
Abstract
Background:
Mucosal healing (MH) is considered the preferred therapeutic target for ulcerative colitis (UC). Impaired quality of life (QoL), irritable bowel syndrome (IBS)-like symptoms, and functional bowel symptoms have been reported in several inactive patients with UC. This study aims to assess the occurrence of functional bowel disorders (FBD)-like symptoms and QoL in UC patients with MH, and to explore the factors related to FBD-like symptoms.
Methods:
UC patients with MH (Mayo endoscopic score, MES = 0 or 1) were required to complete the Rome IV diagnostic questionnaire, the 32-item version of Inflammatory Bowel Disease Questionnaire (IBDQ-32), the 36-item short form healthy survey questionnaire (SF-36), and the Hospital Anxiety and Depression Scale (HADS). UC patients who did not achieve MH (MES > 1) completed the IBDQ-32, the SF-36, and the HADS. Community-dwelling healthy controls (HCs) completed the SF-36 and the HADS.
Results:
Among the 119 UC patients with MH recruited, 45.4% reported functional bowel symptoms; functional constipation-like symptom (13.4%) was the most prevalent, followed by IBS-like symptom (10.9%), and functional diarrhea-like symptom (10.0%). The IBDQ-32 and SF-36 scores were significantly lower in MH patients with FBD-like symptoms than in those without FBD-like symptoms. Disease duration [odds ratio (OR): 1.022; p < 0.001], body mass index (BMI; OR: 0.726; p < 0.001) were independent predictors of FBD-like symptoms in UC patients with MH. Combining these two factors could attain area under the curve [0.786; 95% confidence interval (CI): 0.701–0.856, p < 0.001] to predict FBD-like symptoms in MH patients.
Conclusion:
A number of UC patients with MH had accompanying FBD-like symptoms and significantly impaired QoL. Disease duration, BMI could predict the occurrence of FBD-like symptoms.
Keywords
Introduction
Ulcerative colitis (UC), a type of inflammatory bowel diseases (IBD), is characterized by mucosal inflammation in the rectum and colon that alternates between recurrence and remission, resulting in disability. Clinical symptoms may vary across bowel segments. The principal manifestation of proctitis is urgent and incomplete defecation. While paradoxical constipation is more commonly seen in some patients with left-sided colitis, bloody diarrhea and abdominal pain are more frequent symptoms of pancolitis. 1 The International Inflammatory Bowel Disease Research Organization (IOIBD) issued the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE)-II statement to update the therapeutic goals for patients with IBD. Long-term targets of STRIDE-II added restoration of quality of life (QoL), absence of disability, and normal growth in children based on STRIDE-I, which only put forward clinical remission and endoscopic healing. 2 Mucosal healing (MH), the absence of erosion and ulcers observed during endoscopy in patients with UC, is the preferred therapy target because inflammation is confined to the mucosa. Meanwhile, MH is considered a key research endpoint in UC. The definition of QoL is an individual evaluation of living that meets the individual’s expectations, standards, goals, and concerns based on social, cultural, and environmental context. 3 Casellas et al. 4 demonstrated that UC patients with MH normalized their QoL. However, in a periodic clinical review, several patients with UC who achieved MH often reported gastrointestinal (GI) discomfort and impaired QoL. The main GI complaints were abdominal pain, constipation, diarrhea, and abdominal bloating, similar to those reported for functional bowel disorders (FBDs). However, those GI complaints are not due to known inflammatory disease activity.
FBD is one of the functional GI disorders (FGIDs). 5 FGIDs are a series of chronic GI discomforts that lack structural abnormalities. FGID symptoms include abdominal pain, constipation, diarrhea, abdominal distension, heartburn, dysphagia, nausea, vomiting, belching, and anorectal pain. The criteria recommended by the Rome Foundation are the most frequently used criteria for the diagnosis and classification of FGID. According to the Rome IV criteria, FBD comprises IBS, functional constipation, functional diarrhea, functional abdominal bloating/distension, opioid-induced constipation, and unspecified FBD. According to the Rome II criteria, the prevalence of FBD in patients with inactive UC was 50% in Canada in 2005. 6 The prevalence of IBS-like symptoms in patients with inactive IBD was 9.1–37% under various Rome criteria.6–12 UC patients in remission with IBS-like symptoms had reduced well-being compared with those without IBS-like symptoms. 12 Owing to the similarity of some GI symptoms with FBD and UC, UC patients with MH accompanied by FBD-like symptoms may experience an increase in disease activity and severity, as well as QoL impairment.
