
Abstract
As biologic-based medication options for ulcerative colitis expand, our understanding of their optimal use in clinical practice is advancing as well. The appropriate use of combination therapy with immunomodulators can reduce the immunogenicity of biologic agents and raise serum drug levels of the biologic. A treat-to-target strategy with objective assessments of disease activity clearly defines the goals of biologic drug treatment. Mucosal healing is an evolving treatment goal and is associated with long-term remission and reduced incidence of colectomy. Furthermore, regular reassessments and therapeutic drug monitoring can allow clinicians to make evidence-based changes in therapy. Biologic drug de-escalation or re-initiation are less well developed topics, but are emerging areas of study. We review the evidence underlying these advances and a modern approach to the use of biologic therapy in ulcerative colitis.
Introduction
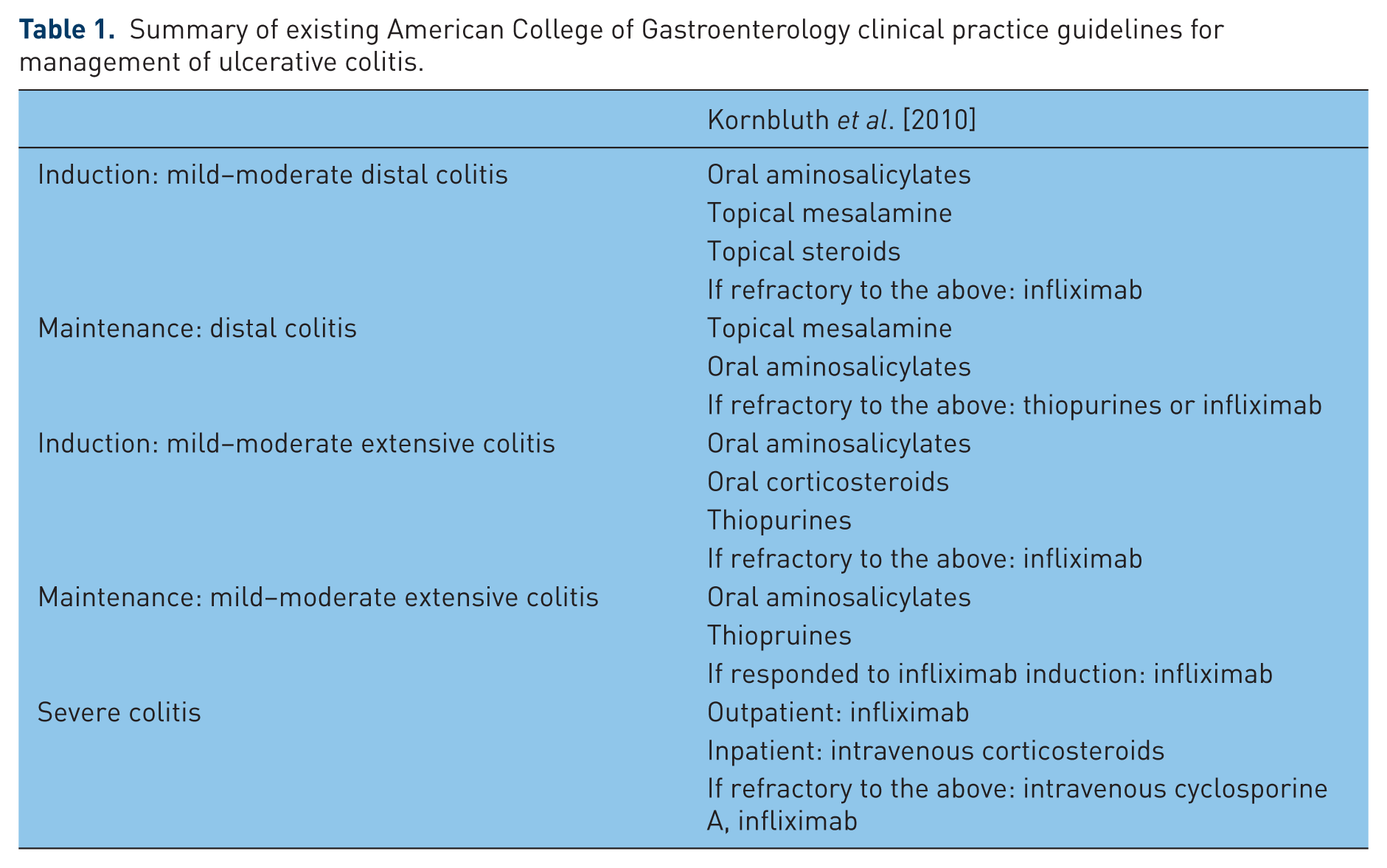
Ulcerative colitis (UC) is a chronic, idiopathic, inflammatory disease of the colon. Current understanding of the pathogenesis suggests that a dysregulated immune response to environmental and microbial stimuli leads to UC in a genetically susceptible host [De Souza and Fiocchi, 2016]. There is significant morbidity and mortality associated with active UC. Recent cohort studies estimate that 4.1–14.8% of patients with UC undergo colectomy during their disease course [Solberg et al. 2009; Targownik et al. 2012; Jeuring et al. 2015]. For years, management primarily included the use of 5-aminosalicylates, corticosteroids, azathioprine, and surgery. The introduction of biologic-based therapies for UC has revolutionized the management of this disease. Guidelines and consensus statements recommend biologic-based therapies as an option for the management of moderate to severe UC (Table 1) [Kornbluth et al. 2010; Bressler et al. 2015]. Biologic therapies are an essential component for the modern medical management of UC. For the patients that have the most active disease and a higher risk of adverse outcomes, biologic therapy can achieve remission [Rutgeerts et al. 2005; Reinisch et al. 2011; Sandborn et al. 2012, 2014].
Summary of existing American College of Gastroenterology clinical practice guidelines for management of ulcerative colitis.
Our understanding of the implications of using biologic therapies in clinical practice is advancing as ever more drug options and drug tests achieve regulatory approval. This review addresses the evidence supporting optimal clinical application of currently available biologic therapies for UC, as well as their treatment goals, diagnostic tests, and methods for adjusting therapy.
Choice of therapy
Available biologic drug options
