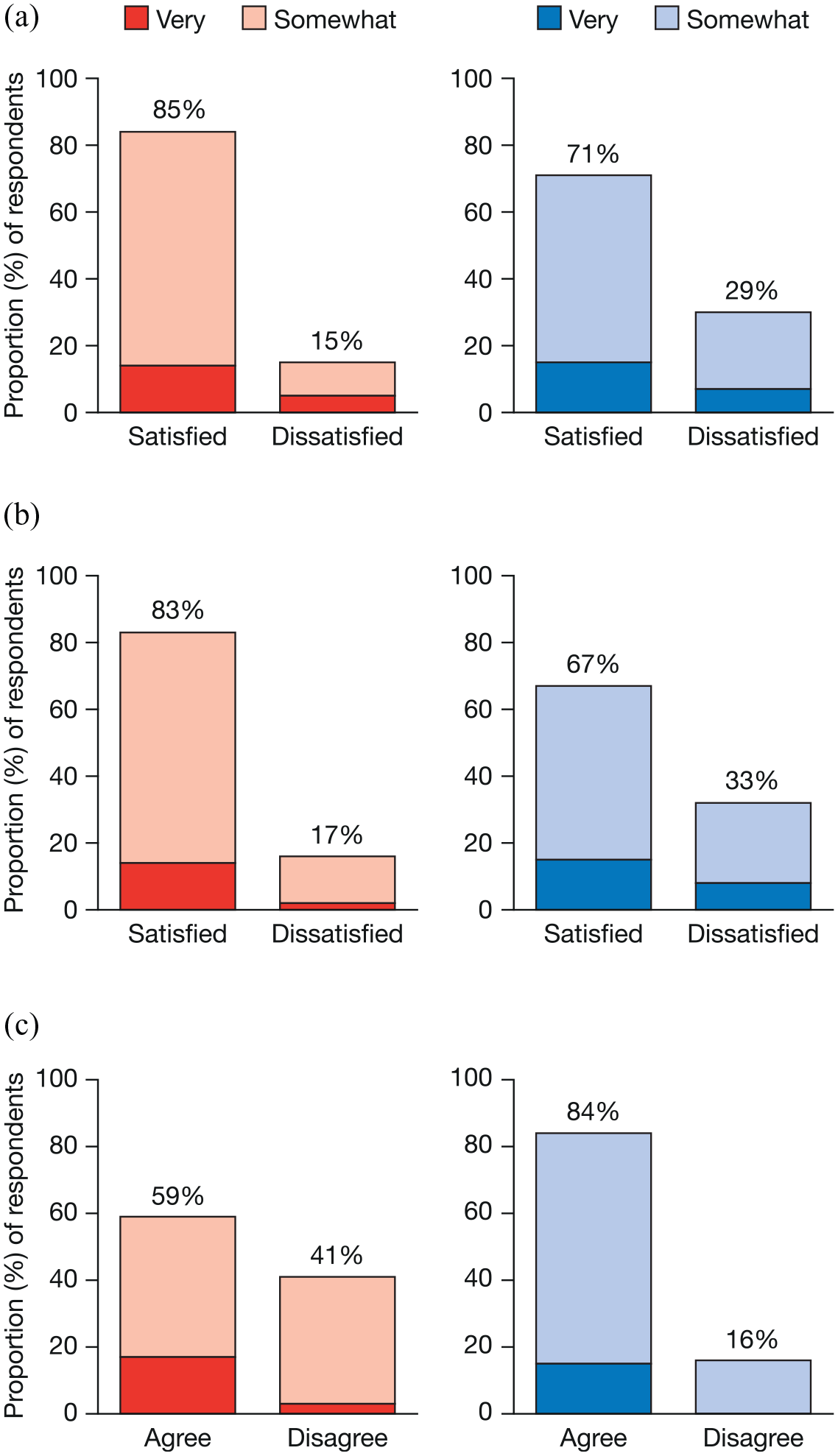
Satisfaction with patient–physician communication and UC medications: (a) mirrored perspectives with patient satisfaction with patient–physician communication (left), and physician perspective of patient satisfaction with patient–physician communication (right), (b) mirrored perspectives with patient satisfaction with current UC medication (left), and physician perspective of patient satisfaction with their current UC medication (right), (c) mirrored perspectives with patient desire to discuss more about their fears of medical treatment (left), and physician desire to discuss more about their patients’ fears of medical treatment (right). UC: ulcerative colitis.