The occurrence and related factors of FBD-like symptoms diagnosed using the Rome IV criteria in UC with MH have not been previously investigated. Therefore, this study aimed to assess the occurrence of FBD-like symptoms and patients’ QoL, and to explore factors related to functional bowel symptoms.
Materials and methods
Patient recruitment and eligibility
This observational, retrospective study was conducted at the IBD center of the First Affiliated Hospital of Sun Yat-sen University from 30 September 2019 to 30 January 2022. We consecutively recruited 246 UC patients aged 18 years old or older. A total of 214 community-dwelling healthy controls (HCs) were recruited. MH was commonly defined as having a Mayo endoscopic score (MES, see Supplementary Table 1) of 0 or 1, complete MH was defined as having an MES of 0. 2 UC patient with not mucosal healing (NMH) was defined as having an MES of 2 or 3. The definitive diagnoses of patients with UC were supported by clinical appearance, laboratory index, endoscopy, and histology results. 13 Patients with a history of surgery, coexisting complicated diseases (rheumatoid arthritis, systemic lupus erythematosus, and ankylosing spondylitis), and extraintestinal manifestations were excluded.
Clinical and demographic information of the patients were collected from their medical records. Patients with MH were asked to complete the Rome IV diagnostic questionnaire, the 32-item version of the Inflammatory Bowel Disease Questionnaire (IBDQ-32), the 36-item short form healthy survey questionnaire (SF-36), and the Hospital Anxiety and Depression Scale (HADS) during an outpatient colonoscopy consultation. Patients with NMH completed the IBDQ-32, the SF-36, and the HADS. Community-dwelling HCs completed the SF-36 and the HADS. The details of these questionnaires are shown below. Participants were divided according to their body mass index (BMI) as follows: underweight (BMI < 18.5 kg/m2), normal-weight (BMI 18.5–24.9 kg/m2), overweight (BMI 25–30 kg/m2), and obese (BMI ⩾ 30 kg/m2).
The reporting of this study conforms to the STROBE statement. 14 The study design was approved by the ethics committee of the First Affiliated Hospital of Sun Yat-sen University [No. (2021) 786]. All participants provided informed consent and we have de-identified all patient details.
Disease activity
Referring to the European consensus, 15 a modified Mayo scoring system was used to evaluate disease activity in patients with UC (Supplemental Table 1). Disease activity was categories such as remission, mildly active, moderately active, and severely active based on the modified Mayo scores of < 2, 3–5, 6–10, and 11–12, respectively.
FBD-like symptoms
The Rome IV diagnostic questionnaire16,17 for adults and the Rome committee consensus scoring approach were used to diagnose and classify functional GI and bowel symptoms in UC patients with MH. The broad categories include the esophagus, gastro-duodenum, bowel, GI pain, sphincter of Oddi, and anorectum. 5 A further division could be made for each broad category; for example, FBD into IBS, functional constipation, functional diarrhea, functional abdominal bloating/distension, opioid-induced constipation, and unspecified FBD. Organic diseases that could explain GI symptoms were excluded in light of the Rome IV criteria. Bowel symptoms of MH patients were not attributed to inflammatory activity.
Quality of life
The IBDQ-32 is a validated QoL tool in patients with IBD. 18 The IBDQ-32 measures bowel symptoms, systemic symptoms, emotional functions, and social functions, with scoring from 1(poor) to 7(best) for 32 items. Considering that the IBDQ-32 is a disease-specific questionnaire, the SF-36 questionnaire was used to evaluate QoL in HCs and patients with MH and NMH. The SF-36 can also be used to assess QoL in patients with UC. 19 The SF-36 comprises eight domains: physical function, role limitations physical health, role limitations emotional problems, energy, emotional well-being, social functioning, pain, and general health, with scoring from 0 (worst) to 100 (best) in each domain of the SF-36.
Anxiety and depression
The HADS is a measure used to evaluate anxiety and depression and assess the severity of symptoms in different populations. 20 Thus, the HADS can be used to determine whether patients with UC are in a state of anxiety or depression. 21 It had been revealed that HADS score was 76% sensitive and 79% specific for diagnosing anxiety or depression in IBD patients. 22 This questionnaire consists of items on anxiety and depression symptoms, with 14 items with scores ranging from 0 to 3. A total score of 0–10 and ⩾ 11 was defined as normal and anxiety or depression, respectively.
