
Abstract
Background:
Depression and anxiety are common among inflammatory bowel disease (IBD) patients. Not only do they worsen quality of life, but also worsen the prognosis of the IBD. Yet, there are no widely accepted guidelines for screening for depression or anxiety in this population. The Hospital Anxiety and Depression Scale (HADS) is a self-administered questionnaire designed to measure anxiety and depression in the physically ill. The purpose of this study was to establish the utility of the HADS as a screening tool in IBD patients.
Methods:
Seventy-nine IBD patients (age 29.86 ± 8.36, 51.9% female, 77.2% Crohn’s disease) were recruited consecutively at the day treatment unit, Gastroenterology Department, Sheba Medical Center. They were asked to complete the HADS, the Beck Depression Inventory (BDI), and the State-Trait Anxiety Inventory (STAI). The scores of the HADS depression and anxiety subscales were correlated with the BDI and STAI scores, and the rates of above-threshold scores were calculated and compared between the three questionnaires and findings from previous studies.
Results:
The two HADS subscales significantly correlated with and the BDI (rs = .69, p < 0.001) and STAI state and trait anxiety (rs = .853, p < 0.001; rs = .744, p < 0.001, respectively). The usual HADS cut-off scores yielded adequate rate of anxiety but lower than expected depression rates.
Conclusions:
Our findings suggest the HADS as a valid screening tool for anxiety and depression in IBD patients. We recommend administering it routinely in gastrointestinal (GI) follow-ups using a lower cut-off score for depression than anxiety (greater than 7 vs greater than 11, respectively).
Keywords
Introduction
Depression and anxiety are increasingly diagnosed worldwide and have substantial consequences, including high morbidity and mortality.1–3 According to the World Health Organization’s current estimates, 264 million people are dealing with depression globally, and it is a leading cause of disability and a major contributor to the overall global burden of disease. 4 Alongside with anxiety, these two mental disorders cost world economies about 1 trillion dollars each year. 5 Even mild levels of depression are associated with loss of productivity. 6
The disease burden and disability of inflammatory bowel diseases (IBDs) are also significant, as patients suffer from a myriad of gastrointestinal symptoms as well as extra-intestinal manifestations. 7 In recent years, a great deal of attention has been given to the psychological burden of IBD. Previous studies have examined depression and anxiety among IBD patients, and it is well established that IBD is associated with high rates of both.8–10 Moreover, disease activity, clinical recurrence, and prognosis were all found to be significantly associated with symptoms of depression and anxiety.11–13 As the link between body and soul in IBD is thought to be bidirectional, these mental conditions may be the result of active IBD, but may also play a role in triggering or intensifying physical symptoms in patients with IBD.14,15 This points to the need of mental health screening as part of a holistic treatment approach. To the best of our knowledge, there are no generally accepted guidelines for the matter.
As there are no relevant laboratory or imaging techniques, the diagnosis of depression or anxiety is based solely on anamnesis, and according to the criteria of the Diagnostic and Statistical Manual (DSM) of the America Psychiatric Association. 16 This causes two major caveats: First, the diagnosis is influenced by the subjectivity of the patient and the doctor. Second, the diagnoses are dichotomous, meaning a patient will be classified as either being depressed/anxious or not, which is an over-simplification of the human condition. A possible way to cope with these limitations is the use of questionnaires. Although not free of fault, questionnaires allow for a bit more objectivity about the patient’s mental state and for a more delicate assessment of the degree of depressive or anxious symptoms. Indeed, over the years different scales were developed and used in various settings and contexts.
The Hospital Anxiety and Depression Scale (HADS) was developed as a screening tool for depression and anxiety in hospitalized patients who may need further mental health evaluation and assistance. The HADS differs from ‘traditional’ depression and anxiety questionnaires mainly due to its focus on nonphysical symptoms, in the attempt to avoid false-positive results in physically ill patients. 17 For example, it does not contain questions about appetite changes or fatigue, although both are part of the criteria of depression in the DSM. 16 The HADS was previously validated for IBD patients in Mexico 18 and Canada 19 and used in other studies for assessment of anxiety and depression among IBD patients.8,20,21
The aim of this study was to establish the utility of the Hebrew version of the HADS as a screening tool in Israeli IBD patients, by comparing its scores with wildly accepted and used depression and anxiety questionnaires: the Beck Depression Inventory (BDI) and the State-Trait Anxiety Inventory (STAI). Both are validated, highly cited, and commonly used questioners22,23 and are considered by many to be the ‘gold standard’ for the screening of depression and anxiety correspondingly. Besides being adapted to physically ill population, the HADS questionnaire is significantly shorter than the BDI and STAI; while the two contain about 60 questions together, the HADS includes only 14.