After identifying a patient for biologic therapy, the clinician must choose an agent and decide whether to use combination therapy. There are currently four approved biologic medications divided by mechanism of action between antitumor necrosis factor α (anti-TNFα) and anti-integrin. Anti-TNFα biologic medications act by binding directly to the proinflammatory cytokine TNFα. Infliximab is an anti-TNFα biologic delivered as an intravenous infusion. After a loading period, typical dosing varies between 5 and 10 mg/kg at an interval of 8 to 4 weeks. Adalimumab is the subsequently approved anti-TNFα biologic medication and is a subcutaneous injection. After a loading period, the dosing is 40 mg, typically every 2 weeks or up to weekly. The next approved anti-TNFα biologic medication for UC is golimumab, which is also a subcutaneous injection. Dosing of golimumab is 100 mg every 4 weeks. Next, vedolizumab is a new biologic medication that uses an alternative mechanism of action. Vedolizumab binds to the α-4-β-7 integrin (α4β7) leukocyte adhesion molecule and prevents leukocytes from migrating to intestinal foci of inflammation. Vedolizumab is an intravenous infusion dosed at 400 mg every 8 weeks after a loading period. The clinician’s choice of medication needs to account for prior biologic medication exposures, response to prior therapies, and any history of adverse drug effects.
There are special circumstances that clinicians encounter in practice that influence their choice of biologic therapy, including patients with a history of cancer, older patients, and hospitalized patients. First, a history of cancer is not a contraindication for biologic therapy. A recent retrospective study found that there was no increase in new or recurrent cancers in patients treated with anti-TNFα medications [Axelrad et al. 2016]. In this situation, the clinician can use the biologic agent of their choosing based on other clinical features. We have generally recommended using vedolizumab as a first line biologic therapy for patients with UC older than 60 years. There is evidence that older patients on anti-TNFα therapy experience serious infections more commonly than in younger patients with UC receiving anti-TNFα therapy [Cottone et al. 2011]. However, we recommend using infliximab as first-line biologic therapy in patients hospitalized with severe UC. Although somewhat limited, data support the use of infliximab as an effective therapy in this setting [Sands et al. 2001; Jarnerot et al. 2005]. Finally, a practical reality is that payers may not allow use of vedolizumab prior to anti-TNF therapies. Many policies in the US require “step-failure” of one or even two anti-TNF therapies prior to allowing use of vedolizumab. In these situations, we have appealed the decision, particularly when the patient is a primary nonresponder to one anti-TNF and the payer requires a second one. Unfortunately, this has only been partially effective in securing approval of vedolizumab.