Statistical analysis
There are two ways to group UC patients: MH (MES = 0 or 1) versus NMH (MES = 2 or 3), and MES = 0 versus MES > 0. The occurrence and descriptive analysis of FBD-like symptoms were performed as numbers, frequencies, and 95% confidence intervals (95%CI). Continuous variables were reported as means and standard deviations (SDs) or median and interquartile ranges (IQRs). The normally distributed continuous variables were compared between two groups using the student t-test, while non-normally distributed variables were compared between two groups using Mann–Whitney U test. Categorical variables were compared using the Chi-squared test. Related factors were identified using a univariate logistic regression analysis model and a multivariable backward stepwise logistic regression analysis. A receiver operating characteristic (ROC) curve analysis was performed to identify predictors of FBD-like symptoms. All statistical analyses were conducted using the SPSS statistical software (version 25.0, IBM, Chicago, IL, USA). A two-sided p value <0.05 was supposed to be statistically significant.
Results
Participants’ characteristics
The characteristics of the participants are listed in Table 1 and Supplementary Table 2. A total of 119 UC patients with MH (response rate 96.0%) and 127 UC patients with NMH (response rate 97.7%). When it comes to MH defined having an MES = 0, a total of 54 UC patients having an MES = 0 score, and 192 UC patients having an MES > 0.
The median modified Mayo score and median disease duration were significantly lower in the MH group than in the NMH group. Based on a blood test that was conducted, median levels of C-reaction protein (CRP) and erythrocyte sedimentation rate (ESR) as well as mean white blood cell (WBC) counts were found to be significantly lower in the MH group than in the NMH group. Patient-reported symptoms were significantly improved in the MH group than in the NMH group. Median BMI was significantly higher in the HC group than in the MH and NMH group. The difference between the MES = 0 group and the MES > 0 group was similar to that between the MH group and the NMH group.
Characteristics of ulcerative colitis (UC) patients with mucosal healing (MH) and without mucosal healing (NMH) and healthy controls (HC).

ALB, albumin; 5-ASA, 5-amino salicylic acid; BMI, body mass index; CRP, C-reaction protein; ESR, erythrocyte sedimentation rate; HADS, Hospital Anxiety and Depression Scale; HB, hemoglobin; HC, healthy control; HCT, hematocrit; IQR, interquartile range; MH, mucosal healing; N, number; n, number; NA, not available; NMH, UC patients without mucosal healing; PLT, blood platelet; SD, standard deviation; UC, ulcerative colitis; WBC, white blood cells.
Scores of HADS anxiety and depression: Normal (0–10), abnormal (⩾ 11).
Occurrence of FBD-like symptoms
Table 2 shows the comparison of the occurrence of FBD-like symptoms in UC patients with MH. Among the 119 UC patients with MH, 54 patients (45.4%) met the Rome IV criteria for having FBD-like symptoms. The prevalence of FBD in the Chinese population was derived from a global survey conducted by the Rome Foundation using the Rome IV criteria. 23 Both age (p = 0.070) and gender (p = 0.193) showed no statistical difference between UC patients with MH and the Chinese population. The occurrence of many functional bowel symptoms was significantly higher in UC patients with MH than in the Chinese population.
The occurrence of functional bowel disorder-like symptoms in ulcerative colitis patients with mucosal healing.

CI, confidence interval; MH, mucosal healing; N, number; n, number; NA, not available; UC, ulcerative colitis.
The prevalence of FBD in the Chinese population was derived from a global survey conducted by the Rome Foundation using the Rome IV criteria. 23
Among the MH patients with FBD-like symptoms, 16 (29.6%) were compatible with other functional GI symptoms. Of this patients, 10 (18.5%) had functional constipation-like symptom, 4 (7.4%) had IBS-like symptom, and 2 (3.7%) had functional diarrhea-like symptom that overlapped with other functional GI symptoms. FBD-like symptoms mainly overlapped with functional anorectal symptoms (18.5%), functional gastroduodenal symptoms (5.6%) and functional esophageal symptoms (5.6%).