Materials and methods
Study design and participants
Seventy-nine IBD patients (age 29.86 ± 8.36, 51.9% female, 77.2% Crohn’s disease – CD) were included in this study. Participants were recruited at the day treatment unit, Gastroenterology Department, Sheba Medical Center, between June 30, 2020, and April 7, 2021. In the unit, patients arrive regularly to be treated with intravenous medication (e.g. infliximab).
The participants were asked to provide demographic data (sex, age, IBD diagnosis, current medication, and psychiatric background) and then completed questionnaires regarding their mental state. As part of the initial screening conversation, all participants were asked about their medical treatment and none of them declared using psychotropic medication. Patients with a known major psychiatric disorder, including psychotic disorders, bi-polar disorder, and autism spectrum disorders, were excluded to control for potential confounding. The study was approved by Sheba’s Internal Review Board (approval number 6007-19-SMC), and all of the participants gave their informed consent in writing.
Questionnaires
Hospital Anxiety and Depression Scale (HADS): A self-report questionnaire for the assessment of physically ill or hospitalized patients. It contains 14 items that are scored on a 4-point Likert-type scale, ranging from 0 to 3, and are divided into two subscales measuring cognitive and emotional symptoms of depression (HADS-D) and anxiety (HADS-A). The total score on each subscale ranges from 0 to 21, and higher score represents worse symptoms. A score equal to or greater than 8 on either HADS-D or HADS-A is considered to be a ‘possible case’, and above 11 a ‘probable case’. 17 The questionnaire was translated to Hebrew and validated in cardiac patients. 24
Beck Depression Inventory (BDI): An established and wildly used, self-report screening questionnaire. It consists of 21 items designed to measure depressive symptoms in the prior week. The items of the BDI are scored on a Likert-type scale ranging from 0 to 3, and the total score ranges from 0 to 63. A higher total score indicates greater depressive symptoms. Accepted cut-off scores are as follows: 10–18 = mild, 19–29 = moderate, and 30–63 = severe depressive symptoms. 25 It has been used in several studies with IBD patients8,26–28
State-Trait Anxiety Inventory (STAI): A commonly used self-report questionnaire that assesses the presence and severity of current (i.e. state) and general (i.e. trait) anxiety. 29 The STAI consists of 40 questions, divided equally between the state and trait subscales, and the total score ranges from 20 to 80. A score of 40 or higher has been identified as the threshold to identify clinically significant symptoms of anxiety. 30 This questionnaire has also been used in several studies with IBD patients.31–33
Data analysis
SPSS 26.0 for windows was used for the statistical analysis of the data. Categorical data were expressed as numbers and percentages, whereas qualitative data as median ± interquartile range (IQR). To evaluate the psychometric properties of the HADS, the internal consistency of the scale was calculated with Cronbach’s alpha coefficient and concurrent validity was assessed by Spearman correlation between the HADS, the BDI, and the STAI. T scores were used to assess group differences in depression and anxiety. Z scores were calculated for the comparison between proportions of positive scores in anxiety (STAI vs HADS-A) and depression (BDI vsHADS-D), for the evaluation of the current recommended cut-off score.
Results
Overall, 79 participants took part in the study. The background characteristics are detailed in Table 1.
Demographic characteristics (N = 79).

SD, standard deviation; TNF-α, tumor necrosis factor-α.
The internal consistency of the HADS was measured by Cronbach’s alpha coefficient and has been found to be 0.88 for the anxiety subscale, and 0.73 for the depression subscale, indicating a satisfactory reliability.
Median HADS scores were 10 ± 12 (ranged from 0 to 28) for the total score, 8 ± 8 (ranged from 0 to 18( for the HADS-A, and 3 ± 5 (ranged from 0 to 13) for HADS-D. Based on the accepted HADS cut-off scores, 39 (49.4%) of the participants scored below threshold (i.e. not anxious), whereas 40 (50.6%) scored above threshold, suggesting some degree of anxiety: 16 (20.3%) were possibly anxious, and 24 (30.4%) were in the probably anxious range. For the HADS-D, 68 (86.1%) scored as nondepressed, 10 (12.7%) as possibly depressed, and 1 (1.3%) as probably depressed.
The median STAI score for state anxiety was 38 ± 20 (ranged from 20 to 66), with 45 (57%) in the nonanxious ranges, and 34 (43%) were classified as anxious. The STAI score for trait anxiety was 38 ± 17 (ranged from 34 to 61), with 43 (54.4%) in the nonanxious range and 36 (45.6%) were classified in the anxiety group.
