
Abstract
Background:
Burnout remains a significant health concern within the healthcare sector. Numerous studies have explored burnout among gastroenterologists. However, as far as we are aware, there is currently no documented research specifically focused on burnout for specialists in the field of inflammatory bowel disease (IBD).
Objective:
The aim of our study was to assess the extent of burnout, its determinants, and to analyze potential risk factors among European healthcare professionals who provide care to patients with IBD.
Methods:
We carried out a cross-sectional pilot study involving healthcare professionals responsible for the treatment of patients with IBD. A total of 102 participants (56.9% male, average age 48 ± 10.6) completed the anonymous multiple question open web survey. The survey consisted of four distinct psychological constructs (burnout, depression, somatization, and well-being), along with inquiries associated with sociodemographic, health-related, and work-related factors.
Results:
In our study, we observed that 47.1% of professionals specializing in IBD experienced burnout. When considering all three factors of burnout simultaneously, 5.9% of participants fell within the moderate range. Among these, depersonalization (DP) was the most prevalent factor, with 48% at a medium level and 47.1% at a high level. Depression, somatization, and well-being correlated with emotional exhaustion (EE) and DP, while only depression correlated with personal accomplishment (PA). Furthermore, age, physical activity, total time spent in healthcare, and time spent as an IBD specialist were correlated with EE. Multiple linear regression analysis revealed that depression was the most dominant predictor of both PA and DP. In terms of work-related factors, we observed that having endoscopic access had a detrimental impact on burnout, while the presence of a dedicated IBD outpatient unit and opportunities to participate in multidisciplinary meetings had a positive effect on mitigating burnout.
Conclusions:
Our pilot study underscores the importance of burnout among IBD professionals in Europe, with a specific emphasis on DP. Subsequent studies may help to uncover the way underlying factors contribute to burnout, potentially laying the foundation for international support and prevention initiative programs.
Plain language summary
Professionals working with IBD patients are at high risk of burnout. The prevalence of depersonalization is the highest and there are several other risk factors. However, we also found protective factors that may help to reduce and prevent burnout.
Keywords
Introduction
Burnout is a complex process, which can be understood as a response to prolonged stressors, and has three main dimensions: emotional exhaustion (EE), depersonalization (DP), and reduced personal accomplishment (PA). 1 DP in social relationships is associated with feelings of distance, dehumanization, and desensitization. EE is characterized by loss of empathy and emotional and physical fatigue. Moreover, in the case of reduced personal performance, a negative evaluation of oneself commonly is present, particularly in terms of the work done with patients.1 –3 According to Maslach, burnout may impair the care and professional attention that human service providers give to their clients. Burnout is a major health problem among doctors and nurses. 2 In general, symptoms of burnout include fatigue, sleeping disorders, psychosomatic symptoms, maladaptive coping, reduced interest, cynicism, indifferent behavior, hopelessness, increased depression and anxiety levels, suicidal ideation, social connections alteration, reduced PA, and an increased number of sick leave days. The effects of these symptoms may burden the healthcare system and cause several personal and financial problems for the individuals (both patients and doctors) and the healthcare system as a whole.3,4 It has been established that burnout affects the physicians’ well-being, organizational effectiveness, and ability to provide quality care. Burnout thus plays a significant role in the overall quality of the universal healthcare system. 4
Healthcare professionals are at daily risk of exposure to different stressors that lead to burnout. Burnout occurs in approximately 30–65% of the physicians, particularly in those working in the fields of emergency medicine, critical care, and general internal medicine.3,5,6 The rate of burnout in gastroenterologists has been reported to be between 18.3 and 64.4%; in addition, 32–63% of gastroenterologist respondents recorded moderate to high levels of EE.7,8 Both professional and personal factors may contribute to the degree of burnout experienced among professionals. Burnout was demonstrated to be the highest in females, those with a younger age, and those having no children or having young children. Work–life imbalance also affects burnout.4,8,9 For example, time spent on work-related activities in the home environment can increase burnout. 8 But other inequalities, family roles, and the relegation of tasks in a home environment can also have an impact on burnout.4,9 A study on English gastroenterology trainees reported a burnout prevalence of 35.3%, and more than 57% of these trainees reported EE, 63.9% low performance, and 23.5% of them showed signs of DP. 10 However, the results are varied and often contradictory concerning the extent of burnout amongst professionals. One thing that might be clear is that a significant proportion of gastroenterologists struggle with symptoms of burnout throughout their career. Currently, no specific data are available in regard to the mental health of inflammatory bowel diseases (IBD) specialists. European Crohn’s and Colitis Organization (ECCO) is an organization that includes experts and doctors in the field of IBD and is therefore dedicated specifically to IBD patients. It is assumed that ECCO members are made up of gastroenterologists who have an outstanding interest in IBD. They research and practice in a field that enables them to interact with people affected by IBD on a daily basis; therefore, influencing them to choose ECCO membership as a personal interest area of focus. It would be compelling to study whether long-lasting management and care of this special group of patients has an influence on the physician’s emotions and whether it leads them to experience a higher incidence of burnout than with other subspecialties.