Among the 54 UC patients having an MES = 0, 26 patients (48.1%) met the Rome IV criteria for having FBD-like symptoms. The occurrence of many functional bowel symptoms was significantly higher in the MES = 0 group than in the Chinese population (Supplementary Table 3). Among the MES = 0 patients with FBD-like symptoms, eight (14.8%) were compatible with other functional GI symptoms.
Characteristics of MH patients with and without FBD-like symptoms
The characteristics of MH patients in UC with FBD-like symptoms (FBD-like +) and without FBD-like symptoms (FBD-like −) are shown in Table 3. Duration of the disease, the proportion of those who were underweight were significantly higher in the FBD-like + group than in the FBD-like − group. The proportion of those with normal-weight was significantly lower in the FBD-like + group than in FBD-like − group. The score of each IBDQ-32 domain was significantly lower in the FBD-like + group than in the FBD-like − group, while scores between the FBD-like + group and NMH group were not statistically different (Table 4). Scores for most of the SF-36 domains were significantly lower in the FBD-like + group than in FBD-like − group as well as in the HC group, while scores between the FBD-like + group and NMH group were not statistically different (Table 4). Supplementary Tables 4 and 5 displayed the characteristics of MES = 0 patients with and without FBD-like symptoms. When MES = 0, the difference of some indicators between the FBD-like + group and the FBD-like − group was similar to that between the two groups when MH was defined as having an MES = 0 or 1.
Characteristic and clinical disease assessment of mucosal healing patients with functional bowel disorder-like symptoms (FBD-like +) and without functional bowel disorder-like symptoms (FBD-like −).

ALB, albumin; 5-ASA, 5-amino salicylic acid; BMI, body mass index; CRP, C-reaction protein; ESR, erythrocyte sedimentation rate; FBD, functional bowel disorder; GI, gastrointestinal; HADS, Hospital Anxiety and Depression Scale; HB, hemoglobin; HCT, hematocrit; IQR, interquartile range; n, number; N, number; PLT, blood platelet; SD, standard deviation; WBC, white blood cells.
Scores of HADS anxiety and depression: Normal (0–10), abnormal (⩾ 11).
Quality of life and psychological disorders in mucosal healing patients with (FBD-like +) and without functional bowel disorder-like symptoms (FBD-like −), patients without mucosal healing (NMH) and healthy controls (HCs).

FBD, functional bowel disorder; HADS, Hospital Anxiety and Depression Scale; HC, healthy control; IBDQ-32, 32-items Inflammatory Bowel Disease Questionnaire; MH, mucosal healing; NA, not available; NMH, UC patients without mucosal healing; SD, standard deviation; SF-36: short form-36 healthy survey questionnaire.
Scores of HADS anxiety and depression: Normal (0–10), abnormal (⩾ 11).
Factors associated with FBD-like symptoms in UC patients with MH
For UC patients with MH, lower BMI, prolonged duration of disease, lower PLT count, higher occurrence of other functional GI symptoms, and anxiety or depression states were associated with the occurrence of FBD-like symptoms by univariate logistic analysis (Table 5). Next, the variables listed above were entered into the multivariate logistic analysis model. Increased disease duration [odds ratio (OR): 1.022; 95% CI: 1.011–1.033, p < 0.001], decreased BMI (OR: 0.726; 95% CI: 0.612–0.861, p < 0.001) were still significant for FBD-like symptoms in UC patients with MH in the multivariate logistic analysis model (Table 5). For UC patients having an MES = 0, disease duration, BMI, and HB level were significant in the multivariate logistic analysis model (Supplementary Table 6).
Factors associated with the occurrence of functional bowel disorder-like symptoms by univariate and multivariate logistic analysis.

ALB, albumin; 5-ASA, 5-amino salicylic acid; BMI, body mass index; CI, confidence interval; CRP, C-reaction protein; ESR, erythrocyte sedimentation rate; GI, gastrointestinal; HB, hemoglobin; HCT, hematocrit; OR, odds ratio; PLT, blood platelet; WBC, white blood cell.
