
Abstract
The rapid emergence of inflammatory bowel disease (IBD) in Asia in the last two decades is anticipated to pose significant challenges to the healthcare systems of developing countries including India. Several epidemiological factors in the Asia Pacific region have been explored as risk factors for the development of IBD. In this narrative review, we discuss the evolution of adult-onset and paediatric IBD in South Asia and India, in relation to the current global epidemiology, over the last decade. The focus lies on the changing epidemiological landscape of IBD in Asia which signals a paradigm shift in the disease trajectory of a chronic, relapsing, complex disease. We enumerate the disease burden of IBD in India and Asia, analyse the risk factors for its recent rise in incidence and briefly discuss the unique entity of very early-onset IBD. We also list the locoregional challenges in diagnosis and management along with suggestions to overcome them. We highlight the lacunae in data which warrants further research. The anticipated infrastructural challenges and disease evolution are likely to be similar in most newly industrialized countries across South Asia. A combined effort led by IBD experts in the region to understand the true disease burden is important. A strong collaborative network on research and formulation of preventive strategies relevant to the region will help reduce the burden in the future.
Plain language summary
The rapid rise of Inflammatory bowel disease (IBD) in Asia in the last two decades is expected to pose significant challenges to healthcare systems of developing countries including India. Several risk factors have been investigated for the development of IBD in the Asia Pacific region. In this article, we discuss evolution of adult onset and childhood onset IBD in South Asia and India and compare it to the current global situation. We focus on the changing landscape of IBD in Asia which indicates a dramatic shift in the disease. We list the burden of IBD in India and Asia, analyse the risk factors for its recent rise, and briefly discuss the unique entity of IBD in infants and toddlers. We also list the challenges in diagnosis and management specific to the region, along with suggestions to overcome them. We highlight the gaps in data which need further research. We anticipate that the disease evolution and challenges are likely to be similar in most newly industrialised countries across South Asia. A combined effort led by IBD experts in the region will be necessary to understand the true burden of disease.
Introduction
Inflammatory bowel disease (IBD) is a complex, relapsing chronic inflammatory disease of the gastrointestinal tract. 1 IBD is broadly classified as ulcerative colitis (UC), Crohn’s disease (CD) and indeterminate colitis or IBD-unclassified (IBD-U). Although the pathophysiology of IBD is not clearly known, a complex interplay of autoimmune, genetic and environmental factors is hypothesized to contribute to the pathogenesis.1 –3
IBD has generally been recognized as a disease of the West because of higher disease prevalence in these regions. However, recent systematic reviews have reported a steady increase in the incidence of IBD across the globe, especially in emerging economies.1,4 This observation has substantial implications for the developing nations of Asia, Africa and South America, which already suffer from overburdened healthcare systems. This paradigm shift in epidemiological patterns of IBD could herald a new epidemic in countries with limited resources thus posing a challenge to clinicians and health policy makers. Diagnosis of IBD in newly industrialized countries which continue to experience a significant communicable disease burden remains challenging often resulting in diagnostic delays. Management of IBD has been transformed with the introduction of biologics and small molecules (Figure 1), resulting in significant improvement in the quality of life of people suffering from IBD. However, the lack of equitable access to these drugs remains a burning issue in parts of Asia, thus compounding the problem.

Treatment pyramid for inflammatory bowel disease.
At present, India is one of the fastest-growing large economies of the world 5 and stands at the cusp of experiencing a rapid rise in the incidence of IBD. In 2010, the total Indian population to be affected by IBD was estimated to be 1.4 million, which was the second-highest number after USA (with 1.64 million). 6 Although the disease prevalence in India is lower than in the West, it has one of the largest burdens of IBD patients in the world, mainly due to a large total population of 1.4 billion (as of January 2024). 7 Estimates based on available data predict a four-fold increase in the prevalence of IBD in India and a 1.6-fold rise in the prevalence of IBD in high-income Asia-Pacific and Southeast Asia regions by 2035. 8
In this review article, we summarize the published literature on the epidemiology of IBD including paediatric IBD (PIBD) in India and Asia over the last decade, evaluate causes for the rise in incidence, and unique considerations, and phenotypes in PIBD. We also list challenges in the diagnosis and management of IBD in this region and propose solutions to overcome them.