Therefore, the purpose of the study was to measure the level of burnout in European gastroenterologists treating IBD patients by using various types of questionnaires and analyzing social and economic risk factors.
Materials and methods
Study design and participants
The current study was an international, observational, cross-sectional, questionnaire-based pilot study, supported and authorized by the ECCO carried out between April 2021 and October 2021. The idea of the study was presented at the 5th IBD National Study Group Virtual Meeting and was found worthy of implementation. The clinical study protocol and the study synopsis were created with the help of the Clinical Research Committee of ECCO. Ethics approval number: RKEB 197/2020-SZTE. Participants were contacted via e-mail, and participation was voluntary. An anonymous multiple question open web survey was conducted with the logistical support of the ECCO (the questionnaire we compiled was published in the organization’s official newsletter). [The reporting of this study conforms to the Checklist for Reporting Results of Internet E-Surveys statement (Supplemental Material 1)]. 11 ECCO members were invited to participate in this survey through collective e-mails. All subscribed members received the newsletter, but the questionnaire was addressed to practicing physicians who are IBD specialists. In total, 9521 recipients received the newsletter. Considering the statistics of the congress (2200 gastroenterologists out of 6800 participants), it was estimated that about half of the members who received the newsletter are gastroenterologists, and about half of them opened the questionnaire. 12 Due to the low response rate, invitations were subsequently sent to our previous study partners (100 additional people). The previous research partners were professionals who also had a high proportion of IBD patients, and their research work was focused on this field of study. Additionally, they had previously collaborated with the authors of this article on joint international studies in this particular field of research. Thus, they were directly contacted to complete the questionnaire. This suggests an estimated response rate of 4–5% among IBD specialists.
Participants gave informed consent prior to filling in the questionnaire. Additionally, they acknowledged their consent for data processing and the potential publication of information obtained from the aggregated data. The questionnaire started with information about the purpose of the survey and how to complete the questionnaire. No personal information was stored during the completion of the questionnaire, only the answers were saved. Filling in the questionnaire could be discontinued at any time without any consequences. There were no rewards or incentives for responding. The answers were stored and processed in accordance with data protection rules. In addition to this, the inform consent and details were contained within the text of the emailed newsletter. The initial questionnaire was first tested among our own colleagues before being publicly released. After creating the questionnaire, the first version was tested among our own colleagues (eight specialists and residents in total) who work in the field of gastroenterology and frequently treat patients with IBD in inpatient or outpatient settings. We developed the final version of the questionnaire with careful consideration of their personal feedback and suggestions. The questionnaire consisted of four well-known, widely used indexes/scales to measure the psychological condition of respondents as well as some multiple-choice questions on sociodemographic data. The number of items varied between 16 and 22 per page. The full questionnaire was five pages long. All questions were compulsory with the exception clause for each. For example: ‘Do you have any known chronic disease? Yes or No. If yes – Which one?’ – that was optional. In this way, the completeness of each response could be checked. Only the completed questionnaires were analyzed and included in the database. The respondents were categorized according to the number of regularly managed IBD outpatients per week: small IBD centers (1–500 patients), medium centers (501–1000 patients), large centers (1001–2000 patients), and extra-large centers (over 2000 patients). The quality of the responding centers was ascertained by targeted questions: the existence of regular multidisciplinary meetings, the number of IBD nurses, the existence of dedicated IBD outpatient units, the possibility to administer biological drugs, and finally, access to the endoscopy unit.