Predictors of FBD-like symptoms in UC patients with MH
The duration of disease and BMI that were significant in the multivariate logistic analysis model were selected for the construction of ROC curves to predict the occurrence of FBD-like symptoms. We also combined the above variables to test their combined predictive value for the occurrence of FBD-like symptoms (Figure 1). For UC patients with MH, disease duration achieved an area under the ROC curve (AUC; 0.717, 95% CI: 0.626–0.796, p < 0.001), BMI achieved an area under the ROC curve (AUC; 0.695, 95% CI: 0.604–0.776, p < 0.001). Moreover, the combination of disease duration, BMI level attained a higher AUC (0.786, 95% CI: 0.701–0.856, p < 0.001). For UC patients having an MES = 0, the combination of BMI, disease duration, and HB level attained a higher AUC (0.837, 95% CI: 0.707–0.925, p < 0.001, Supplementary Figure 1).
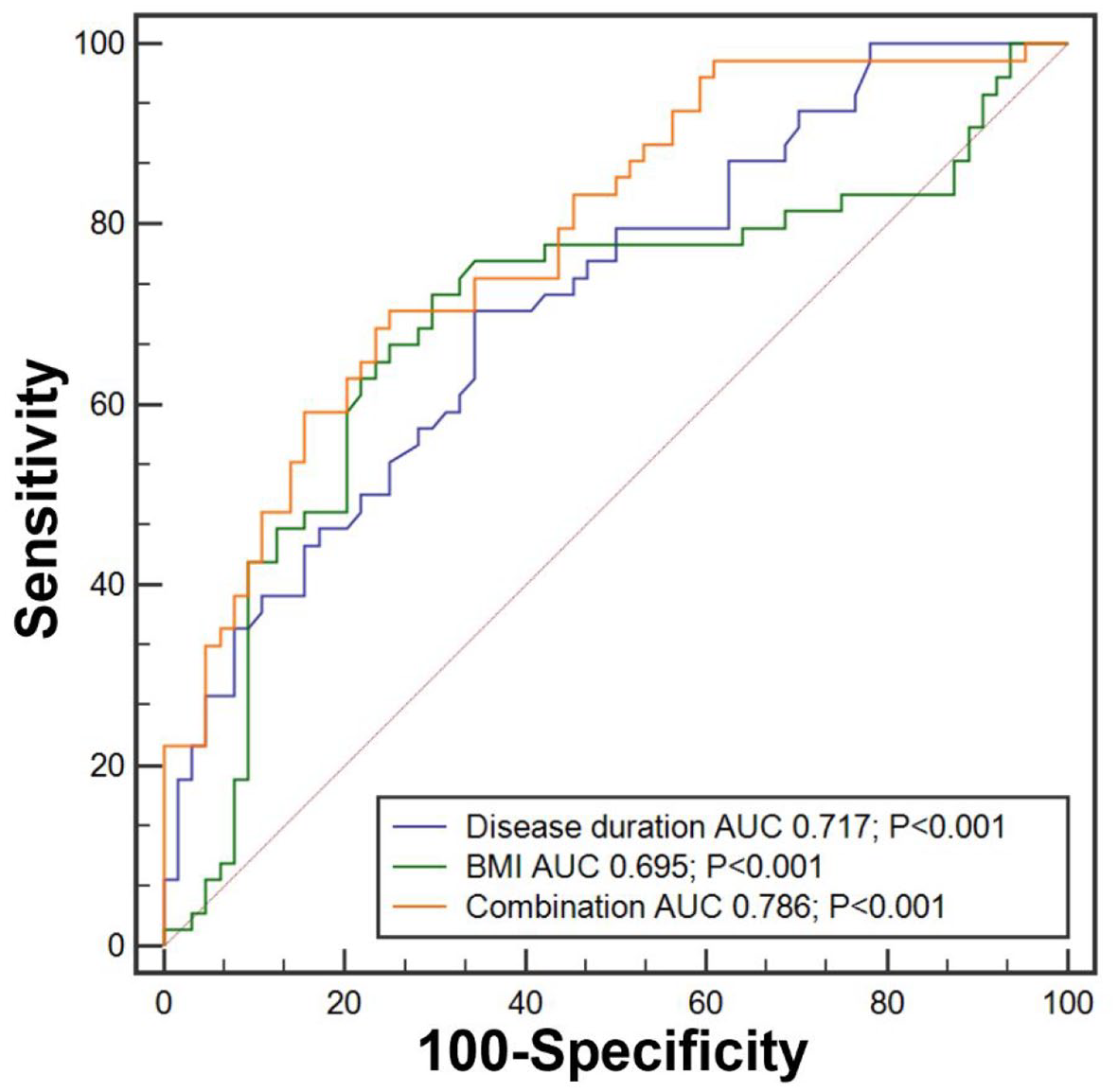
Receiver operator characteristic (ROC) curve that predicted the occurrence of FBD-like symptoms in UC patients with MH. Combination: combined factor of disease duration and BMI.