Epidemiology – disease burden of IBD across the world, Asia and India
Global burden of IBD
As per current data, the incidence of IBD in the Western world is estimated to be between 20 and 30 per 100,000 population.1,4 In 2017, there were 6.8 million cases of IBD globally. 9 As per the Global Burden of Disease (GBD), the highest age-standardized prevalence rate in 2017 occurred in high-income North America [422 (398.7–446.1) per 100,000] and the lowest age-standardized prevalence rates were observed in the Caribbean [6.7 (6.3–7.2) per 100,000 population]. 9
Burden of IBD in Asia
Asia has seen the biggest wave of industrialization in the last 20 years. Japan, China, India and countries in the Middle East are some of the fastest-growing economic regions of the world. This massive growth has led to a rapid emergence of IBD in the population.10,11 The Asia-Pacific Crohn’s and Colitis Epidemiology (ACCESS) study conducted in nine countries across Asia-Pacific in 2013 was the first large-scale population-based study in the region which reported incidence rates ranging from 0.54 to 3.44 per 100,000 people in Asia. 12 The incidence rate in Asia (per 100,000 people) was 0.76 for UC, 0.54 for CD and 0.07 for IBD-U. 12 In this study, the highest annual incidence of IBD was seen in highly urbanized areas like Guangzhou (mainland China) at 3.44 per 100,000, followed by Hong Kong at 3.06 per 100,000 and Macau at 2.2 per 100,000 persons. 12 There was significant variability in incidence within the same country and was likely related to the different degrees of urbanization and variable access to healthcare. 12 A prospective population-based study in 13 countries in Asia-Pacific by the same group between 2011 and 2013 found that India [9.31; 95% confidence interval (CI): 8.38–10.31] and China (3.64; 95% CI, 2.97–4.42) have the highest IBD incidence (per 100,000 persons) in Asia. 13 Also, of note, was the observation that not all newly industrialized countries experienced high incidence rates. Incidence rates in Singapore and Malaysia were much lower at 1.06 per 100,000 and 0.94 per 100,000 persons, respectively. 12 An epidemiological study of IBD in Malaysia which reported incidence based on race and ethnicity throws more light on this observation. In this study, the highest rate of incidence was seen in Indians (1.91 per 100,000 persons), followed by Chinese (0.63 per 100,000 persons) and Malays (0.35 per 100,000 persons) living in Malaysia. 14 This distinction in inter-racial incidence supports the hypothesis of the complex interplay between genetic and environmental factors that underlines the pathogenesis of IBD, thus explaining the heterogeneity in incidence across developed countries in Asia with multiple ethnicities. The age-standardized incidence of elderly onset IBD (onset >65 years of age) in Asia as per GBD 2019 was 3.52 (2.6–4.73)/100,000 in males and 2.92 (2.18–3.91)/100,000 in females with an annual percentage change (APC) of 0.75 and 0.66, respectively. 15 Data from India, Hong Kong and the Middle east on elderly IBD suggest a less severe phenotype, less use of immunomodulators and biologics, but higher rates of colorectal cancer and infections.16 –18
Time trends of UC and CD in Asia
Temporal trends in incidence and prevalence over the last decade from Asia are sparse. However, available data suggest increasing APC of both UC and CD. 11 Population-based data in Japan which has a national IBD registry shows a steep rise in recorded IBD cases from 1991 to 2015; a 9.5-fold increase in the prevalence of UC (18.1–172.9) and CD (5.9–55.6), per 100,000 persons was noted.19,20 A similar observation was noted in a population-based study from South Korea [Korean Association for the Study of Intestinal Diseases (KASID)] over two decades. It revealed a 10-fold increase in the incidence of UC (0.34–5 per 100,000 persons) and a staggering 72-fold increase in the incidence of CD (0.05–3.6 per 100,000 persons).21,22
The gap between the incidence of UC and CD is closing in Asia. A recent cross-sectional study across 38 centres in 15 countries of South Asia, South-East Asia and Middle East in 2022 reported UC to be twice as common as CD, 23 but notably, the incidence of CD has increased significantly narrowing the gap between the two conditions. 23 In the KASID study, a reduction in the UC to CD ratio from 6.8 to 2.3 was observed, demonstrating a sharper rise in CD incidence during the study period.21,22 This epidemiological pattern is analogous to the events that unfolded in the 20th century in the West. 24
The rise of IBD in Asia is an alarming trend. Nearly 60% of the total global population (approximately 4.68 billion) reside in Asia, in comparison to 0.6 billion people in North America and 0.75 billion people in Europe. 9 Although the prevalence of IBD in Asia remains lower than in the West, the rising incidence contributes to a large disease burden due to the population density in these regions. The emergence of IBD in Asia signals that it is no longer a disease of the West. It is a global disease that places significant financial and resource burdens on resource-limited countries of Asia, Africa and South America. The direct and indirect costs of IBD on healthcare systems and economies of countries are significant with rising years lost to disability and years lost to life noted in high prevalence countries. 9 If Asia were to stay on the same trajectory in the evolution of IBD, it is likely to experience prevalence rates matching those of the West.
Burden of IBD in India
Indians have been thought to be at low risk of IBD. For nearly five decades, this perception was neither refuted nor confirmed due to the scarcity of data on the incidence and prevalence of IBD in India. Over the last two decades, there has been a gradual accumulation of published literature on IBD in Indian populations that has challenged this observation. Epidemiological data from India have several lacunae and are restricted to hospital-based data or those from small consortiums from one region of the country. However, available data prove that IBD is not a rare entity in India as was previously thought. A summary of the epidemiological studies in India on IBD and their distribution across the country is shown in Table 1 and Figure 2.
Summary of published literature on large epidemiological studies of IBD among the Indian population.

CD, Crohn’s disease; IBD, inflammatory bowel disease; UC, ulcerative colitis.