Combination therapy
The clinician should subsequently consider whether a patient requires the use of a biologic medication in combination with an immunomodulator. Panaccione and colleagues published the evidence to support this strategy in a randomized, double-blind, double-dummy, placebo-controlled trial of infliximab monotherapy, azathioprine monotherapy, or combined therapy with infliximab and azathioprine for patients with moderate to severe UC known as the UC SUCCESS trial [Panaccione et al. 2014]. A higher percentage of patients receiving combination therapy achieved corticosteroid free remission by week 16 than with infliximab monotherapy (39.7% versus 22.1%) or azathioprine monotherapy (39.7% versus 23.7%). In addition, a higher percentage of patients receiving combination therapy achieved mucosal healing by week 16 (62.8%) than with azathioprine monotherapy (54.6% with infliximab; 36.8% with azathioprine).
Combination therapy results in superior outcomes by reducing immunogenicity of biologic agents and raising serum biologic drug levels. The UC SUCCESS trial showed that more patients receiving infliximab monotherapy developed positive anti-infliximab antibodies than those patients receiving combination therapy [Panaccione et al. 2014]. In addition, patients on infliximab monotherapy have lower infliximab drug levels than patients on combination therapy with azathioprine. Yarur and colleagues showed that a higher level of serum 6-thioguanine nucleotides positively correlated with serum infliximab level (correlation coefficient 0.52) [Yarur et al. 2015].
The clinician should also be sure to use evidence-based immunomodulator dosing when instituting combination therapy. For thiopurine immunomodulators, patients with a 6-thioguanine (6-TG) nucleotide level of less than 125 pmol/8×108 red blood cells (RBCs) have a significantly higher likelihood of having detectable anti-infliximab antibodies (odds ratio 13) [Yarur et al. 2015]. A methotrexate dose of 15 mg or more weekly in combination with an anti-TNFα biologic was associated with longer duration of clinical remission in a retrospective review of patients with inflammatory bowel disease (IBD) at our institution [Colman and Rubin, 2015].
Measurement of disease activity
It is necessary to establish an objective determination of disease activity prior to initiating treatment. An objective measurement determines the appropriateness of the treatment decision and provides a guide for future assessment of response to therapy. The Mayo score is a useful tool for measuring UC disease activity [Schroeder et al. 1987]. The Mayo score includes an objective assessment of disease activity by endoscopic appearance, and clinical assessments by stool frequency, rectal bleeding, and the physician’s global assessment. The Mayo endoscopic subscore ranges from 0 to 3. An endoscopic subscore of 0 represents normal appearance or inactive disease. An endoscopic subscore of 1 is mild disease with erythema, mild friability, erosions, and loss of normal vascular pattern. An endoscopic subscore of 2 is moderate disease with marked erythema, absent vascular pattern, friability, and erosions. An endoscopic subscore of 3 represents severe disease with spontaneous bleeding and ulceration. Mucosal healing is a Mayo endoscopic subscore of 0 or 1 [D’Haens et al. 2007; Pineton De Chambrun et al. 2010]. This definition of mucosal healing is a treatment outcome in each of the major trials of biologic medications in UC [Rutgeerts et al. 2005; Reinisch et al. 2011; Sandborn et al. 2012, 2014; Feagan et al. 2013].
Treat-to-target
Recently, a multinational committee of 33 experts in IBD published evidence-based recommendations for treatment goals in UC [Peyrin-Biroulet et al. 2015]. Even though they recognized clinical remission as a goal, it is not sufficient on its own and requires an objective measurement of disease activity. They recommended using the endoscopic Mayo score as an objective treatment goal based on the available evidence. The recommended target Mayo endoscopic subscore is 1 or 0, with 1 as the minimum target and 0 as an optimal outcome. Meanwhile, the authors acknowledged the prognostic value of histologic findings but their role in clinical practice is not yet clear. In addition, levels of the surrogate markers, C-reactive protein and fecal calprotectin, are not appropriate treatment goals by themselves. Noninvasive testing with C-reactive protein and fecal calprotectin are useful as adjuncts to monitoring therapy, and should prompt objective endoscopic measurement of disease activity if levels are not responding to therapy.