Physicians were more likely to discuss treatment-related topics with their patients than QoL-related topics (shown in Supplemental Figure S3). Each topic in the discussion between patient and physician was classified as either of these according to the content of the discussion). Physicians use discussion about side effects as a proxy for the success of a medication regimen (shown in Supplemental Figure S4).
The majority (83%) of patients said they were honest with their physician when discussing their experiences with UC, although almost half (45%) said they regretted not telling their physician more; most (75%) physicians also felt that their patients were being honest with them (shown in Figure 5a). Survey responses indicate that physician time can be a barrier to communication, as around half (52%) of patients felt that their physician rarely had time to address all their questions and concerns, and two-thirds (68%) of physicians agreed (shown in Figure 5b).

Patient and physician views on patient honesty and addressing patient concerns: (a) patient and physician perceptions on patient honesty and (b) patient and physician perceptions on addressing concerns.
When asked about specific aspects of patient–physician communication, high proportions of patients reported that they were satisfied with the discussions they had with their physician (shown in Supplemental Figure S5). Despite high levels of patient satisfaction with patient–physician communication overall, patients identified several aspects of UC management that they felt their physician could explain better (shown in Supplemental Figure S6). Just over half of patients felt that their physician could better explain the hereditary nature of UC (52%) and how to access information and support from patient advocacy organizations (52%). Other aspects of UC management that patients felt their physician could better explain included the benefits and risks of biologics (40%), what will happen if their UC treatment fails (37%), and potential risk factors for cancer (30%). Patients also pointed to aspects of their experience of living with UC that they wished their physician understood better, with the most common aspects reported by patients being how much UC impacts their QoL (29%), how difficult it is for them to afford their medications (28%), how UC affects their mental health (27%), and how difficult it is for them to keep a job (25%) (shown in Supplemental Figure S7).