Heat map depicting the number of IBD-related publications (including case reports, case series and large studies) from different Indian states between 1991 and 2021 (as indexed on PubMed).
A PubMed search was conducted using the search terms India, Inflammatory Bowel Disease, IBD, Ulcerative Colitis, UC, Crohn’s disease, CD, IBDU, Pediatric IBD, Pediatric UC, Pediatric CD or Colitis published between 1991 and 2021. A total of 352,526 results were obtained. Two authors screened the title and abstracts for content related to IBD and the affiliation of the corresponding author. After screening, 347 abstracts with IBD content and affiliation to an Indian University, educational institute or hospital were selected for generating the Indian map-based heat map.
According to data from two population-based studies on UC in the Northern Indian states of Haryana 25 (1984) and Punjab 26 (2003), the prevalence was ~43/100,000 persons. The incidence of UC in 2004 in Punjab was 6.02/100,000 persons. In a more recent prospective study from Hyderabad, the mean annual incidence of UC in 2012–2013 was 5.40 (4.70–6.18)/100,000 persons. 13
CD, on the other hand, suffers from lack of population-based data from India and other low- and middle-income countries. 30 The data on the incidence of CD come from a multi-country prospective study involving 13 countries in the Asia-Pacific region between 2012 and 2013, including Hyderabad, a city in southern India. The estimated mean annual incidence of CD was 3.91 (3.31–4.57) per 100,000, based on a cohort of 367 IBD patients over a period of 1 year. 13 India had the highest incidence of CD among countries in East and Southeast Asia. The incidence of CD in India was higher than the pooled incidence of CD in East Asia (0.34/100,000) and Southeast Asia (0.36/100,000). 13
In contrast to North America and Europe, where the northern latitudes bear the brunt of the disease burden,31,32 IBD has been reported from all parts of north and south India. 27 However, a distinct north–south gradient has been observed in the phenotype of IBD, with UC being predominant in the northern states and CD in the south, the cause for which is unclear. 28
The distribution of disease in the majority of Indian patients with UC is left-sided (E2) or extensive colitis (E3), 13 whereas patients with CD have the ileocolonic disease and an inflammatory phenotype.23,28
Possible factors for increasing incidence in newly industrialized countries
It is generally accepted that IBD occurs as a result of a complex interaction between three important spheres – genetic susceptibility of the host, external environment and intestinal microbiome and the host’s immune system (Figure 3). 33 It has been increasingly recognized that the above factors do not act in isolation. IBD is the result of an aberrant immune response to a dysbiotic gut housed in a genetically susceptible host. We examine current evidence that indicates the changes in genetics and environmental factors in Asia, including in India, and how they have resulted in the emergence of IBD in regions with historically low incidence.

An illustration of the pathogenesis of IBD.
Genetics
The role of genetics in the pathogenesis of IBD became apparent with familial aggregation and twin studies. Since the sequencing of the human genome and advent of rapid and cost-effective genetic sequencing technology, several genome-wide association studies have been undertaken, mostly in Caucasians of European descent, within large IBD cohorts to identify IBD susceptibility loci. These studies have identified 163 genetic loci, 34 which explain only 13.6% of CD and 7.5% of UC, a small fraction of the total heritability of IBD. Investigation of some well-described IBD susceptibility loci such as NOD2 and IL23R in Indians has revealed no association with IBD. 35 However, recent studies have identified polymorphisms in genetic loci associated with IBD, unique to the Indian population, such as TNFSF15 (tumour necrosis factor superfamily) gene, 36 IRGM gene, 37 TLR4 D299G, 38 TLR5 gene, 39 BAT2, MSH5, HSPA1L, SLC44A4, CFB and NOTCH4. 40 The Malaysian study which reported highest incidence in Indians living in Malaysia as compared to other ethnicities further adds strength to the hypothesis that Indians are equally genetically susceptible to develop IBD. 14 However, genetic susceptibility alone cannot sufficiently explain the sudden rise in the incidence of IBD and varying incidence within regions with inhabitants of comparable genetic backgrounds.
External environment
The role of environmental factors is best studied in immigrants from Asia to Western societies. The finding of increased incidence of IBD in second-generation Indian migrants to the UK similar to that of the native general population was revealing. 41 These findings were further strengthened by similar findings from studies in Canada.42,43 They observed that earlier age of immigration was associated with the increased risk of IBD – an increase of 14% for every younger decade of life at immigration. 42 They also observed that South Asians born in Canada were younger at the onset of IBD compared to South Asian immigrants and the general population. 43
A recent meta-analysis of observational studies by Piovani etal. 44 identified nine risk factors (smoking, urban living, vitamin D deficiency among others) and seven protective environmental factors (breastfeeding, tea, physical activity, etc.) with moderate to high epidemiologic evidence of association. Although association does not indicate causation, we examine some of the environmental factors in the Asian context in the following sections.