Discussion
IBS-like symptoms in inactive UC were reported as early as 1983. 24 Our study reported the occurrence of FBD-like symptoms diagnosed using the Rome IV criteria in UC patients with MH. Consistent with our results, functional bowel symptoms were more common in patients with inactive UC than in the general population of Canada. 6 Disease-specific (IBDQ-32) and generic (SF-36) measurement tools indicated poor QoL in UC patients with MH accompanied by FBD-like symptoms. Meanwhile, a combined assessment of disease duration, BMI of UC patients with MH can predict the occurrence of FBD-like symptoms.
We found that the most frequent types of FBD-like symptoms in UC patients with MH were functional constipation-like symptom (13.4%), functional diarrhea-like symptom (10.0%), and IBS-like symptom (10.9%). The occurrence of IBS-like symptom in our study was different from that reported in some studies. This difference may be based on how the diagnosis of IBS was made, in part, on the scoring system. According to the results of the 2021 Rome Foundation Global Study in China, the prevalence rate of IBS according to the Rome IV criteria was 1.4%, whereas that according to the Rome III criteria was 3.8%. 23 The fold difference between the two diagnostic criteria was 2.7. Furthermore, the subject inclusion criteria might have influenced the results. Farrokhyar et al. 6 reported the prevalence of IBS (9.1%), functional abdominal bloating (4.5%), functional constipation (26.2%), and functional diarrhea (11.4%) in inactive UC as defined by patients’ self-reports. Hoekman et al. 25 found a prevalence of IBS (48%) in inactive UC defined by fecal calprotectin < 200 μg/g. Kotani et al. 26 demonstrated that the prevalence of functional diarrhea (5.2%) and IBS (26.7%) in inactive UC, defined by the Rachmilewitz clinical activity index value of 4 for at least 6 months. In Perera et al’.s 27 study, the disease activity index showed that 29% of patients with deep remission met the Rome III criteria for IBS. Participants in our study were selected through objective endoscopic observation, which is the gold standard for UC remission. Both CRP and ESR levels are normal in patients with MH. This meant that the FBD-like symptoms of participants in our study were unrelated to patients’ ongoing inflammation.
Although patients in our study achieved the therapeutic goal of MH, their QoL did not improve when they had functional bowel symptoms. The benefits of MH for patients were offset by FBD-like symptoms. Our study stands out, compared with other studies, because our study supports the improvement in the STRIDE-II guidelines. The combination of theory and example suggests that we must consider factors other than endoscopic healing when determining the extent to which UC patients truly achieve the desired outcome status. Moreover, lower BMI, longer course of the disease may be associated with the occurrence of FBD-like symptoms and impaired QoL. These factors may mask the benefits of MH in UC patients and are worthy of clinicians’ attention. For physicians, early identification and intervention of these factors are conducive to improving the prognosis of the disease. For patients with MH, these factors may also be beneficial to disease management and self-care.
BMI is a common and convenient method of nutritional assessment in patients with IBD. Kim et al. 28 demonstrated that underweight UC patients had a higher risk of escalation treatment and surgery. Guardado et al. 29 found that the postoperative bleeding risk of underweight and overweight IBD patients was higher than that of normal-weight and obese patients. Similar to the above studies, the proportion of underweight patients in the FBD-like + group was higher than in the FBD-like − group. More importantly, the proportion of normal-weight patients was significantly lower in the FBD-like + group than in FBD-like − group.
In our study, the duration of disease was significantly longer in participants with FBD-like symptoms than in those without FBD-like symptoms. Similar findings have been reported previously.7,12,30 According to the existing reports, there may be three links between FBD-like symptoms and the course of disease. Based on the study by Vivinus-Nebot et al., 31 the persistence of high tumor necrosis factor-alpha (TNF-α) levels and subclinical inflammation were found in IBS-like symptoms in quiescent IBD. The longer it takes to achieve remission, the more structural changes there are in the intestine, and the higher the occurrence of IBS-like symptoms after remission. 12 Another possibility is that persistent residual inflammation leads to IBS-like symptoms after remission. 31 Therefore, when communicating with UC patients with a long course of disease clinically, we should pay more attention to their QoL after reaching MH and ask whether there are other intestinal discomforts, rather than rushing to end the consultation.