Mucosal healing
Mucosal healing is the recommended treatment target in UC because endoscopic inflammatory activity is closely associated with risk for colectomy and likelihood of long-term remission. Carbonnel and colleagues showed that endoscopically defined disease severity was significantly associated with the risk of colectomy. They defined severe disease as deep/extensive ulcers, mucosal detachment, large mucosal abrasions, or well like ulcers, and defined moderate disease as superficial ulcers or ulcers that were deep but not extensive. Of the patients with severe disease, 93% required subsequent colectomy compared with 23% of patients with moderately active disease [Carbonnel et al. 1994]. Similarly, in a Norwegian observational cohort, patients who achieved mucosal healing at 1 year of treatment were less likely to undergo colectomy in the next 4 years regardless of treatment exposure (relative risk (RR) 0.22) [Froslie et al. 2007]. Meucci and colleagues later studied patients with UC in clinical remission and showed that endoscopic inflammation predicted disease relapse. Patients who achieved both endoscopic and clinical remission by 6 weeks had a significantly lower rate of disease relapse in the following 12 months (23%) than those patients who achieved clinical remission alone (80%) [Meucci et al. 2012]. Furthermore, complete endoscopic response to a Mayo endoscopic subscore of 0 predicts an even greater likelihood or long-term remission. Yokoyama and colleagues studied patients in clinical remission stratified by Mayo endoscopic subscore and reported remission rates for the following 5 years. Patients with a Mayo endoscopic subscore of 0 maintained remission at 100% in 6 months and 78% at 5 years. This was significantly different than patients with scores of 1, 2, or 3 at 6 months (93%, 70%, 50% respectively) and 5 years (40%, 10%, 0% respectively) [Yokoyama et al. 2013].
Histologic healing
Histologic healing is a closely related concept to mucosal healing. Histologic healing is not a recommended treatment target, even though there is evidence that it is associated with improved outcomes. A study by Riley and colleagues obtained rectal biopsies in 82 patients with UC who were in clinical remission on sulfasalazine or mesalamine. They determined that the histologic findings that predicted clinical relapse within 12 months were acute inflammatory cell infiltrate, crypt abscesses, mucin depletion, and breached surface epithelium [Riley et al. 1991]. Furthermore, data from our institution showed that patients who achieve complete histologic normalization were significantly less likely to experience clinical relapse than either patients with histologic activity or histologic quiescence [Christensen et al. 2015].
Histologic inflammatory activity is an important consideration because it is associated with risk for colorectal neoplasia. Rutter and colleagues performed a case-control study to determine the association between histologic inflammation on surveillance colonoscopy and later development of colonic dysplasia [Rutter et al. 2004]. They found that each incremental increase in histologic severity score increased the odds of colorectal neoplasia by 4.69. Furthermore, we previously performed a case-control study of patients with UC who had developed colorectal neoplasia matched to control patients with UC [Rubin et al. 2013]. On multivariate analysis, mean histologic score and male sex were significantly associated with colorectal neoplasia. Each one unit increase in histologic activity index score was associated with an adjusted odds ratio of 3.68.
Treating to achieve a target: is it a practical end point?
Mucosal healing is a practical therapeutic goal that is achievable with available medical therapy in many patients. Bouguen and colleagues performed a retrospective review of patients with UC undergoing at least two consecutive endoscopic assessments [Bouguen et al. 2014]. They strictly defined mucosal healing as the absence of any type of friability or erythema from inactive disease equivalent to a Mayo endoscopic subscore of 0. Patients without mucosal healing who had changes in therapy were more likely to achieve mucosal healing and histologic healing during the follow-up period (median 76 weeks). Furthermore, in a multivariate analysis, any therapeutic change after demonstration of disease activity was associated with a hazard ratio (HR) of 9.8 for achieving mucosal healing and an odds ratio of 9.2 for achieving histologic healing. These findings suggest that a clinician can target mucosal healing through the treat-to-target strategy. We recommend considering mucosal healing as the target therapeutic goal in all patients with UC, but we acknowledge that we currently do not know if all patients are equally capable of achieving mucosal healing and some may still require colectomy. The balance must occur between escalating therapy to achieve healing when the patient may already feel better or have achieved clinical remission.
Short interval reassessment
Once a patient starts biologic therapy for UC, a short interval reassessment is important for determining response to therapy and helping guide treatment decisions. Anti-TNFα medication response can occur as early as 2–4 weeks and peaks by week 16 of treatment [Rutgeerts et al. 2005; Reinisch et al. 2011; Sandborn et al. 2012, 2014]. Peak effect of vedolizumab in UC occurs by week 6 of treatment [Feagan et al. 2013]. A recent consensus statement recommends reassessment of anti-TNFα therapies by 8–12 weeks of treatment and reassessment of vedolizumab therapy by 8–14 weeks of treatment [Bressler et al. 2015]. We recommend assessing for clinical response combined with an objective marker of disease activity, which can include fecal calprotectin, serum C-reactive protein level, or endoscopic assessment.