The gut microbiome and IBD
In recent decades, the microbiome has become a key area of interest in the study of the pathogenesis of chronic inflammatory and immune-mediated diseases. The gut microbiota plays an important physiological role in the supply of nutrition and energy to the enterocytes, the development of the host immune system and host defence. 45
The evidence for the fundamental role played by the gut microbiome in the pathogenesis of IBD has been established in animal studies involving germ-free mice.46,47 The gut microbiome is different in patients with IBD compared to healthy controls, with a consistent increase in pro-inflammatory microbial communities and a depletion of the anti-inflammatory capacities of microbiota.48,49 This alteration in microbiome or dysbiosis in IBD patients via an aberrant immune response and defective barrier integrity results in chronic intestinal inflammation. 45 The identification of mutations in genes involved in the microbiome–immune interactions among patients with IBD and epidemiologic observations implicating risk factors that modulate microbiota such as antibiotic use, diet, cigarette smoking, levels of hygiene, sanitation and infections, further strengthens this hypothesis. 50
There have been several studies in Asia examining the gut microbiome in patients with IBD compared to healthy controls (Table 2). However, majority of these studies are limited by small sample size, heterogeneity of study cohort, severity of disease, treatment exposure and analytical methods. Despite these limitations, the results of these studies are not too dissimilar from the IBD population in the West with a predominance of Actinobacteria, Proteobacteria such as Escherichia coli, Lactobacillus and a decrease in abundance of butyrate-producing species of Firmicutes phyla including Faecalibacterium prausnitzii, Roseburia, Coprococcus and Ruminococcus in patients in IBD.
List of human studies on gut microbiome in IBD from Asia in from 2013 to 2024.

CD, Crohn’s disease; HC, healthy controls; IBD, inflammatory bowel disease; PCR, polymerase chain reaction; RT-qPCR, reverse transcriptase quantitative PCR; 16s rRNA, 16s ribosomal ribonucleic acid; UC, ulcerative colitis.
Current literature suggests intestinal microbiota influences immune response and consequently, gut immune homeostasis. However, the concept of a ‘healthy’ gut microbiome is still unclear. Further research is essential to increase our understanding of the gut microbiome of IBD patients in India. A large study (LogMPie) investigating the microbiome of healthy volunteers across India provides an excellent baseline against which microbiome studies in IBD in India could be compared with. 65
Antibiotic use
It has been borne out in several studies in the West that patients with IBD report a higher exposure to antibiotics prior to IBD diagnosis, compared to healthy controls.66 –68 This epidemiological association is biologically plausible and bolsters the ‘dysbiosis’ hypothesis in the pathogenesis of IBD, as antibiotic use alters the gut microbiome significantly and for a disconcertingly long time, up to 2 years, 69 but it does not confirm causality.
Studies in the Asia Pacific region on antibiotic use as a risk factor for future development of IBD have, however, revealed conflicting results. The study of environmental risk factors in the ACCESS database showed a protective effect of antibiotic use against the development of IBD. 70 The authors hypothesized that antibiotic use may be a surrogate marker of exposure to gastro-intestinal (GI) infections in early childhood which may lead to induction of tolerance. This is in consonance with the hygiene hypothesis discussed later in the article. Interestingly, the same authors in the recently published Eastern Inflammatory Bowel Disease Gut Microbiota (ENIGMA) study have observed that exposure to antibiotics before 18 years of age was associated with the development of CD in an urban and rural Chinese and Australian cohort [adjusted odds ratio (OR), 3.46, 95% CI, 1.38–8.69; p = 0.008]. 71
The divergence observed in the association of antibiotic exposure with IBD between West and East is perhaps due to methodological differences (recall versus registry), differences in antibiotic prescribing practices, access to over-the-counter antibiotics, levels of sanitation, type of infections, etc. However, the diametrically opposite finding noted in the Southeast Asian cohort (ACCESS versus ENIGMA) is intriguing. This re-emphasizes the need for larger, multicentre, prospective studies to evaluate the epigenetic and environmental factors associated with IBD in newly industrialized economies.
Role of diet in IBD
Diet plays a central role in the pathogenesis of IBD through its influence on enteric microbial homeostasis. 72 The western diet rich in ultra-processed food, red meat, high-fat dairy, animal fat, trans unsaturated fat, refined grains and highly refined sugars and low intake of vegetables and fruits, has been consistently associated with increased risk of IBD by altering the gut microbiome, host homeostasis and regulating T-cell immune response.73 –75 Recent data from the ENIGMA study consortium have noted that CD patients have a higher intake of processed food and food additives such as aspartame, sucralose and polysorbate-80, total emulsifiers, artificial sweeteners and titanium dioxide compared to healthy controls and first-degree relatives. 76
The rising incidence of IBD in newly industrialized countries in Southeast Asia is, in part, related to changing dietary habits and culinary practices with increasing ‘westernization’ of diet. Traditionally, the Indian diet mainly comprised locally grown cereals, pulses, vegetables, fruits, fish and meat. Indians have diverse culinary practices and food habits influenced by many cultural identities belonging to various communities and ethnicities, varying agricultural practices, geographical locations and religious beliefs. Given this diversity and heterogeneity, India does not have a typical pan-India diet.