The median BDI score for depression was 7 ± 10 (ranged from 0 to 26). According to the recommended BDI cut-off, 48 (60.8%) were classified as nondepressed, 24 (30.4%) as mildly depressed, and 7 (8.9%) as moderately depressed. No participant scored in the severe depression range.
To assess the differences in the prevalence of anxiety and depression, we conducted a Z test. Higher prevalence of depression was obtained with the BDI compared with the HADS-D (Z = 3.59, p < 0.01). There was no significant difference between STAI and HADS-A in the prevalence of anxiety (Z = 1.30, p = 0.2).
To examine the correlation between the HADS subscales and the BDI and STAI, we conducted three Spearman correlation tests; results of the correlation between HADS-D and BDI score indicated a significant correlation (rs(76) = .69, p < 0.001). The correlations between HADS-A and both STAI subscale independently were significant (rs(76) = .853, p < 0.001; rs(76) = .744, p < .001, for state and trait anxiety, respectively) (Figures 1 and 2).
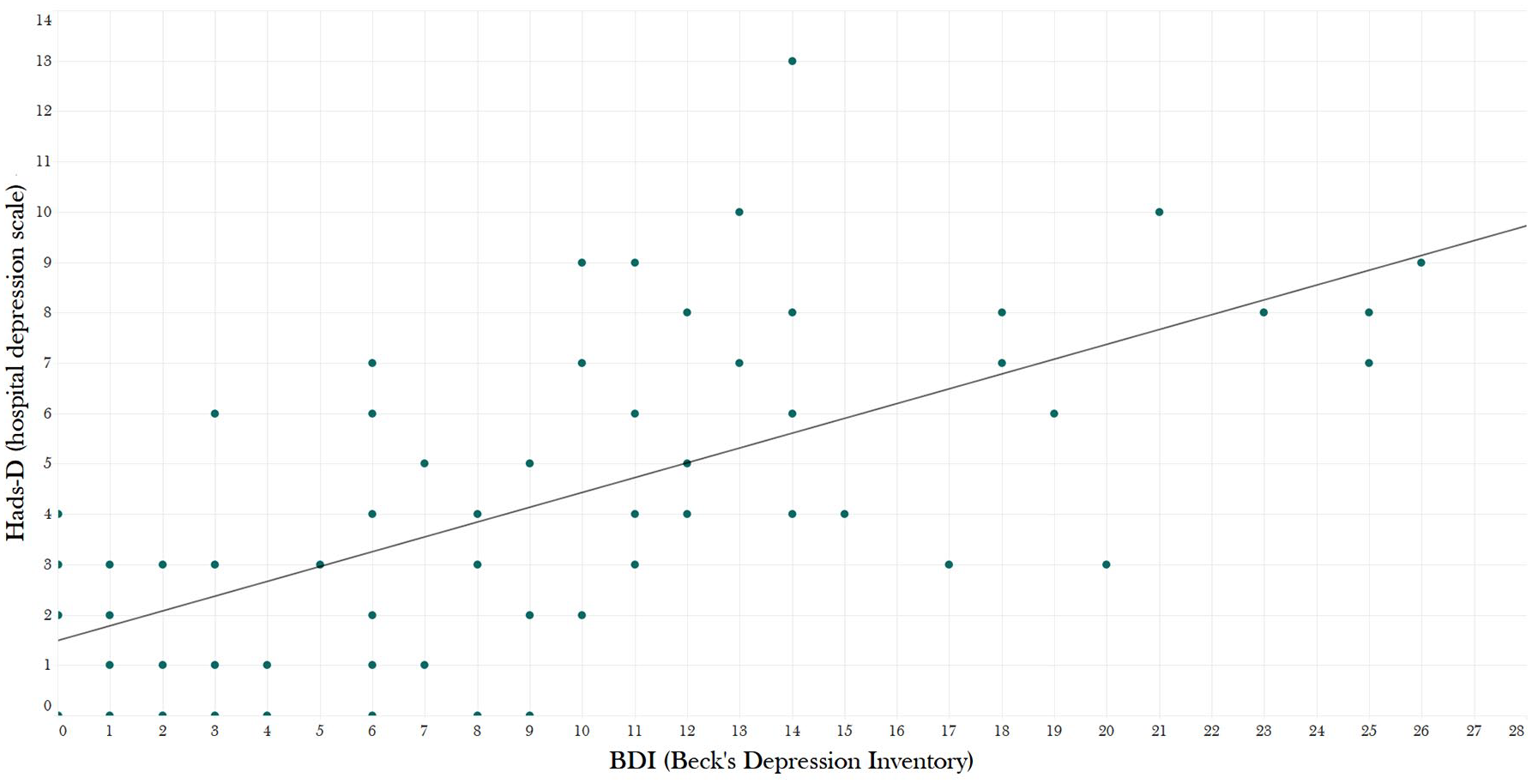
Correlation between HADS-D and BDI.