The questionnaire was only available in English and took about 20 min to complete. The sample included all gastroenterologists who were ECCO members and subscribed to the newsletter and completed the questionnaire, as well as research partners in the field who also completed the questionnaire. Completion was by convenience sampling and a snowball method. No other professionals were included in the study. The questionnaire was divided into four sections. In the first part of the study, sociodemographic data was collected, such as age, gender, leisure activities, and spiritual beliefs. The second section gathered information about the physical health of the participants including chronic diseases, body mass index (BMI), list of regular medications, and smoking and drinking habits. The third part of this study focused on information related to work and collected comprising data on the workplace, time spent in healthcare, number of work hours, and scientific activities. The final component of this study recorded four psychological measures: Maslach Burnout Inventory (MBI), Patient Health Questionnaire-9 (PHQ-9), Patient Health Questionnaire-15 (PHQ-15), and World Health Organization 5-item well-being questionnaire (WHO-5).13 –19
Measures
MBI is a widely used measure to assess burnout. It covers three different domains of burnout: EE, DP, and PA. Higher EE and DP scores in combination with lower PA scores result in higher burnout levels. Scores for all three factors are categorized as low, moderate, and high. PA scores are inversely interpreted to EE and DP. The combination of high categories in all three subscales (DP, EE, and PA) indicates burnout.13,14 However, some authors define burnout as having high EE and/or DP scores.8,20 This was also used to determine the degree of burnout. Generally, the inventory is considered highly reliable (Cronbach’s α = 0.795). 13 In our own study, Cronbach’s α was 0.874.
PHQ-9 is a self-administered questionnaire that is useful to screen the severity of depression (Cronbach’s α = 0.848). The clinical cut-off is 10, and it strongly predicts the likelihood of depression. 15 Our PHQ-9 results showed that Cronbach’s α was 0.850.
PHQ-15 is a self-administered questionnaire that may be useful in screening for somatization and the severity of somatic symptoms (Cronbach’s α = 0.784). The cut-off score is 10 or above.16,17 Our reliability analysis result was Cronbach’s α = 0.782.
WHO-5 is a self-reported measure of current mental well-being with high reliability (Cronbach’s α = 0.927). The raw scores range from 0 to 25. A score of 0 represents the worst quality of life and 25 the best quality of life.18,19 Our reliability analysis result was Cronbach’s α = 0.925.
Statistical analyses
Statistical tests were performed by using Jamovi software Version 2.2.2 (The Jamovi project (2021), 21 with p < 0.05 considered statistically significant. In addition to descriptive statistical analysis, Pearson correlations, independent sample t-test, Mann–Whitney test, and linear regression analysis were performed on the data. Pearson correlations were performed with continuous variables (e.g. total questionnaire scores, age, number of children, number of leisure activities, number of regular medications, on-call duty, years at work, number of patients cared for, etc.). Additionally, dichotomous variables were included or transformed for ease of analyzing the data. In the correlation analyses, one participant was excluded based on the number of IBD nurses in their institution (average 2.15 ± 1.68) as they reported 52 IBD nurses, which is an outlier when compared to the others. This report of having 52 nurses is more than 3 standard deviations from the average and is not as realistic as the value 6, which was the maximum value in the remaining data. All participants were included in the sample when comparing groups. Gender differences were assessed in the four questionnaires (separated by MBI subscales). In each group, depending on whether the normal distribution was found, Mann–Whitney (PA, EE, depression, and somatization) or independent samples t-tests (DP and well-being) were performed Multiple linear regression analyses were used to further investigate the factors explaining burnout. In addition to the psychological scales, variables that correlated with the burnout subscales (PA, DP, and EE) were included, as well as five additional dichotomous variables (multidisciplinary meetings, number of IBD patients managed by the center, existence of dedicated IBD outpatient unit, possibility to use biological drugs, and access to endoscopy unit). In case of dichotomous variables, the yes–no answer was the default (multidisciplinary meetings, existence of dedicated IBD outpatient unit, access to endoscopy unit) or recoded the response options into two categories (number of IBD patients managed by the center (above 1000 patients = 1, below 0), possibility to use biological drugs (not available = 0, available = 1). The Jamovi program uses Enter method for the regression analysis.
