
Abstract
Inflammatory bowel disease (IBD) is a gastrointestinal disorder characterized by chronic relapsing inflammation and mucosal lesions. Reliable biomarkers for monitoring disease activity, predicting therapeutic response, and disease relapse are needed in the personalized management of IBD. Given the alterations in metabolomic profiles observed in patients with IBD, metabolomics, a new and developing technique for the qualitative and quantitative study of small metabolite molecules, offers another possibility for identifying candidate markers and promising predictive models. With increasing research on metabolomics, it is gradually considered that metabolomics will play a significant role in the management of IBD. In this review, we summarize the role of metabolomics in the assessment of disease activity, including endoscopic activity and histological activity, prediction of therapeutic response, prediction of relapse, and other aspects concerning disease management in IBD. Furthermore, we describe the limitations of metabolomics and highlight some solutions.
Introduction
Inflammatory bowel disease (IBD), a chronic recurrent inflammatory disease of the gastrointestinal tract, is composed of Crohn’s disease (CD) and ulcerative colitis (UC). 1 These two disorders differ in many respects. CD is characterized by dispersed lesions and transmural inflammation that can occur anywhere in the gastrointestinal tract, with the most frequent symptoms of abdominal pain, diarrhea, fistulae, obstruction, and/or perianal lesions. 2 In UC, the lesions are continuous and limited to the mucosal layer of the colon and rectum, which can most commonly lead to bloody diarrhea and rectal bleeding.3,4
The prevalence of IBD is higher in developed countries than developing countries. 5 Nevertheless, the prevalence and incidence of IBD are increasing globally, especially in newly industrialized countries. 6 Therefore, the disease burden will become ever higher in both developed and developing countries. 7 To reduce the disease burden, personalized management, including regular monitoring of disease activity, matching the patients with the proper treatment, and predicting prognosis, is important. Previous studies have referred to a variety of serological and fecal biomarkers, such as serum C-reactive protein (CRP), interleukin 6, fecal calprotectin, and lactoferrin, which serve as surrogate markers for the diagnosis and management of IBD. 8 However, these available biomarkers could only assist with the activity monitoring and prognosis of IBD to some extent, instead of being considered as a gold standard in the personalized management of IBD. Additional studies or techniques are necessary to discover potential and effective biomarkers to guide the management of IBD.
Given that patients with IBD often exhibit specific metabolomic profiles, metabolomic analysis is a potential tool for identifying diagnostic and therapeutic markers of IBD. 9 Metabolomic analysis is a technique with the advantages of high throughput, high sensitivity, and high accuracy for the qualitative and quantitative study of small metabolite molecules in biological samples, including feces, urine, serum, plasma, breath, and biopsy samples. Metabolomic analysis covers a wide range of metabolites with a molecular mass less than 1500 Da, including but not limited to sugars, lipids, amino acids, nucleic acids, organic acids, fatty acids, and some exogenous chemicals. 10 Through metabolomics analysis, promising metabolites or models based on metabolites for facilitating accurate diagnosis and personalized management of IBD will be discovered. Although previous studies have summarized the role of metabolomics in the identification of diagnostic markers for IBD and their possible association with pathological mechanisms,9,11–13 few other clinical applications of metabolomics have been reviewed in detail. Therefore, in the present review, we highlight the possible value of metabolomics in evaluating disease activity for IBD, as well as its potential in predicting treatment response and disease relapse.