Patient misconceptions/knowledge gaps
Survey questions explored patients’ knowledge of UC (shown in Figure 6). Some patients had misconceptions about inflammation-specific facts of UC: 26% of patients believed that if their symptoms were under control then their disease was not active (a further 20% were not sure); 23% did not know it was important to keep their disease under control to reduce long-term complications; and 22% did not know that uncontrolled inflammation is a risk factor for colorectal cancer (shown in Figure 6a). Some patients had misconceptions about treatment: only 69% knew that it was not OK to stop taking UC medications once they felt better (shown in Figure 6b); only 76% knew that it was not OK to keep using steroids as a long-term maintenance medication (shown in Figure 6c); and only 60% knew that it was possible for their body to stop responding to biologics (shown in Figure 6d). Physicians recognized that some patients had knowledge gaps in these areas (shown in Figure 6b–d).
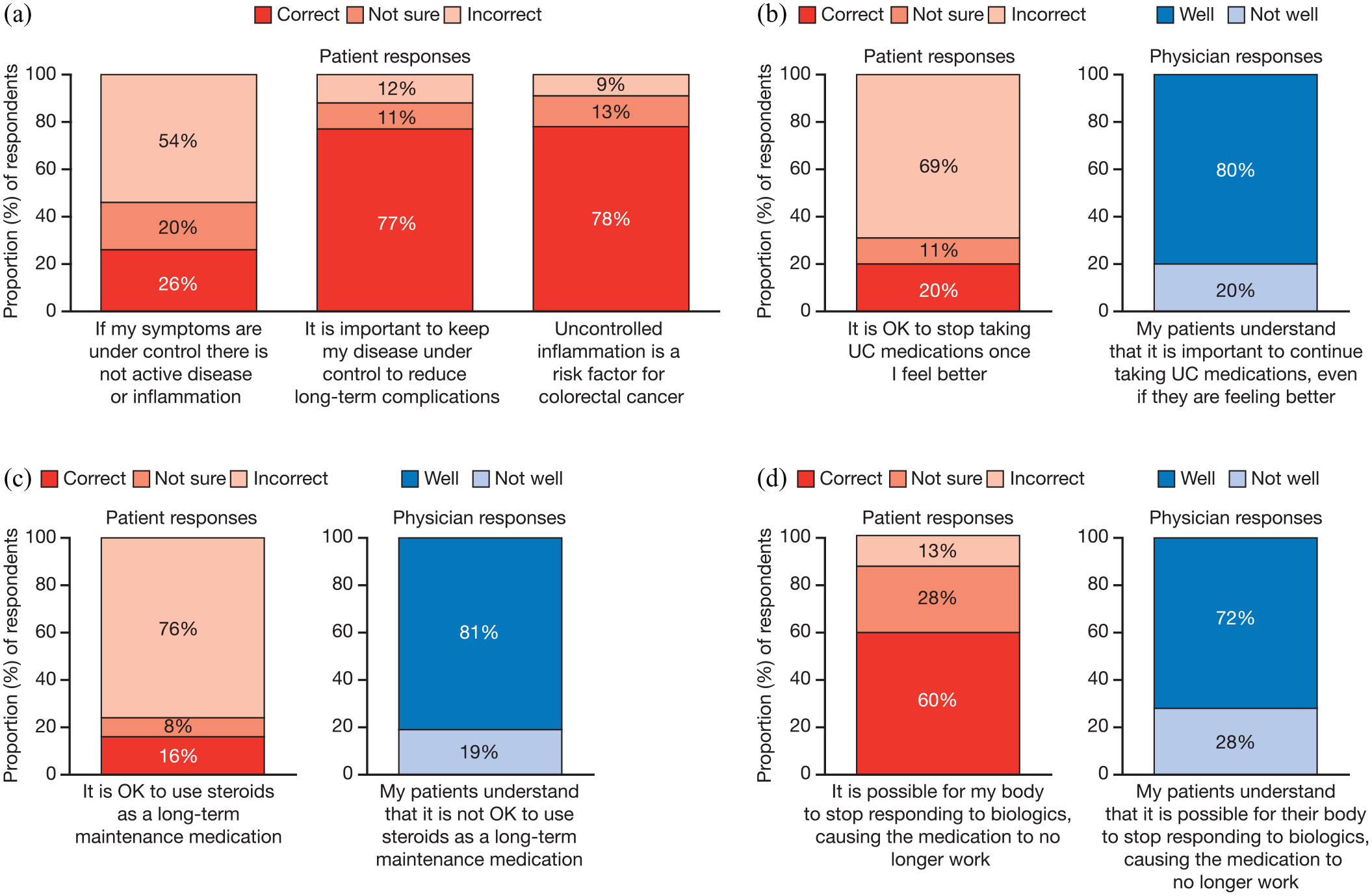
Understanding of symptoms, disease course, and treatment: (a) patient misconceptions pertaining to inflammation-specific facts of UC, (b) patient misconceptions about ceasing medication, (c) patient misconceptions about long-term steroid use, and (d) patient misconceptions about responding to biologics.
Information and support
Most (72%) patients wished they knew where to find information and support when they were first diagnosed with UC. Just over half (57%) of patients believed that patient advocacy organizations are important to the management of UC, a view more commonly shared by men (64%) than women (38%). Of those patients who had interacted with a patient advocacy organization, 78% wished they had known about them sooner (shown in Figure 7a). A higher proportion (71%) of physicians believed that patient advocacy organizations are important in the management of UC (shown in Figure 7b). However, physicians only recommended patient advocacy organizations as a source of information and support to a mean of 26% of patients (shown in Figure 7c).