Results
Baseline characteristics
A hundred and two professionals completed the pilot questionnaire (male 56.9%). The response rate was quite low (about 5%). The average age was 48 ± 10.6 years, the youngest healthcare professional was 31 years old, and the oldest was 85 years old. Sociodemographic, health, and work-related factors are summarized in Table 1.
Sociodemographic, health, and work-related factors.

IBD, inflammatory bowel disease.
Based on our study findings, it is characteristic of the general IBD specialist to live in a relationship, work mostly in a city hospital, and largely associated with a university environment. They have 22 or more days off per year and have sufficient financial savings. They are non-smoker, but occasionally consume alcohol, and rate their own current health status as mostly good. They are also active in conducting scientific research, regularly attend multidisciplinary meetings, have a dedicated IBD outpatient unit, and have access to biological therapy. They have been working as an IBD specialist for an average of 14 years, work 12 h/day, have two to three on-calls per week, attend 55 IBD patients, and perform 19 endoscopies per week. Their work is supported by two IBD nurses working at the center.
In terms of the questionnaires examined, 12.7% of the participants scored above 10 on the depression questionnaire, which is already an indication of the presence of a clinical level disorder. 0.9% of the respondents reported a medium or high score on the somatization symptoms scale. On general well-being, 43% of the respondents scored below 14 points, with the majority reporting a medium or high perceived quality of life.
Level of burnout
For all three factors of burnout combined, 5.9% (n = 6) of participants fell within the moderate range. There were none who scored in the worst range in all three burnout categories. However, 47.1% of the respondents (n = 48) were in the highest category in terms of DP, which in this case also provides an indicator of burnout.8,20 Among those with high DP, 43.8% (n = 21) reported a moderate decrease in PA and 8.3% (n = 4) had a moderate level of EE. One-third of the respondents had a moderate decrease in PA, with less than 10% of these having EE. However, nearly half of the doctors experienced DP symptoms to a moderate degree, whereas the other half experienced DP symptoms to a high degree. Descriptive statistics of burnout subscales are summarized in Table 2, and frequencies of burnout category results are demonstrated in Table 3.
Descriptive statistics of MBI subscales.
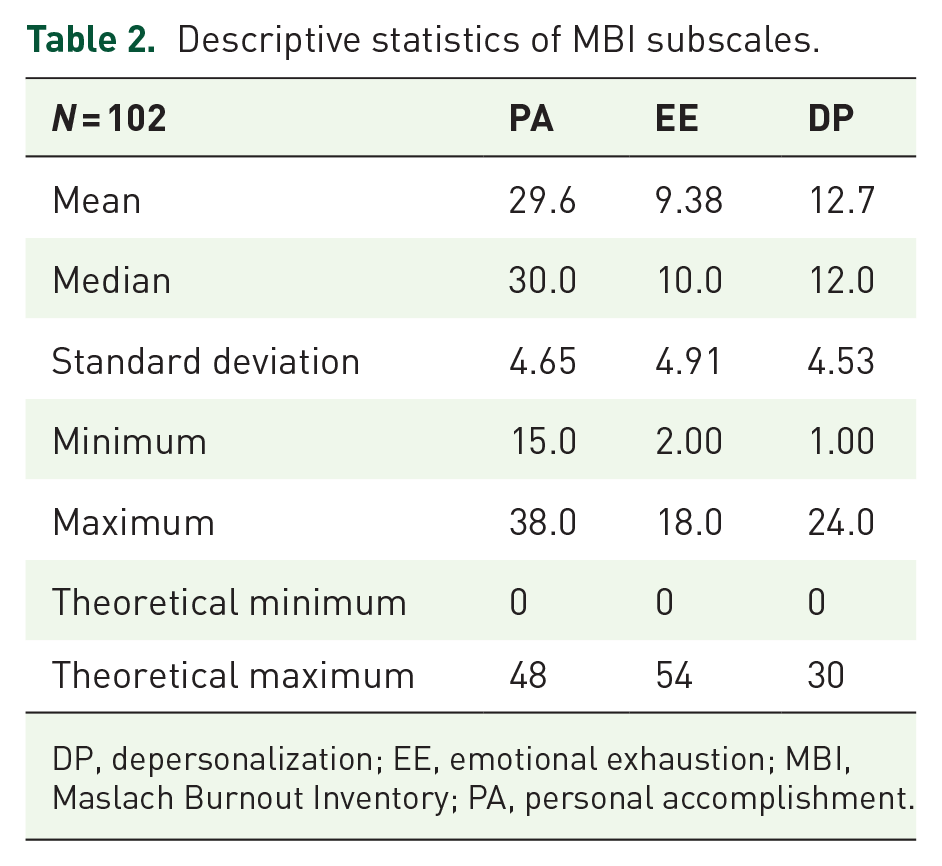
DP, depersonalization; EE, emotional exhaustion; MBI, Maslach Burnout Inventory; PA, personal accomplishment.