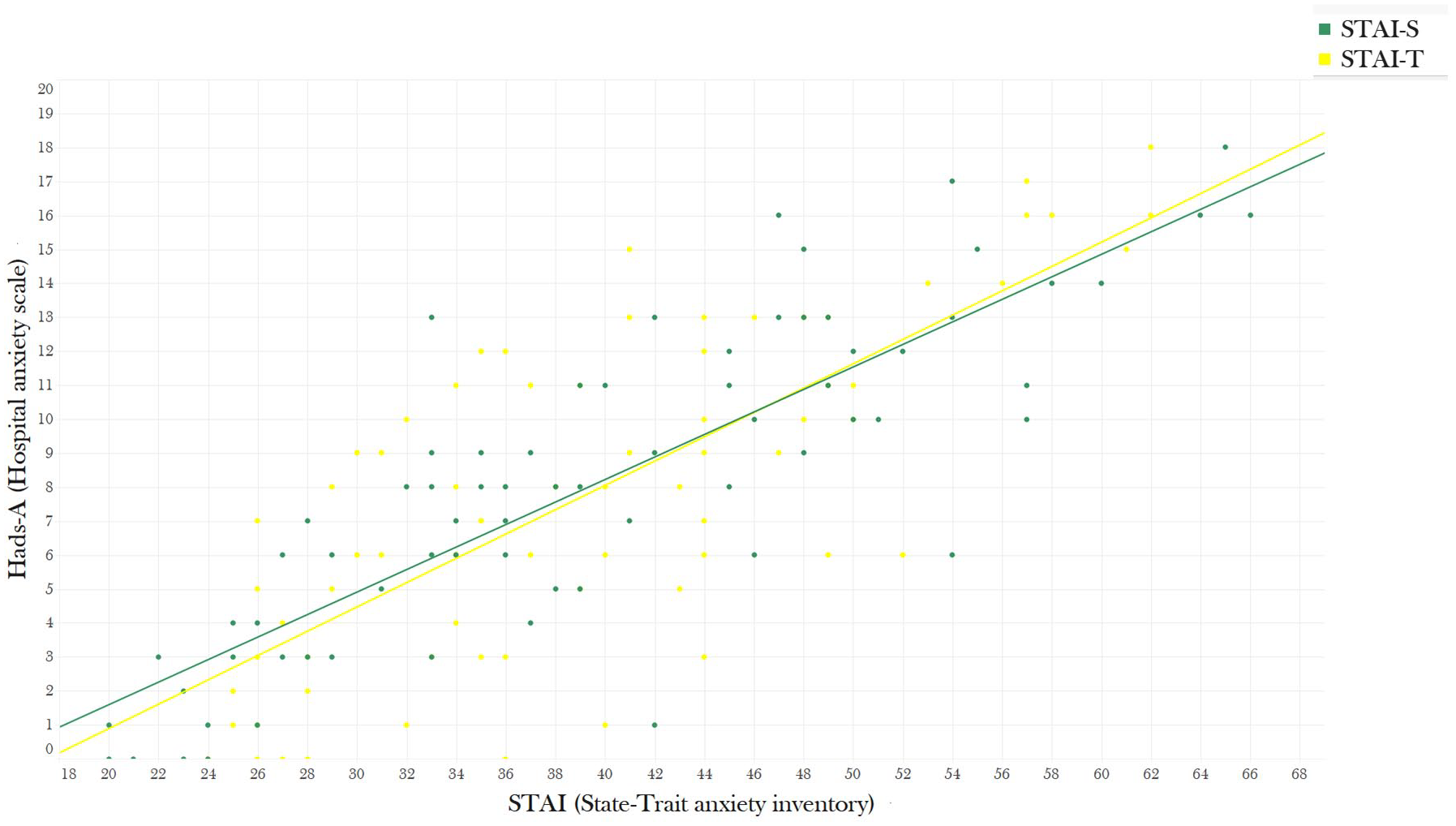
Correlation between HADS-A and STAI.
Anxiety and depression scores compared by gender, medication type, disease type, and disease activity are presented in Table 2.
Group differences in anxiety and depression scores (N = 79).

HADS-A, Hospital Anxiety and Depression Scale – anxiety; HADS-D, Hospital Anxiety and Depression Scale – depression; SD, standard deviation; TNF-α, tumor necrosis factor-α.