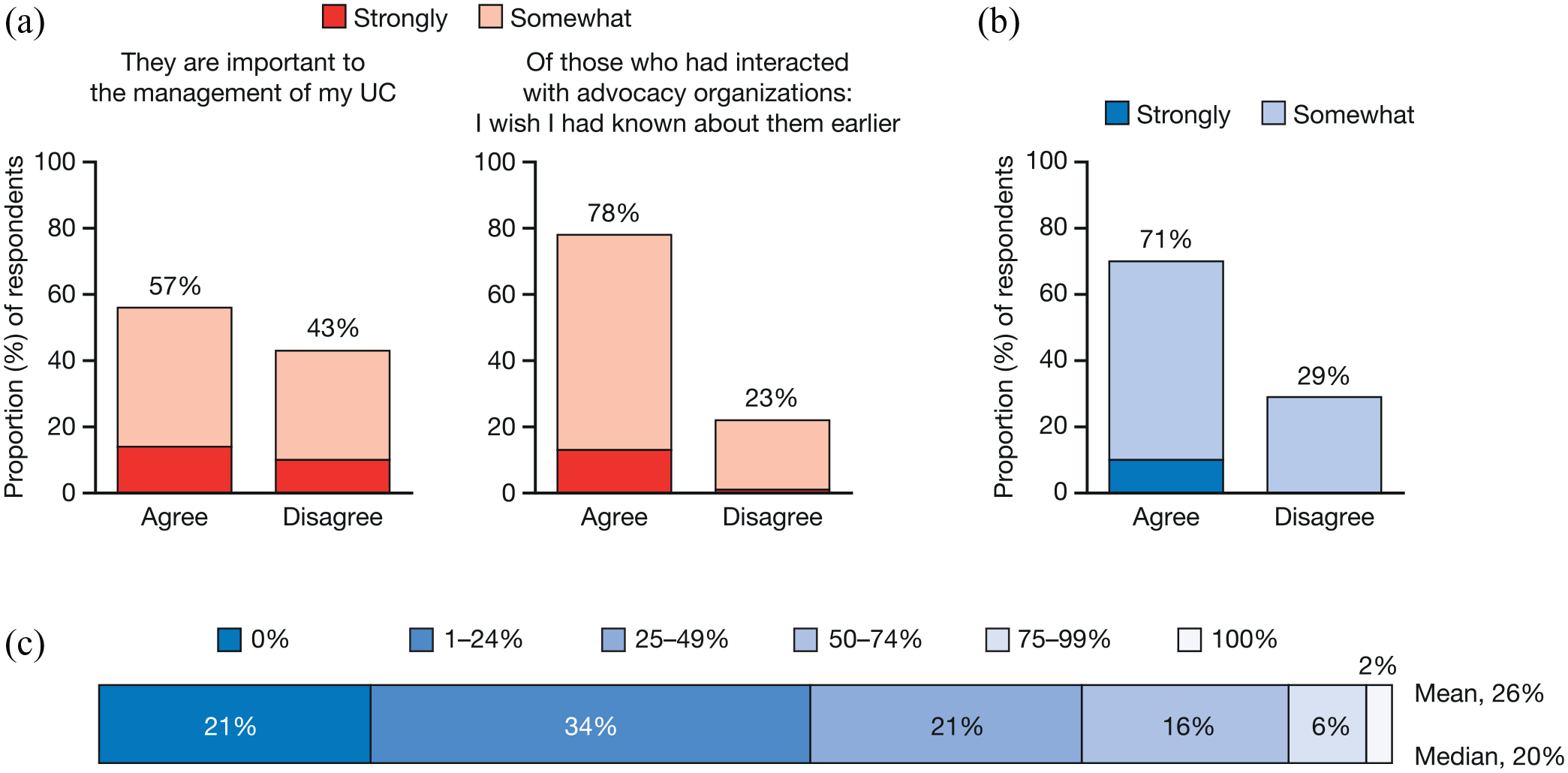
Patient and physician perceptions on patient advocacy organizations: (a) patient perceptions on patient advocacy organizations, (b) physician perceptions on the importance of patient advocacy organizations to the management of UC, and (c) proportion of patients that physicians recommend patient advocacy organizations to.
Just over a third (38%) of patients had interacted with a patient advocacy organization, although only 20% of patients said they were referred to one by their physician (Supplemental Table S3). A similar proportion of patients (21%) said they had relied on information from a patient advocacy organization or support group to help them make choices about treatment and UC management. Just under a third (31%) of patients said they had participated in a support group. When patients were asked what information they would be interested in receiving from a patient advocacy organization (Supplemental Material; shown in Supplemental Figure S8), the top responses were: how to live better with UC (50%); how to know if my medications are working (39%); and treatment options, including how medications work (34%).
When physicians were asked what resources could help improve relationships with their patients, the top three responses were: more information about UC in general to give to my patients (44%); the ability to refer my patients to chronic disease management classes (38%); and more information about the UC treatment options that are available to give to my patients (36%; shown in Supplemental Figure S9).