Frequencies of burnout categories (N = 102).
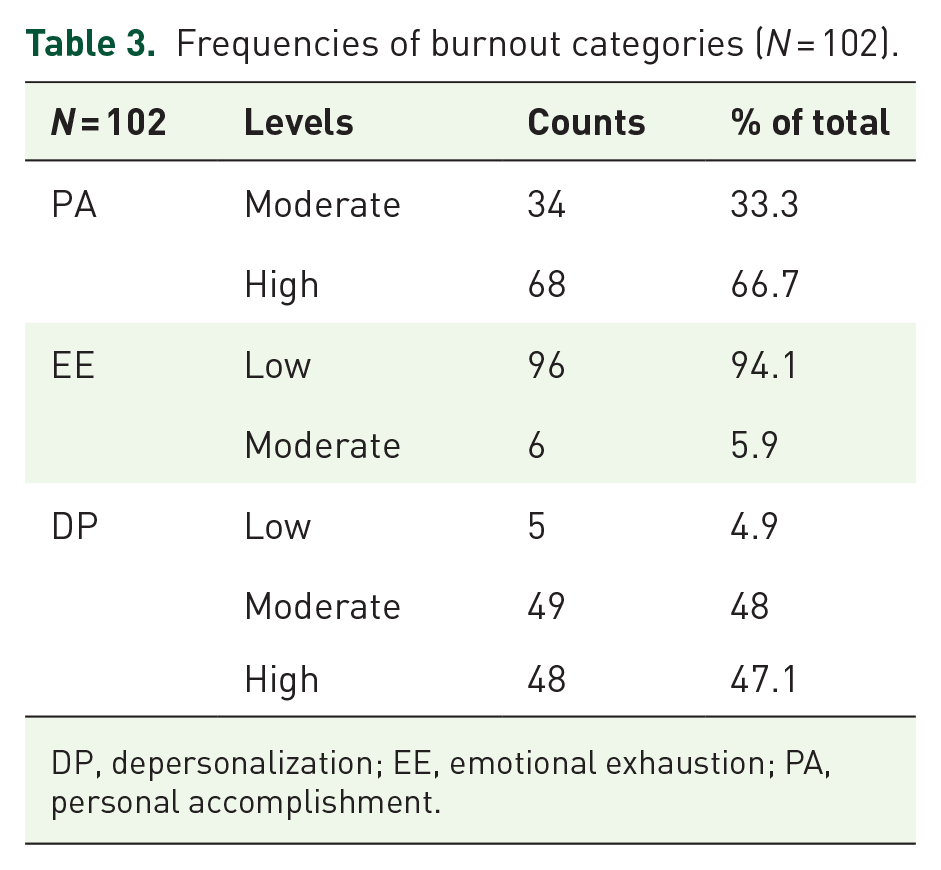
DP, depersonalization; EE, emotional exhaustion; PA, personal accomplishment.
Factors associated with burnout
Correlations were used to examine which variables were associated with the degree of burnout. The burnout questionnaire was assessed on three subscales: PA, EE, and DP. The three subscales were compared with the following continuous variables: age, number of leisure activities, children, regular medications, exercise, BMI, time spent in healthcare, time spent as IBD specialist, managed IBD patients, on-call duties, work hours, number of endoscopies, number of IBD nurses, and collective sum of the psychological questionnaires. Seven different variables (age, exercise, time spent in health care, and time spent as an IBD professional depression, somatization, and well-being) show low or moderate correlation with one or more burnout subscales. Moderately strong correlations were found for all three psychological factors with EE, and depression with DP. The results are summarized in Table 4, and all other non-significant correlations are presented in the Supplemental Table (Supplemental Material 2).