Serum drug levels, optimal serum targets
We recommend that the clinician considers measuring the biologic drug serum concentration because early assessment of drug levels correlates with longer-term response and mucosal healing. There is a significant positive correlation between anti-TNFα drug concentration in serum and in healed tissue (r = 0.50). Meanwhile, tissue with the highest degree of inflammation has the lowest levels of anti-TNFα drug [Yarur et al. 2016]. This suggests that patients with a higher burden of inflammation may require higher anti-TNFα exposure to control their disease. Vaughn and colleagues studied the effect of proactive infliximab concentration monitoring in a cohort of patients with IBD. They found that patients with infliximab trough concentration of greater than 5 μg/ml had a higher probability of remaining on infliximab (HR 0.1). At 5 years, the probability of remaining on infliximab was 86% in the group with proactive concentration monitoring compared with 52% in the group without proactive monitoring [Vaughn et al. 2014]. The active UC trials 1 and 2 (ACT-1 and ACT-2) of infliximab in UC showed that a level of infliximab of 41 μg/ml at week 8 had a positive predictive value for clinical response of 80%. Furthermore, patients with higher levels of infliximab at week 8 had a higher likelihood of maintaining remission by week 30 [Adedokun et al. 2014]. Seow and colleagues similarly showed that the presence of a detectable infliximab trough was significantly associated with higher likelihood of remission and reduced risk for colectomy [Seow et al. 2010]. Similarly, Roblin and colleagues found that higher trough levels of adalimumab were significantly associated with a higher likelihood of mucosal healing in a cohort of patients with UC and Crohn’s disease [Roblin et al. 2014].
There are several commercially available serum tests for infliximab and adalimumab drug level and antidrug antibody levels, but there are none currently available for golimumab or vedolizumab. The commercially available tests for infliximab and adalimumab differ by their methods of detection. Table 2 summarizes the available tests for infliximab and adalimumab. The initial tests were enzyme-linked immunosorbent assay (ELISA) based, followed by electrochemiluminescence immunoassay (ECLIA). However, these tests are limited because they cannot detect antidrug antibodies in the presence of drug. Prometheus Laboratories (San Diego, CA, USA) developed a homogenous mobility shift assay (HMSA) that is able to simultaneously measure drug concentrations and antidrug antibody concentrations [Wang et al. 2012]. Validation of the HMSA methodology showed that it was more sensitive at indentifying anti-infliximab antibodies than an ELISA-based methodology. An HMSA based test for adalimumab was also developed and the test characteristics were better than older ELISA and ECLIA based tests [Egea-Pujol et al. 2013]. However, cost and availability at different institutions limit choice of assay for some patients and providers.
Available serum tests for infliximab and adalimumab concentrations and antidrug antibody concentrations.

ECLIA, electrochemiluminescence immunoassay; ELISA, enzyme-linked immunosorbent assay; HMSA, homogenous mobility shift assay; LC-MS/MS, liquid chromatography, tandem mass spectrometry; N/A, test not available.
Serum drug levels can provide useful information to optimize anti-TNFα medications based on this evidence (Figure 1). The clinician can measure drug trough level and antidrug antibodies at approximately 12–14 weeks of therapy. If the drug level reaches an optimal level, then continued disease monitoring at 6–12-month intervals is appropriate. However, if it does not reach an optimal level, then the clinician must assess for potential causes of a low drug level and make adjustments in therapy as indicated. Follow-up reassessment and repeated measurement of drug level and antidrug antibodies is appropriate to help attain optimal use of the drug.

Proactive approach to optimization of anti-tumor necrosis factor (TNF) α therapy in ulcerative colitis. ADA, antidrug antibody.
Adjusting therapy
Following a reassessment of the patient’s disease activity and consideration of the patient’s drug levels, the treating gastroenterologist should adjust biologic drug dosing, start an immunomodulator, or optimize immunomodulator dose.