Discussion
The aim of this study was to examine the utility of the HADS questionnaire as a screening tool for depression and anxiety in Israeli IBD patients. We correlated HADS scores of 79 IBD patients with two well-accepted depression and anxiety scales – BDI and STAI, and found significant and strong correlations between them, indicating that HADS is a valid screening tool. Yet, we found some differences between the questionnaires in the prevalence of depression that should be considered, as the BDI showed higher prevalence of depression. A possible explanation of this discrepancy may derive from the reference to the physical symptoms in the BDI. Another possible explanation derives from the interpretation of the total scores of the different questionnaires: while the BDI has four levels of severity (no depression, mild, moderate, and severe), the HADS-D has three levels of severity (no depression, possible, and probable). These differences present one of the faults of using a questionnaire – the continuous score is sensitive to subjective manipulation, in the form of the categories of severity. Indeed, according to the BDI, 30% of the participants in our sample had a scored compatible with ‘mild depression’, which has no representation in the HADS-D categories.
Applying questionnaires in a clinical practice requires the user to decide whether it is more important to prevent false-positive or false-negative results. We believe that this balance is especially important to enable the use of HADS by GIs, to refer patients on a routine basis to a mental health professional for evaluation. A recent meta-analysis of 77 studies explored the prevalence of anxiety and depressive symptoms among IBD patients and revealed that nearly 32% of patients had symptoms of anxiety and 25% had symptoms of depression. 34 While in our study the rates of significant anxiety were similar between the HADS-A (using the higher ‘probably’ anxious cut-off) and STAI, previous studies, and the cohort’s BDI scores, imply that the HADS under-detected depressive symptoms.
Little is known about HADS validity among IBD patients, and we are familiar with only two studies on the subject. The first established the psychometric properties of the HADS by factor analysis. 18 In a second extensive study, Bernstein et al. compared sensitivity and specificity of different questionnaires completed by IBD patients, included the HADS, with a semi-structured clinical interview. They found that for a cut-off score of 11, HADS-D had the highest specificity, but relative low sensitivity. Therefore, the authors recommended a lower cut-off of 7 for the HADS-D to improve its sensitivity. 19 Our findings are in line with this recommendation, as we found lower than expected rates of depression using the HADS. As opposed to the depression scale, our findings regarding HADS-A are consistent with previous findings and STAI rates of anxiety. It was also compatible with the authors’ original cut-off recommendation (i.e. 8 or above for ‘possible case’, and 11 or above for ‘probable case’).
Given these findings, we recommend using different cut-off scores for each subscale: 7 or above for the diagnosis of concomitant depression with IBD, and 11 or greater for concomitant anxiety with IBD.
Our study has several limitations. First, as we had a relatively small sample size, the generalizability of our findings may be affected. Second, we assessed the validity of the HADS by comparing its score to two other self-report screening tools rather than to a robust psychiatric evaluation. This might yield false-positive or false-negative results due to a reporting bias of the participants. Third, our sample included only patients who were treated at the day unit of our department; as visiting the day treatment unit involves regular visits to the hospital, continuing interaction with an IBD nurse, encounter with other IBD patients, and receiving medication by infusion, it could affect our sample by acting as a sort of a therapeutic setting, making it more homogeneous than a general sample of individuals with IBD. Finally, it is important to note that even though BDI and STAI are well-accepted questionnaires to assess anxiety and depression in mental health circuits and were used by several studies with IBD patients,8,26–28,31–33 both questionnaires were not validated among IBD patients.
In conclusion, depression and anxiety are common among IBD patients. These conditions do not only cause substantial mental pain but also worsen prognosis. Therefore, mental health screening should be a part of the routine in gastroenterology follow-ups. Although comprising only 14 questions, we found the HADS questionnaire to be valid and highly correlated with other ‘gold standard’ self-report scales that are 4 times as long. Short and accurate, we recommend using the HADS routinely. A patient’s score of 7 or above in the depression subscale and 11 or greater in anxiety subscale should raise the possibility of a referral to a mental health professional for evaluation.
Footnotes
Author contributions
Asia Avinir was responsible for participant rectuiement, data analysis and manuscript preparation. Shira Dar and Ola Haj contributed in data collection and anlysis. Michal Taler, Doron Gothelf, Uri Kopylov and Shomron Ben-Horin contributed in the study’s design, interpretation and the data and critical revision of the final manuscript. Ehud Mekori-Domachevsky contributed in study concepualization. data interpretation and final apporval of the manuscript.
Authors’ note
This study establishes the utility of the Hospital Depression and Anxiety Scale (HADS) as a screening tool for IBD patients, by concurrent validity, as part of the routine in gastroenterology follow-ups.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.