A systematic review (of published literature till July 2015) of dietary patterns in India identified 41 dietary patterns, of which 29 were predominantly vegetarian. 77 Interestingly, upon analysing the studies by splitting them into time periods (as before and after 2000) to obtain temporal trends, the authors noted that dietary patterns, in recent years, were more likely to be characterized by the consumption of wheat, fruit and sweets but less likely to be characterized by vegetables. 77 Another study made a similar observation that there has been a major shift from consumption of coarse grains such as sorghum, barley, rye, maize and millet to consumption of rice and wheat in both China and India, particularly in the urban and high-income groups. 78 The study also noted that Indians consume high levels of dairy products, particularly highly saturated ghee, and high amounts of sugar. 78 These observations signal a shift in the dietary habits of Asians which is concomitant with the epidemiological transition of disease being noted in the region. There is an urgent need for studies to firstly define the changing dietary patterns, cooking and agricultural practices in India and Asia at large, the degree of penetration of ‘western’ foods in Asian households and subsequently to study the role of traditional Asian foods in IBD – both as trigger and therapy.
Breastfeeding
In a recent case–control study in Asia, Ng etal. 70 found that breastfeeding for more than 12 months was markedly protective (>90%) for the development of CD and UC. A systematic review of the role of breastfeeding in the development of PIBD showed breast milk exposure to have a significant protective effect (OR, 0.69; 95% CI, 0.51–0.94; p = 0.02) in the development of early-onset IBD. 79 The inverse association of breastfeeding and IBD has been observed in all ethnicities; however, the magnitude of protection was found to be significantly greater among Asians (OR 0.31, 95% CI, 0.20–0.48) compared to Caucasians (OR, 0.78; 95% CI, 0.66–0.93; p = 0.0001) in CD. 80 Duration of breastfeeding showed a dose-dependent effect with the strongest decrease in risk observed when breastfed for 12 months vis-a-vis 3 or 6 months.70,80 Breastfeeding rates reported in the recent NFHS-5 (National Family Health Survey 2019–2021) published from India are encouraging. The exclusive breastfeeding rate in the first 6 months was 63.7% compared to 54.9% in the NFHS-4 survey of 2015–2016. 81 Exclusive breastfeeding rates were higher in rural (65.1%) than urban (59.6%) areas. 81 It is important to continue to advocate for exclusive breastfeeding for the first 6 months of life, given the strong protective effect against the development of IBD, in addition to the other innumerable beneficial effects of breast milk.
Smoking
Smoking has been consistently shown to be a risk factor for the development of and complicated course of CD and is protective for UC. However, this observation is not replicated in Asian studies. In the study by Emerging Nations Consortium (ENC), which included 10,400 patients from 15 countries in South-East Asia, South Asia and Middle East, around 6% patients were smokers and 5% were ex-smokers. 23 But they found no difference between a history of current or past smoking and UC or CD. 23 Complications such as stricturing disease (B2: 20% versus 19%, p = 0.61) or surgery (15% versus 11%, p = 0.08) were not significantly different between smokers versus non-smokers with CD, respectively. 23 Similarly, two Indian studies found no association between smoking and IBD.82,83 A clear explanation for this epidemiological observation is not forthcoming and as such, no conclusions or recommendations can be made regarding the association of smoking and IBD in Asia, whether deleterious or protective, based on available data.
Hygiene hypothesis and urban living
The hygiene hypothesis also known as the ‘microbial deprivation hypothesis’ or ‘sheltered child syndrome’ refers to the emergence of immune-mediated diseases as a result of continuous improvement in hygiene and living conditions brought about by urbanization. 25 Exposure to infections in early childhood helps establish an immunological balance between pro-inflammatory T-helper cells 1 (Th1) and tolerance-inducing regulatory T-cell response. This prevents the subsequent untoward responses to allergens, microbial or other antigenic stimuli, which are implicated in the pathogenesis of inflammatory disorders. 70
However, hygiene does not have a tangible metric that can be easily measured. Surrogate markers of improved hygiene include gross domestic product, degree of industrialization, level of education, access to clean water, flush toilets, number of siblings, sharing of bedrooms, number of infections, prevalence of infections such as Helicobacter pylori/tuberculosis, etc. Analysis of environmental risk factors from the ACCESS database noted having a pet dog in childhood was associated with a lower risk of development of CD, thus supporting the hygiene hypothesis. 53 Data from India are conflicting. Sood etal. noted that having a private bed and better toilet facilities were associated with a decreased risk of UC, whereas owning a pet was associated with an increased risk of UC, which contradicts the hygiene hypothesis. 68 Similarly, in another Indian prospective multicentre study, living in a rural area was a risk factor for the development of IBD. 67
Environmental factors associated with urban living such as depletion of greenspace and blue space (water) and rising air pollution levels have been investigated as risk factors for the development of IBD. Retrospective cohort studies using linked population-based health and environmental data in Canada concluded that higher exposure to residential greenspace during childhood was protective against and conversely, early life exposure to air pollution was associated with the development of PIBD, respectively.84,85 This observation was also noted by Zhang etal. 86 using the large UK biobank study database where higher residential greenspace, blue space and natural environment were found to be protective against adult-onset IBD. These newly emerging data although preliminary and merely epidemiological associations, throw light on the possible factors influencing the paradigm shift in burden of IBD being experienced by most emerging Asian economies. Importantly, they provide potential novel avenues for prevention thus aiding public health policy and urban planning in this region.