This study also showed that among patients with FBD-like symptoms, 29.6% experienced an overlap with other functional GI symptoms. Patients with intestinal tract symptoms were more likely to experience discomfort from the anorectum and upper GI tract at the same time. Ford et al. 32 suggested that IBS and dyspepsia have a common pathogenic mechanism. These results indicate that FBD-like symptoms may be attributed to specific unknown effects from other digestive tracts.
In our study, we found states of anxiety or depression in UC patients with MH who reported FBD-like symptoms. This finding is consistent with the literature.27,30,33 Worse psychological outcomes in participants with FBD-like symptoms supported the speculation that anxiety, depression, and other potential psychological factors may be associated with FBD-like symptoms in UC patients without active mucosal inflammation. The underlying mechanism of MH patients accompanied with FBD-like symptoms remains unclear. The Rome Foundation better defined FGID as disorders with gut–brain interaction. Animal experiments have provided potential mechanisms of the interaction between the brain and the intestine. Mice with chronic GI inflammation showed behavioral changes similar to human emotional disorders, 34 while inducing depression in a mouse model with stationary colitis made the disease active again. 35 These findings highlight the importance of psychological states, in addition to disease activity indices (e.g. modified Mayo score, MES), in assessing the state of UC patients’ health. Our study also supports the connection between the brain and the gut.
Our study has several limitations. It is an observational retrospective study that lacks information on the follow-up of participants. For example, an increase in the frequency and cost of clinical visits, examinations, and tests due to FBD-like symptoms, in addition to the necessary periodic review of UC. Despite achieving endoscopic healing, patients with FBD-like symptoms tend to undergo excess interventions, surgeries, or hospital visits due to known organic diseases.27,36 Therefore, a future study should consider this limitation and opt for a better study design. The larger the sample size, the more reliable the research conclusion is. However, in our study, the relatively small number of participants may have been due to the reduction of outpatients and endoscopy patients caused by COVID-19. Telephone or mail surveys may be needed to mitigate this limitation, but these methods tend to have low response rates. Nevertheless, the response rates in our study were > 95%. There were many missing values of fecal calprotectin in the participants. However, the levels of CRP and ESR of participants collected through medical records showed no difference between participants with and without FBD-like symptoms. Crohn’s disease (CD) was not within the scope of our study because it often involves the small intestine. Our enrollment evaluation relied on colonoscopy, which makes it difficult to evaluate the mucosa of the small intestine.
Conclusion
In conclusion, our study reported the occurrence of FBD-like symptoms in UC patients with MH and compared the QoL among the FBD-like +, FBD-like −, NMH, and HC groups. We found a higher proportion of underweight patients, a lower proportion of patients with normal-weight, a longer duration of the disease, a greater proportion of patients who experienced overlap with other functional GI symptoms, poorer QoL, and higher proportion of anxiety and depression states in MH patients with FBD-like symptoms than in those without FBD-like symptoms. We reported predictors of the occurrence of FBD-like symptoms such as disease duration and BMI. This study highlights why the STRIDE-II statements were improved.
Supplemental Material
sj-docx-1-tag-10.1177_17562848221092597 – Supplemental material for Mucosal healing and quality of life in therapeutic goals of ulcerative colitis: occurrence and related factors of functional bowel disorder-like symptoms
Supplemental material, sj-docx-1-tag-10.1177_17562848221092597 for Mucosal healing and quality of life in therapeutic goals of ulcerative colitis: occurrence and related factors of functional bowel disorder-like symptoms by Lihui Lin, Tianqi Wang, Yaming Lu, Peng Chen, Yingfan Zhang, Xiaoman Zu, Baili Chen, Ren Mao, Rui Feng, Yi Cui, Shenghong Zhang and Yao He in Therapeutic Advances in Gastroenterology
Footnotes
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a grant from the National Natural Science Foundation of China (Grant no. 81670607, Grant no. 81870374, Grant no. 81670498), Guangdong Science and Technology (Grant no. 2017A030306021), and the Fundamental Research Funds for the Central Universities (Grant no. 19ykzd11).
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.