Metabolomics
Metabolomics is the qualitative and quantitative study of a suite of small metabolite molecules in biological samples, which symbolizes the metabolic phenotypes of a living system under specific conditions, or in other words, reflects the metabolic response to pathophysiological stimuli or even genetic modification at a certain time point. 10 It includes both targeted and untargeted methods. Targeted metabolomics often focuses on specific known metabolic pathways and can be used for the quantification of metabolites. However, untargeted metabolomics tends to analyze a large number of metabolites in a sample without bias and can be used for the identification of unknown metabolites.14,15 In the existing literature, analytes in metabolomics of IBD involve an immense variety of metabolites participating in various metabolic pathways in organisms, such as the tricarboxylic acid cycle, urea cycle, or fat oxidation. These metabolites can be roughly classified as endogenous and exogenous substances. The former includes organic acids such as citrate and succinate, lipids such as sphingolipids and glycerolipids, amino acids such as histidine and cystine, short-chain fatty acids (SCFAs), glycosylation products, and other endogenous molecules. Exogenous substances including different kinds of xenobiotics have also been mentioned in some studies.11,13
The primary analytical techniques for metabolomics are nuclear magnetic resonance (NMR) spectroscopy and mass spectrometry (MS) coupled with gas or liquid chromatography. 16 NMR spectroscopy distinguishes metabolites by the resonance frequency of nuclei in a magnetic field. Since the frequency and pattern of resonance vary with the chemical environment, each metabolite with a specific molecular structure generates a unique resonance, showing characteristic chemical shifts in the spectra. 17 MS, however, ionizes and fragments the compounds into smaller molecules of different mass-to-charge ratios, which can be measured by a detector and then give rise to corresponding mass spectra. Ionization and fragmentation are to a large extent determined by the chemical structures of metabolites, which enables the identification of different compounds. Chromatography used prior to MS analysis physically separates the metabolites so that the detection of individual molecules can be enhanced. 18 Both NMR spectroscopy and MS coupled with chromatography are high-throughput techniques and have their own advantages and limitations. 19 As compared to MS, NMR spectroscopy requires minimal sample preparation and has a higher quantitative ability and reproducibility without sample destruction. Nevertheless, signals of metabolites with low concentrations may be covered and cannot be identified due to overlapping signals, leading to a lower sensitivity and narrower detection range as compared to MS techniques. With the help of bioinformatic tools, data acquired from NMR or MS can be processed automatically. 14 Multivariate statistical techniques, such as principal components analysis and partial least squares discriminant analysis, are widely applied in metabolomics studies to discover distinct metabolite profiles in different sample classes. 20