Paediatric IBD
PIBD is distinctly different from adult onset IBD in its phenotype and disease behaviour as it is more extensive and severe at onset, with a refractory course. 87 Nearly a quarter of the new cases of IBD have onset below 20 years of age. 88
Burden of PIBD in Asia
As observed in adult-onset IBD in newly industrialized countries of Asia, Africa and South America, 4 the global rise in incidence has been noted in childhood-onset IBD as well. 89 Epidemiological data on PIBD from Asia are limited to large tertiary and quaternary referral centres. Recent data indicate a low overall incidence of PIBD in Asia compared to Europe and North America 89 ; however, epidemiological trends available from some parts of Asia such as Singapore and Saudi Arabia indicate a sharp increase in incidence rates in the preceding decade. 90 West Asia reports the highest incidence of PIBD in the region with an incidence ranging from 0.5 to 21.6 per 100,000 person years. 89 Consistent with data on Adult IBD in Asia, the incidence of Paediatric CD is rising across Asia in comparison to Paediatric UC. This phenomenon is notable in Singapore which has witnessed a 10-fold rise in the incidence of Paediatric CD from 0.23/100,000 person-years in 1994–2004 to 2.28/100,000 person-years in 2005–2015. 91 Similar trends of a steep rise in CD incidence have been noted in Taiwan and Japan.92,93
Burden of PIBD in India
The true incidence and prevalence of PIBD in India remains a knowledge gap. Data regarding PIBD in India are scanty, heterogeneous and limited to largely single-centre studies and one multicentre prospective study from select Paediatric Gastroenterology Centres around India (Table 3).
Summary of paediatric IBD studies from India.

CD, Crohn’s disease; IBD-U, inflammatory bowel disease-unclassified; UC, ulcerative colitis.
Despite the limited data, there are signals pointing to a rise in the incidence of PIBD. Poddar etal. 96 noted a significant increase in the number of cases diagnosed with IBD in their North Indian tertiary referral centre in a 5-year period between 2011 and 2016 when compared to the last decade (2001–2010). The reasons for the increase in incidence in newly industrialized countries are manifold. 89 It includes a true rise in the incidence in PIBD as is being observed across the globe, increasing awareness among paediatricians regarding PIBD resulting in earlier recognition and referral, and better diagnostic capabilities with the availability of paediatric gastroenterologists, endoscopy and imaging services.
Prospective data from nine centres across India reveal CD as the most common PIBD phenotype (65.2%) followed by UC (28%) and IBDU (6.7%). 97 As seen in the adult cohort, 28 a north–south divide in IBD phenotype with UC being predominant (50%) in Northern India and CD constituting the majority (75.3%) of PIBD cases in Southern India has been noted.94,97 Disease location and extent of PIBD in Indian children is similar to reports from the West. The majority of patients with UC have pancolitis (58%) and most patients with CD exhibit ileocolonic disease (58%). 97 Rates of perianal CD (11%) also mimic those in European children. 97
Very-early onset IBD
The majority of childhood IBD is polygenic in nature. The genetic influence on the pathogenesis of IBD decreases with the advancing age of the onset of disease. As such, the genetic burden of disease is highest in the youngest. Very early-onset IBD (VEO-IBD) is the umbrella term that refers to the onset of disease under 6 years of age which includes infantile IBD (onset <2 years of age) and neonatal-onset IBD – onset (onset <28 days of life). 98 VEO-IBD is phenotypically and genetically distinct from older onset IBD and accounts for 4–15% of PIBD. 99 VEO-IBD has a stronger family history of IBD, a higher prevalence of extraintestinal manifestations and are more likely to be monogenic in nature. 100 Till date, 75 genes have been implicated in monogenic IBD. 101 Variants in these genes may result in defective T-cell immune tolerance, epithelial barrier dysfunction, defect in cells regulating inflammation (interleukin-10 signalling defect), neutrophil dysfunction, combined or isolated defect in T and B-cell and hyperinflammatory disorders. 99 Monogenic disorders contribute to 10–15% of infantile IBD and 7–10% of VEO-IBD. 102 It is crucial to recognize VEO-IBD as a distinct entity as it has a different clinical phenotype, diagnostic algorithm, management options and outcomes compared to later onset IBD.