Discussion
Here, we present results from ad hoc analyses of the UC Narrative Survey from Japan to identify, in detail, practical issues that could be addressed to optimize care. The UC Narrative is a collaborative, global initiative, which examined perspectives on multiple aspects of UC through two related surveys: one patient-based and one physician-based. 19 While results from the Global UC Narrative Survey have been published previously,19,20 there remain many other undiscovered aspects of UC to consider for further optimal care, including day-to-day disease impact, disease management, goal setting, and patients’ and physicians’ communication, as explored here. The current survey revealed that most patients considered themselves in remission, despite impacts to their daily life (shown in Figure 2; Supplemental Table S1). Most patients were happy with the communication with their physician, but desired longer appointment times and earlier discussion about patient advocacy organizations (shown in Figures 2, 4, and 7).
Globally, most patients had moderate to severe UC (defined by self-reported treatment history), yet many described their UC as in remission (defined as controlled with few to no symptoms). 19 This was also true for the results reported here from Japan, although it is of note that, compared with the other eight countries in the global survey, a higher proportion of patients in Japan and Finland reported remission. 20 Despite reporting remission, patients still experienced disease symptoms and impacts upon their QoL, such as multiple visits to the bathroom to pass stool, air, blood, or mucus. Roughly half of physicians answered that their patients were in remission (Supplemental Table S1); however, physicians commented on their patients as a collective rather than on any specific patient.
Physicians were more likely to discuss treatment-related topics with their patients than QoL-related topics. In relation to treatment nonadherence, over half of patients said they were hesitant to tell their physician if they do not take their medication exactly as prescribed; however, most physicians believed that over 50% of their patients did adhere to treatment, and a strong majority wished their patients would talk to them before stopping their medications. Half of patients said their physician rarely had time to address all of their concerns, and over half worried that if they asked too many questions they would be seen as a difficult patient. Of those who were comfortable raising concerns and fears, two-thirds wished they had talked more about their fears of medical treatments.
This survey highlights the importance of regularly monitoring patients’ mental health, as most patients in Japan reported being mentally exhausted due to their UC (shown in Figure 1). Most patients felt they would be more successful if they did not have UC. Moreover, many patients reported that their UC had a negative impact on their confidence at work. Previously, a survey in Japan reported that patients missed work due to worrying about UC symptoms, rather than because of the symptoms themselves. 23 Nearly, half of patients reported that they had not told their employer about their UC for fear of repercussions. On a positive note, we also report that many patients believed that having UC made them more appreciative of the important things in life.
While adjustments of the treatment regimens according to the results of objective monitoring in the treat-to-target strategy have led to improvements in UC management, 15 the importance of patient–physician communication should not be neglected, as shared decision-making is a major driver of treatment satisfaction.7,25,26 Here, the length and focus of routine appointments was a concern raised by patients and physicians (shown in Figure 2). Many patients desired longer appointment times and felt their current appointment length was not sufficient to address all questions and/or concerns. Interestingly, these concerns were more likely to be voiced by men than women. Despite the desire for longer appointment times, there was a high level of patient satisfaction with patient–physician communication. Previously, the prevailing style of communication in Asia was paternalistic, 27 and patients seemed less likely to ask questions or voice concerns. 16 The data reported here suggest that patients and physicians recognize the importance of greater discussion of treatment goals.
Despite satisfaction with communication, there were some aspects highlighted by patients for improvement. Patients wished their physician better understood how much UC impacts upon various aspects of their life, a finding that aligned with previous studies that reported that healthcare professionals often underestimated the impact of UC symptoms on their patients (shown in Figure 2). 28 Around half of patients felt that their physician could better explain how to access information and support from patient advocacy organizations. Social support has been shown to positively correlate with health-related QoL in patients with IBD. 29 Of those patients who had interacted with a patient advocacy organization, most wished they had known about them sooner (shown in Figure 7). Unlike national patient advocacy organizations that exist in some Western countries, such as the US Crohn’s & Colitis Foundation, and Crohn’s and Colitis Canada, 30 most patient advocacy organizations in Japan are small and disjointed, limiting their influence on policy. 31
Physicians’ views on their patients’ top priorities for UC management were slightly misaligned with patients’ views. Physicians underestimated the importance of reducing cancer risk and fatigue for their patients, and placed more importance on healing mucosa than patients did (shown in Figure 2).