Change biologic drug dosing
Induction dosing of infliximab guided by a patient’s inflammatory status can achieve a greater likelihood of response. Gibson and colleagues retrospectively compared the standard infliximab dosing regimen with an accelerated dosing regimen in patients hospitalized with acute severe UC [Gibson et al. 2015]. Clinically evident recurrence of inflammation determined the accelerated induction dosing schedule. They showed a lower rate of colectomy during the induction phase in patients given the accelerated dosing regimen than in patients given the standard regimen (6.7% versus 40%) [Gibson et al. 2015]. In the multivariate analysis of these patients, accelerated dosing of infliximab and serum albumin level were independently associated with avoidance of colectomy during induction. However, the colectomy rate was similar between the two groups in the 2 years of follow up after induction. Because of this study, some referral centers are using accelerated dosing schedules for select hospitalized patients, particularly with hypoalbuminemia, but this practice requires further study.
A possible underlying cause of primary nonresponse to infliximab therapy is rapid clearance due to fecal losses of the drug and high inflammatory burden. A study by Brandse and colleagues showed that high fecal loss of infliximab in the first days after induction is associated with primary nonresponse in moderate–severe UC, possibly due to decreased exposure to the active drug [Brandse et al. 2015]. They also identified that patients with lower serum albumin levels had significantly higher fecal infliximab concentrations on day 1 and significantly lower serum infliximab concentrations at week 2. In a separate study, Brandse and colleagues showed that a C-reactive protein baseline level greater than 50 mg/liter predicted a significantly lower degree of drug exposure during standard infliximab induction dosing [Brandse et al. 2016]. Biologic drug pharmacokinetics are complex and further prospective research needs to determine if this explains the mechanism of benefit from accelerated drug dosing.
Additionally, increasing biologic dose or switching biologic guided by drug and antidrug antibody levels can recapture response if a patient experiences secondary loss of response (Figure 2). Paul and colleagues showed that an increase of infliximab level by more than 0.5 ug/ml was associated with increased mucosal healing by a likelihood ratio of 2.02 [Paul et al. 2013]. In addition, a retrospective study of patients with IBD by Afif and colleagues showed that consideration of both the infliximab level and anti-infliximab antibody level can help guide an optimal change in therapy [Afif et al. 2010]. Dose escalation in response to inadequate drug levels was associated with complete or partial clinical response in 86% while a change to another anti-TNFα drug only recaptured 33% of patients. In addition, for patients with positive anti-infliximab antibody levels, a change to another anti-TNFα drug achieved complete or partial clinical response in 92% while an increase in dose only recaptured 17%. However, more research is needed given conflicting results from the TAXIT trial in which no change in clinical remission was identified in patients with UC who underwent protocolized dose escalation of infliximab [Vande Casteele et al. 2015]. An important limitation to the TAXIT trial was that most of the patients with UC who underwent dose escalation were already in clinical remission and therefore could not improve.