VEO-IBD in India
Data on VEO-IBD from India are sparse and include case reports, single-centre retrospective data 103 and one prospective multicentre study. 97 VEO-IBD constituted 19.8% of a total of 325 children with IBD, as reported recently by Srivastava etal. 97 in their prospective multicentre study of 9 select Paediatric GI centres. In a large single-centre study of 292 PIBD patients, Banerjee etal. 103 reported 22 (7.5%) children with VEO-IBD. Most patients with VEO-IBD had IBD-U, isolated colonic disease, 97 a strong family history of IBD and an aggressive phenotype. 103 The limiting factor of these studies is the lack of genetic data in these cohorts. The proportion of monogenic IBD in VEO-IBD in Indian children is yet to be elucidated.
Challenges in diagnosis and management of IBD in Asia
Paucity of epidemiological data: The existing data, although heterogeneous, are pointing towards a rising incidence in both adults and PIBD in Asia. Population-based studies on the incidence and prevalence of IBD are restricted to certain countries from Southeast Asia, and are lacking from several parts of South Asia, particularly India, where the true burden of the disease is unknown.
Presence of enteric infections and tuberculosis: Asia, in contrast to Europe and North America, faces the dual problem of enteric infections and IBD which mimic each other. The endemicity of tuberculosis, a close differential to CD, poses significant challenges in diagnosis. Differentiating intestinal tuberculosis (ITB) from CD remains a clinical dilemma given the significant overlap between the two granulomatous inflammatory conditions. Clinical features such as concomitant pulmonary involvement, ascites, night sweats and shorter duration of symptoms favour a diagnosis of ITB. 104 Endoscopically, involvement of fewer than four segments of the bowel, patulous ileocecal valve, transverse ulcers, scars or pseudopolyps strongly indicate ITB. 104 However, none of these features is specific for CD or ITB. Misdiagnosis of ITB as CD carries the risk of disseminated TB due to the use of immunosuppressive therapy. As such, the Asian Organization of Crohn’s and Colitis Guidelines in 2021 recommend a therapeutic trial of antitubercular therapy (ATT) when diagnosis is uncertain. 105 Conversely, empirical ATT results in the risk of drug-related toxicity and delays in referrals and diagnosis of IBD. Concerningly, a study from India noted that patients who received a therapeutic trial with ATT before a diagnosis of CD had accelerated progression to stricturing disease and a higher need for surgery. 106 Among ENC countries, an empirical therapeutic trial of ATT was prescribed to 19% of patients with CD, 2% of UC and 10–11% of children with IBD. India accounted for the second highest proportion of empirical ATT among the ENC nations.23,97,103
Diagnostic delay: It is well established that delay in diagnosis leads to variable periods of untreated disease with its ensuing complications. A diagnostic delay of >18 months in CD was associated with higher rates of intestinal resection (17% versus 13%, p = 0.009) but no difference in rates of stricturing complication (22% versus 20%, p = 0.12) in the ENC study. 23 A median diagnostic delay from onset of symptoms to diagnosis was 10 months, which was significantly longer for CD versus UC (12 versus 6 months, p < 0.0001). 23 In PIBD, a diagnostic delay of >6 months was observed in 76% of children. 103 Delay in diagnosis may be related to delayed presentation or delayed referrals from primary care providers (PCP).
Lack of awareness among general practitioners and PCPs regarding IBD: Despite the rapidly changing epidemiology of IBD, it is still considered a disease of the West. This misconception among practising physicians and paediatricians results in low clinical suspicion for IBD, thereby leading to delayed diagnosis.
We list the possible factors contributing to the knowledge–attitude–practice gap in the diagnosis and management of IBD and suggest remedial measures (Table 4, Figure 4).
Lack of uniform and affordable access to biologics: The introduction of biologics was anticipated to reduce costs by reducing hospitalizations and surgery; however, the cost of illness in IBD is rising, the main driver being the cost of biologics.107,108 Anti-TNFα agents are widely available in India and other parts of Asia; however, a survey of Indian gastroenterologists in 2012 revealed the use of anti-TNFα agents to be low (0.8%) in the treatment of IBD. 27 Low biologics use in India is likely related to prohibitive cost and lack of universal healthcare insurance resulting in significant out-of-pocket expenditure for families. 109 Non-uniform access to biologics, fear of opportunistic infections and TB reactivation, and lack of experience with optimal use of biologics and low ratio of gastroenterologists for the population are all contributing factors.107,110,111 A recent Asia-wide survey to determine IBD treatment strategies revealed that the availability of newer biologics such as anti-integrins, anti-IL12/23 and JAK inhibitors across Asia is heterogeneous. 112 Ustekinumab and Vedolizumab have only recently become available in India and are not yet available in large parts of South Asia. The survey also showed that gastroenterologists in Asia prefer a step-up, or an accelerated step-up strategy compared to a top-down strategy for induction of remission in moderate to severe disease. 112
Possible reasons for knowledge–attitude–practice gap in diagnosis of IBD in Asia and suggested remedial measures.