Variables significantly correlated with burnout subscales.

Significant correlations (p < 0.05) are highlighted.
DP, depersonalization; EE, emotional exhaustion; PA, personal accomplishment.
Factors explaining burnout
The regression model explaining the PA was significant: R2 = 0.161;
Regression model of factors explaining PA.

The main explanatory factors are highlighted.
IBD, inflammatory bowel disease; PA, personal accomplishment; VIF, variance inflation factor.
Results of the regression analysis of EE were R2 = 0.518;
Regression model of factors explaining EE.
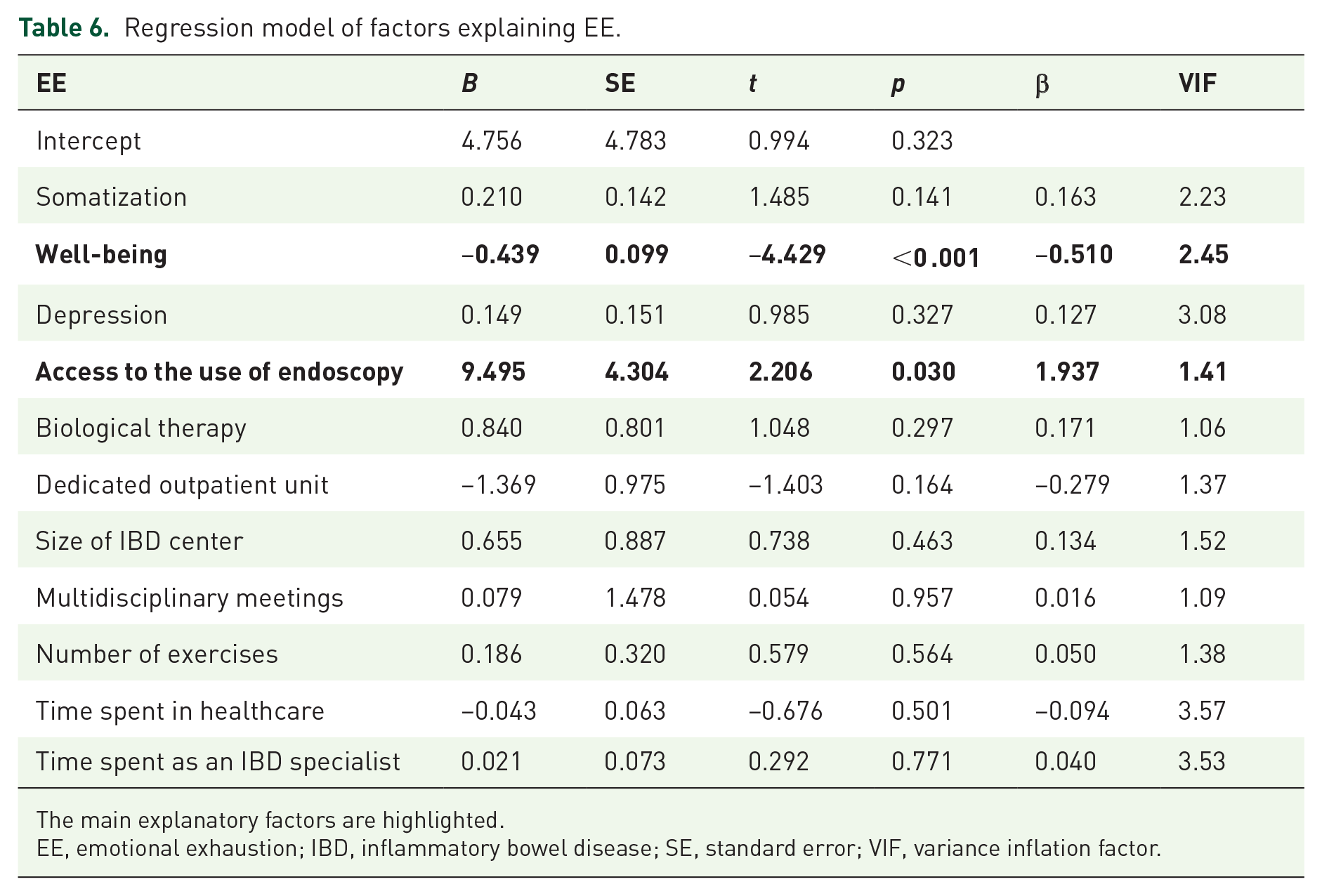
The main explanatory factors are highlighted.