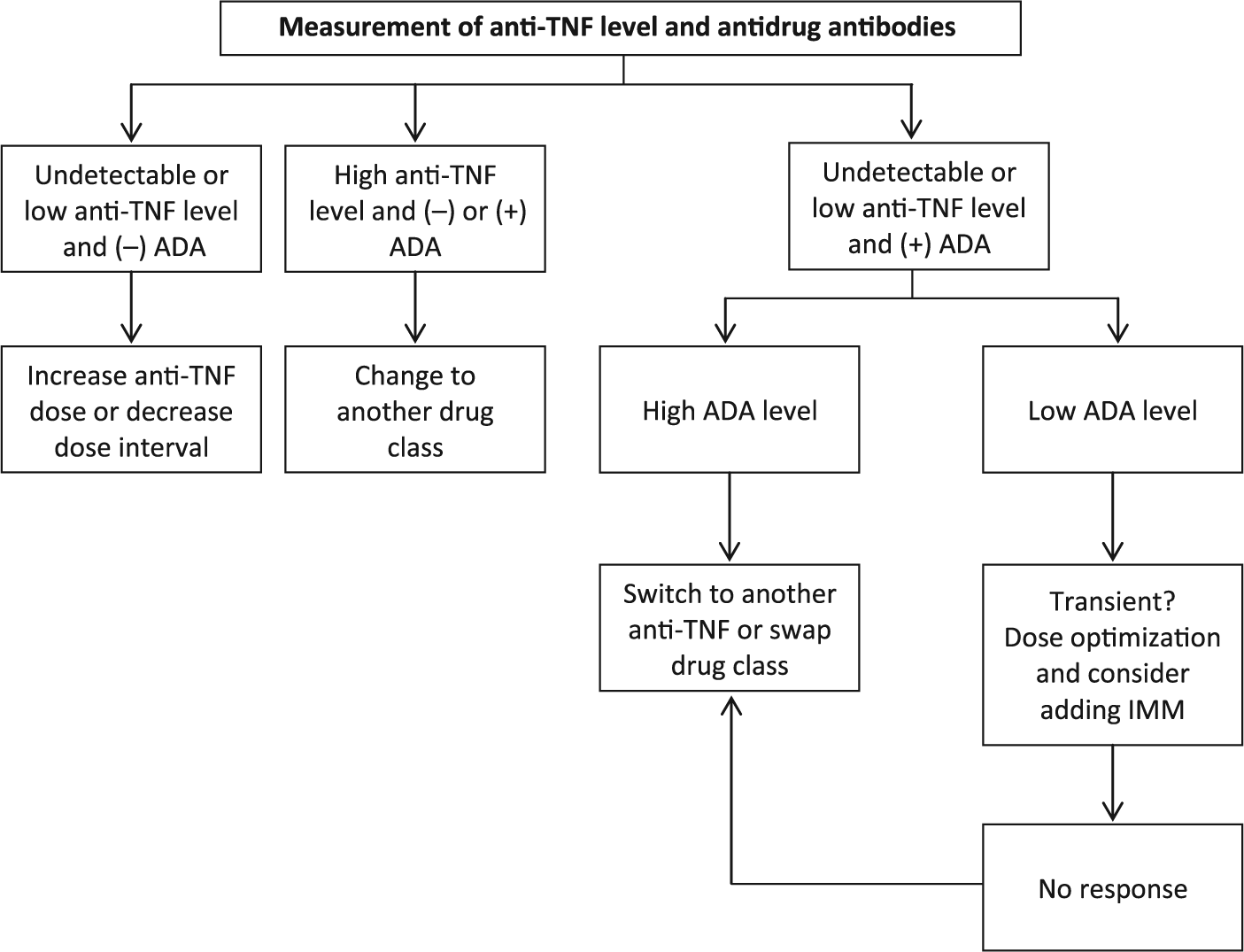
Reactive approach to the patient losing response to anti-tumor necrosis factor (TNF) therapy using therapeutic drug monitoring. ADA, antidrug antibody; IMM, immunomodulator.
Addition of an immunomodulator
There is also evidence that antibodies to infliximab may be transient and addition on an immunomodulator can overcome them. Vande Castelle and colleagues found that antibodies to infliximab were transient in 28% of patients [Vande Casteele et al. 2013]. Only 13% of these patients with transient antibodies to infliximab had to discontinue infliximab, compared with 68% of patients with persistently positive antibodies (RR 5.1). Ben-Horin and colleagues showed that adding an immunomodulator could overcome antibodies to infliximab [Ben-Horin et al. 2013]. All of the five patients included were able to stay on infliximab and saw antibody levels decreased while infliximab trough levels increased.
Optimization of immunomodulator dosing
In addition to changes in biologic dosing and choice of therapy, dose escalation of thiopurine immunomodulators can target higher serum levels of 6-TG nucleotide levels. 6-TG levels less than 125 pmol/8×108 RBCs are associated with higher anti-infliximab antibodies and higher 6-TG levels are associated with clinical remission [Osterman et al. 2006; Yarur et al. 2015].
De-escalation of therapy
Patients often ask about the circumstances under which biologic drug therapy can be de-escalated, but there is little evidence available currently about the safety and efficacy of this consideration. A recent systematic review and meta-analysis identified 14 studies describing de-escalation of an anti-TNFα biologic. Relapse rates varied between 14% and 41.8% at 12 months and between 35% and 47.1% at 24 months [Torres et al. 2015]. Among these studies was a retrospective study by Steenholdt and colleagues that followed 28 patients with UC in clinical, steroid-free remission after discontinuation of an anti-TNFα biologic medication [Steenholdt et al. 2012]. At 1-year follow up, 75% remained in remission, however 40% remained in remission at 4.5 years of follow up. However, the study did not define remission based on objective findings and relapse was limited to surgery, hospitalization, or need for reintroduction of an anti-TNFα biologic.
Serial fecal calprotectin measurements may be able to monitor for elevated risk of relapse after anti-TNFα de-escalation. A study by Molander and colleagues prospectively followed patients with IBD in clinical and endoscopic remission for 1 year following discontinuation of anti-TNFα therapy [Molander et al. 2015]. They found a significant increase in median fecal calprotectin levels at 2, 4, and 6 months prior to endoscopic relapse.