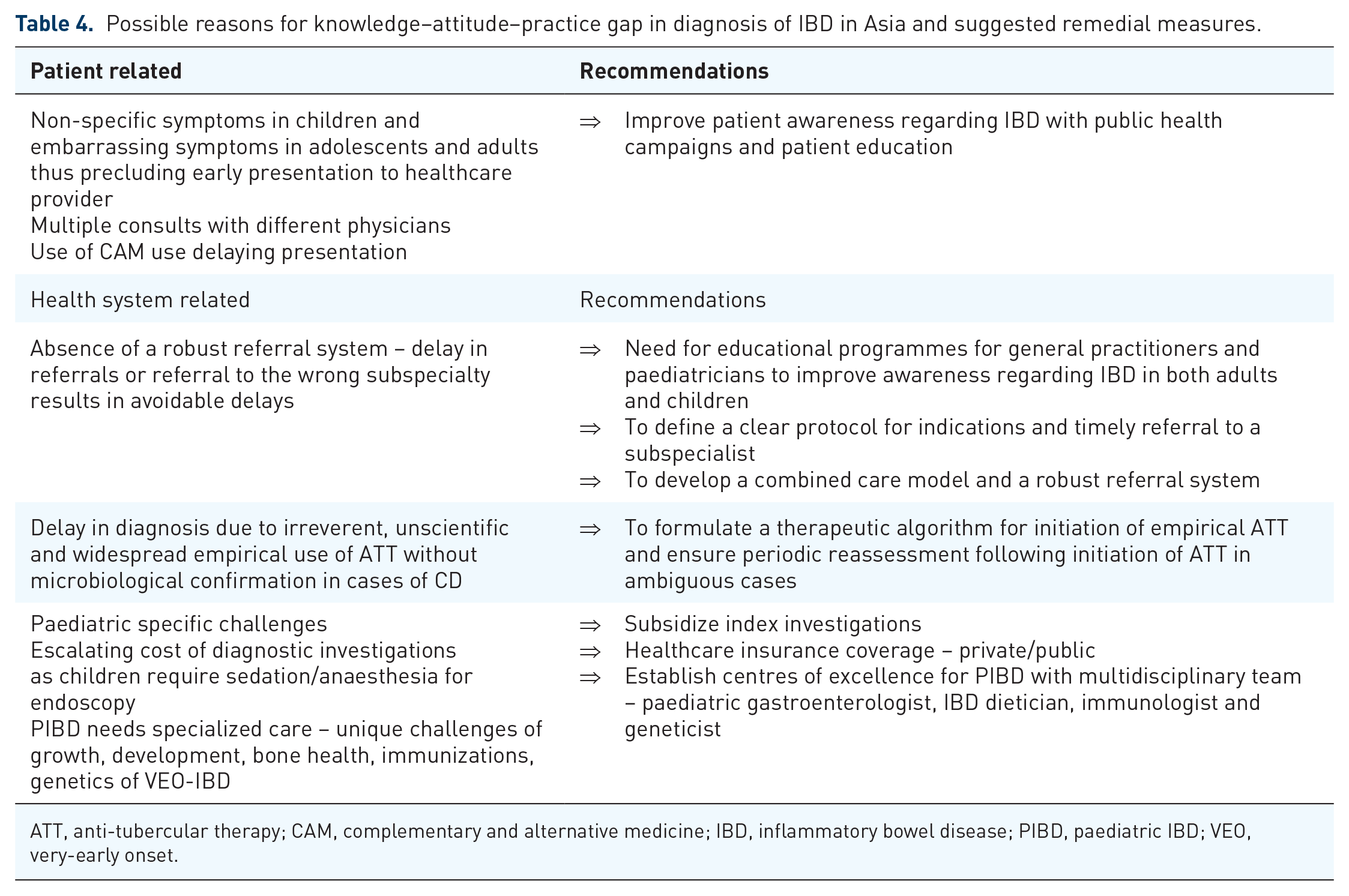
ATT, anti-tubercular therapy; CAM, complementary and alternative medicine; IBD, inflammatory bowel disease; PIBD, paediatric IBD; VEO, very-early onset.

An overview of challenges and remedial measures for diagnosis and management of IBD in developing countries.
Conclusion and future directions
Current available evidence suggests a significant rise in IBD in India and other parts of South Asia. Its chronic relapsing course affects all age groups, and the cumulative prevalence is bound to place a significant burden on healthcare resources in the future. However, the paucity of reliable population-based data makes it challenging to plan appropriate allocation of resources. There is an urgent need for nationwide epidemiological studies to establish the true disease burden that will help healthcare professionals and policymakers. Furthermore, we need to identify regional risk factors contributing to the rising incidence of IBD in India and South Asia. The data on disease burden and risk factors will help develop a strategy to effectively manage this surge in the disease. As the rise of IBD in India and other Asian countries is relatively recent, we are uniquely placed to study the risk factors and disease characteristics (demographics, phenotype, environment, diet, microbiome) compared to the more advanced disease trajectory of the western countries. The key differences may perhaps reveal potential therapeutic targets and advance our knowledge of prevention. IBD requires a multi-pronged approach at all levels of healthcare for effective management, within a resource-limited setting. A systematic collaborative approach with high-quality research at its core is of utmost importance in facing this challenge.