EE, emotional exhaustion; IBD, inflammatory bowel disease; SE, standard error; VIF, variance inflation factor.
Results of the regression analysis of DP were R2 = 0.263;
Regression model of factors explaining DP.

The main explanatory factors are highlighted.
DP, depersonalization; IBD, inflammatory bowel disease; SE, standard error; VIF, variance inflation factor.
Gender differences
Gender differences were assessed in the various questionnaires. In each group, depending on whether the normal distribution was found, Mann–Whitney or independent samples t-tests were performed. The results of the tests are shown in Table 7. There was no significant difference between male and female specialists in DP [t(100) = −1.35, p = 0.179]. Men had significantly higher well-being scores compared to women [t(100) = 2.74, p = 0.007]. There was no significant difference between the two genders in regard to EE and PA. However, there was a significant difference between the two groups in the prevalence of depressive symptoms (p < 0.001) and somatization symptoms (p < 0.001). Women scored significantly higher (almost double) than men on these variables for both depression and physical symptoms (Table 8).
Mann–Whitney and t-test results and descriptive statistics of gender differences.

df = 100.
Significant variables are highlighted.
DP, depersonalization; SD, standard deviation; WHO, World Health Organization.
Discussion
The aim of the pilot study was to measure the level of burnout and analyze social and economic risk factors among European IBD specialists. Previous studies have assessed the incidence of burnout in larger groups, but no similar study has been conducted specifically among IBD professionals. A total of 102 participants took part in the survey. Our study results are the first to measure the mental status of a specialized healthcare professional group from various European countries, and the results might be beneficial in determining the needs for intervention on an organizational level.
First and foremost, our study revealed that 47.1% of the IBD professionals experienced burnout. Compared to previous studies, burnout rates were generally higher, which may suggest there might be an increasing risk associated with this target group.4,10,22 We found that factors predisposing to burnout include depression, reduced subjective well-being, somatization, and access to the use of endoscopy. Contrary to these, we identified access to outpatient care and multidisciplinary meetings as protective factors. In our study, out of the various burnout factors, DP rates were the highest among IBD specialists. According to a German study, 33% of German gastroenterologists had a high DP score, 17% had a high EE score, and about 50% had a low PA score. 23
There was a moderately strong positive correlation for depression and somatization with both EE and DP, and a moderately negative correlation between well-being and EE. Depression was correlated with all three burnout subscales. Several previous studies have found a medium-to-high correlation between depression and burnout, and our pilot study was consistent with them.24,25 In addition to correlation, an association was also found between burnout and depression. 26 British researchers have investigated the correlation between well-being and burnout among doctors. They have found a medium negative correlation between the two factors. 27 In addition, younger age, regular exercise, and time spent in holistic medicine and as an IBD specialist are also negatively correlated with EE, but it has not been reported in the explanatory model. Young age seems to be a risk factor that is frequently identified in burnout studies.3,4
Higher levels of EE have been measured, which might lead to cynicism and somatization, and thus, have a negative impact on personal effectiveness. 28 A meta-analysis has found that outpatient doctors experience higher levels of EE than their inpatient colleagues. 29 This finding may contradict ours. In our case, outpatient care was a protective factor. Depression was found to be the strongest explanatory factor behind the decline in both PA and DP. Similarly, a representative survey of Austrian physicians have assumed that major depression is strongly associated with all the three subscales of burnout. 30 A link between work-related burnout and depression has also been identified in young doctors. 31 Moreover, access to the use of endoscopy appeared to have significant effects on EE and a tendency in case of DP. Irrefutably, endoscopic work with IBD patients can be a source of increased stress for professionals. The increasing complexity of endoscopic techniques combined with an increased risk of complications and less professional experience may lead to higher burnout rates.22,32
In a significant number of studies on gastroenterologists, workload-related factors, age, and female gender were the three most frequently cited risk factors.7,33,34 We found no significant effect of gender and age on burnout, but work-related factors, such as access to the use of endoscopy, outpatient unit, and multidisciplinary meetings (as a trend) seemed to have an impact on burnout. The results suggest that stress and the difficulty of endoscopic work are reflected in the degree of burnout among doctors; the greater the workload in this particular area of the profession, the greater the degree of burnout. It is a welcome conclusion that those working in this specific field are also accompanied by protective factors. Outpatient care is perhaps one of the scenes where they can achieve improved patient well-being, a sense of success through helping them and a higher level of satisfaction. The professional environment that a multidisciplinary team can provide may reduce the strain on professionals through development and shared responsibility, as well as collaborative problem solving and perspective switching.