In order to de-escalate therapy, we recommend the following steps: assess for deep remission; choose a de-escalation strategy; monitor for subclinical relapse; and have a rescue strategy. In our clinical practice, we define deep remission as clinical remission combined with an objective measure of inflammatory control. This objective measure may be mucosal healing on endoscopy or a normal C-reactive protein level. Histologic healing is currently used as an adjunct, and it is not required for deep remission. When we have performed therapeutic de-escalation, we monitor for subclinical relapse with serial fecal calprotectin measurements, serial C-reactive protein levels, or planned endoscopy. We typically perform fecal calprotectin measurements every 3 months for at least the first year after discontinuation. The interval between de-escalation and planned endoscopy depends on the therapy that was discontinued. There are limited data to support this practice in UC at the current time.
Reinitiating a previous therapy
Several studies suggest that drug reinitiation is a viable option to consider if disease relapses following drug withdrawal. Farkas and colleagues prospectively followed patients with UC who had stopped infliximab therapy [Farkas et al. 2013]. In the patients with recurrent disease activity that were retreated with infliximab, 94% achieved clinical remission. Baert and colleagues found that absent antibodies to infliximab after a first re-exposure and concomitant immunomodulator therapy were associated with short-term response [Baert et al. 2014]. They also found that patients who stopped therapy because of remission were more likely to have long-term response to infliximab after re-exposure. Molander and colleagues performed a multicenter trial of anti-TNFα discontinuation in patients with IBD [Molander et al. 2014]. Among the 10 patients with UC who relapsed after anti-TNFα discontinuation, 9 (90%) were in clinical remission at 12 months after reinitiating anti-TNFα therapy.
We have synthesized the available evidence into a modified clinical algorithm for restarting infliximab at our institution (Figure 3). The Chicago Algorithm for Restarting Infliximab begins with a patient who has had at least 6 months without infliximab after having lost response or intentionally discontinuing infliximab therapy. Next, the patient receives a first dose of infliximab with premedication. We use a dose of prednisone of 40 mg the day before infusion and an additional dose of prednisone of 40 mg with acetaminophen 650 mg and diphenhydramine 25 mg on the day of the infusion. One week later the patient has a test for infliximab level and antibodies to infliximab. If the patient has a detectable level and negative antibodies, then they continue with standard infliximab induction dosing at weeks 2 and 6, followed by maintenance doses. If the patient has positive antibodies to infliximab, they do not receive any further doses and we consider alternative therapeutic options.

Chicago algorithm for restarting infliximab. Based on available evidence and modified from Baert et al. [2014]. Premedications include one dose of oral prednisone 40 mg the day before the first loading infusion and on the day of the first loading infusion, with one dose of oral diphenhydramine 25 mg and one dose of oral acetaminophen 650 mg. ATI, antibody to infliximab; IFX, infliximab.
Conclusion
The optimal use of biologic agents depends on choosing the appropriate medication strategy, following response to therapy, and adjusting treatment plans based on available evidence. Our understanding of biologic therapies has increased significantly since their initial approval for use in IBD. The available biologic medications remain limited in number and careful use is essential for patients to receive maximum benefit.
Integrating objective treatment goals and therapeutic drug monitoring into clinical practice is a significant development in managing patients with UC. With objective assessments, clinicians can clearly define disease activity and response to therapy. This is an invaluable tool to address a patient’s concerns and symptoms in an evidence-based way. In addition, therapeutic drug monitoring allows the clinician to understand the patient’s disease activity in the context of their biologic drug treatment. By clearly characterizing the patient’s drug levels and antidrug antibody status, the clinician can make informed decisions on dosing and make changes in therapy that are more judicious.
Despite these advances, biologic therapy for UC needs further research to improve our clinical decision making and improve patient care. There is little prospective evidence comparing drug therapies and treatment strategies. In addition, there is more to learn about the optimal time to initiate therapy and about the role for newer targeted agents early in the disease course or in less active disease. These findings could help determine optimal, customized biologic therapy for individuals with UC in the future.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
Dr. Sofia has served as an educational consultant for Janssen. Dr. Rubin has served as a consultant and received grant support from AbbVie, Janssen, Takeda, UCB, Amgen, Pfizer, and Prometheus.