Although these findings provide important insight into the views of patients with UC and physicians who treat them, some limitations exist. As the survey was conducted online, a self-reported system that included treatment history was used as a proxy for disease severity in patients with UC. In addition, while approximately 20% of physicians in Japan are female, 32 only 12 (6%) of the participating physicians in this survey were female. Moreover, participating physicians were not the physicians of participating patients. In spite of these limitations, these ad hoc analyses exhibit some strengths, as they have revealed more practical issues for further optimal care, through multifaceted analyses using numerous question items.
In conclusion, there was a high level of concordance between patients and physicians in their responses; however, the survey revealed some gaps between patients’ and physicians’ perspectives. Most patients felt they would be more successful if they did not have UC. Physicians were more likely to discuss treatment-related topics than QoL-related topics, and they underestimated the importance to patients of toileting accidents and overestimated the importance of mucosal healing. Although most patients felt comfortable raising concerns with their physician, about half of patients worried about asking too many questions, and most patients wished they had talked more about medication fears. The majority of patients said they were honest with their physician when discussing their experiences with UC, although nearly half regretted not telling them more. More positively, most patients agreed that UC had made them more appreciative of the important things in life. This survey serves as a reminder of the importance of patient–physician communication, even in the era of biologics and treat-to-target strategies.
Supplemental Material
sj-docx-1-tag-10.1177_17562848221095372 – Supplemental material for Notable gaps between patients’ and physicians’ perspectives on communication and disease management in Japan: multifaceted ad hoc analyses of the global Ulcerative Colitis Narrative Survey for further optimal care
Supplemental material, sj-docx-1-tag-10.1177_17562848221095372 for Notable gaps between patients’ and physicians’ perspectives on communication and disease management in Japan: multifaceted ad hoc analyses of the global Ulcerative Colitis Narrative Survey for further optimal care by Kenji Watanabe, Sean Gardiner and Shoko Arai in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
The authors would like to thank The Harris Poll for their support of the study, and contribution to the study design and statistical analysis; the UC Narrative Survey Panel for their contribution to the study design; and GCI Health for their support of the study. The authors would also like to thank the patients and physicians who were involved in the UC Narrative Survey. The UC Narrative surveys were sponsored by Pfizer Inc. Medical writing support, under the guidance of the authors, was provided by Chris Guise, PhD, CMC Connect, McCann Health Medical Communications and was funded by Pfizer Inc, New York, NY, USA, in accordance with Good Publication Practice (GPP3) guidelines (Ann Intern Med. 2015; 163:461–64).
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The UC Narrative surveys were sponsored by Pfizer Inc. Medical writing support was funded by Pfizer Inc.
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KW has received research funding from Asahi Kasei Medical CO., Ltd, KYORIN Pharmaceutical Co., Ltd, Mitsubishi Tanabe Pharma, Mochida Pharmaceutical Co., Ltd, Otsuka Pharmaceutical Co., Ltd, and Zeria Pharmaceutical Co., Ltd; consultancy fees from AbbVie Japan, EA Pharma Co., Ltd, Janssen Pharmaceuticals, Inc, JIMRO Co., Ltd, Kissei Pharmaceutical Co., Ltd, KYORIN Pharmaceutical Co., Ltd, Mitsubishi Tanabe Pharma, Mochida Pharmaceutical Co., Ltd, Olympus Corporation, Pfizer Japan Inc, Takeda, and Zeria Pharmaceutical Co., Ltd; and lecture fees from AbbVie Japan, Astellas, Covidien Japan Inc, EA Pharma Co., Ltd, Janssen Pharmaceuticals, Inc, JIMRO Co., Ltd, Kissei Pharmaceutical Co., Ltd, KYORIN Pharmaceutical Co., Ltd, Mitsubishi Tanabe Pharma, Mochida Pharmaceutical Co., Ltd, Nippon Kayaku Co., Ltd, Olympus Corporation, Pfizer Japan Inc, and Zeria Pharmaceutical Co., Ltd. SG and SA are employees and shareholders of Pfizer Inc.
Data sharing statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.