When compared with the opposite sex, women reported higher somatization and depression scores, while men reported higher subjective well-being values. Gender differences were present in these factors, but no gender differences were found for burnout. Men’s higher well-being values may be due to different social roles and expectations; as a matter of fact, men may feel less need to talk about their difficulties, and the working environment may view these attempts less seriously. Women are more likely to experience and express depressive symptoms, and those with depression that are affected by valence are more at risk of DP. Screening for this factor can also provide useful data on burnout, especially for female professionals. On the other hand, women also reported more somatic symptoms when compared to men. Although there was a strong correlation between depression, anxiety, and somatization, it was independent of gender and age. 35 To our knowledge, no studies have examined gender differences in depression and somatization among gastroenterologists.
A major factor in managing burnout is establishing and maintaining a work–life balance. In terms of prevention, personal and institutional level interventions are important. Problem-focused coping and the exploration of resources as individual factors can be supportive to increase well-being. Organizational-level strategies can focus on supporting professional development, reducing work-related stress, and supporting and mentoring colleagues.34–36 Participation in professional societies, research activities, and education can also help manage burnout. 3
The research had many limitations. Due to the low number of subjects, we could not draw conclusions for a wider population. Furthermore, the study questionnaire study did not allow us to qualitatively explore the attitudes of the participants. For many professionals, English is not considered as their mother tongue or primary language, subsequently for some questions, minor differences in the answers may not have been accurately reflected. In addition to the cross-sectional study, it would also be useful to use follow-up methods to investigate the state of burnout among doctors. Online completion and convenience sampling was also a drawback as we could only involve respondents indirectly with no opportunity for face-to-face contact. An additional limitation of this study is the fact that respondents may come from a range of countries that have differing health systems, which can ultimately mean large individual and organizational differences within and across countries. In addition to the structure of the healthcare system, other general and social differences and problems may also affect response preferences. In the future, we plan to carry out a more detailed, broader, comparative study on the subject.
According to this study, professionals who work with IBD patients, particularly within this group of gastroenterologists, also are at a high risk of experiencing burnout. In conclusion, the role of protective factors against burnout (access to outpatient care and multidisciplinary meetings) may have a positive effect and are mostly accessible in well-equipped clinical centers. In addition to the higher level of care and cost-effectiveness aspects that have been identified at these institutions, this finding also underlines the influenceable role these institutions have on promoting positive returns on the mental health of their doctors. However, further research is needed to explore these factors in more detail.
Supplemental Material
sj-docx-1-tag-10.1177_17562848231214086 – Supplemental material for Burnout among European IBD specialists: a survey supported by ECCO
Supplemental material, sj-docx-1-tag-10.1177_17562848231214086 for Burnout among European IBD specialists: a survey supported by ECCO by Anett Dávid, Márta Volosin, Klaudia Farkas, Tamás Resál, Csilla Keresztes, Beatrix Rafael and Tamás Molnár in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
We wish to thank the ECCO for supporting the release of our questionnaire and the IBD professionals who took the time to complete the forms. Thanks are also merited to all colleagues who contributed their personal help and support in making this study possible. Publication support was funded by Klebelsberg Library, University of Szeged.
Declaration
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.