Metabolomics for assessing disease activity in IBD
The assessment of disease activity in IBD is an essential step in judging the stage of the disease, selecting an appropriate treatment plan, monitoring the progress of the disease, and evaluating the treatment effect.21,22 Clinical remission and endoscopic healing in IBD are recommended as intermediate and long-term therapeutic targets, respectively. Histological healing also assists in assessing the depth of treatment response in UC. 23 Therefore, a precise and convenient assessment of disease activity is necessary for the management of IBD. Studies have found that changes in the levels of some metabolites in patients with IBD are strongly associated with the severity of disease activity, and models based on metabolomic findings are capable of accurately distinguishing patients with active disease from those in remission. Since researches that focus on metabolomics and clinical disease activity contribute to revealing disease characteristics rather than patient management, in this section, we just review studies aimed at assessing the endoscopic or histological activity of IBD through metabolomics (Table 1).
Metabolomic analysis and endoscopic disease activity in IBD.
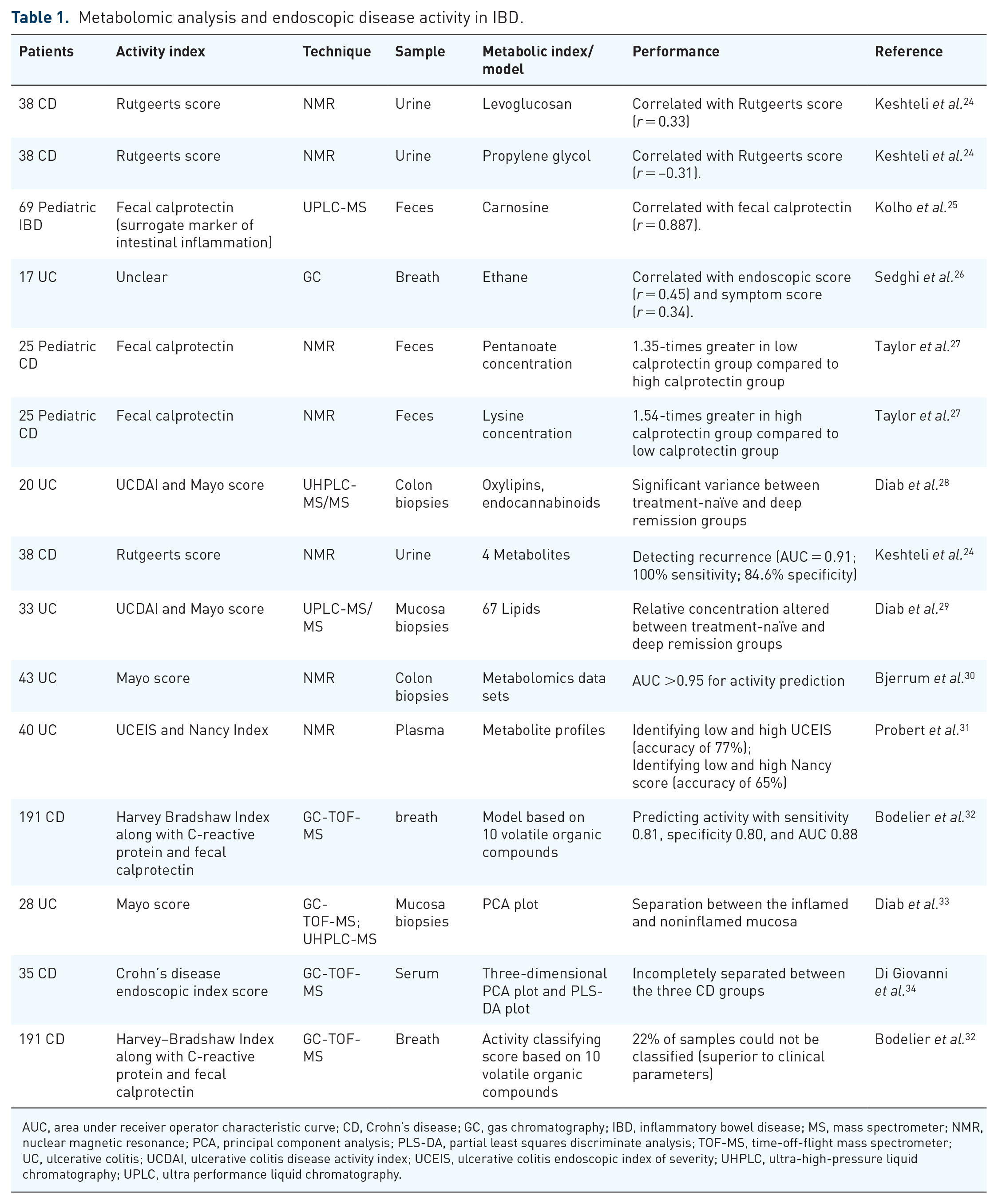
AUC, area under receiver operator characteristic curve; CD, Crohn’s disease; GC, gas chromatography; IBD, inflammatory bowel disease; MS, mass spectrometer; NMR, nuclear magnetic resonance; PCA, principal component analysis; PLS-DA, partial least squares discriminate analysis; TOF-MS, time-off-flight mass spectrometer; UC, ulcerative colitis; UCDAI, ulcerative colitis disease activity index; UCEIS, ulcerative colitis endoscopic index of severity; UHPLC, ultra-high-pressure liquid chromatography; UPLC, ultra performance liquid chromatography.
Metabolomic analysis and endoscopic activity
Several studies have revealed that a variety of metabolites from different samples are related to endoscopic activity in patients with IBD. Bodelier et al.
32
conducted a prospective cohort study of 725 exhaled air samples from 191 patients with CD to explore potential volatile organic compounds (VOCs) to discriminate the active and remission patients. They found that remission patients were characterized with elevated decanal level and reduced concentration of other nine VOCs. Moreover, in breath samples, ethane was mentioned to be positively correlated with the endoscopic score of UC in another study.
26
Through metabolomics analysis, several metabolites in urine sample, including ethylmalonate,
Besides single metabolites, previous studies have reported statistical models based on metabolomics for distinguishing different severities of endoscopic inflammation in patients with IBD. Predictive models based on mucosal biopsies were confirmed to exhibit good performance in predicting endoscopic inflammation in UC.30,33 Probert et al.
31
found that the plasma metabolite profiles were able to discriminate endoscopic remission from endoscopic activity with a sensitivity, specificity, and accuracy of 82%, 82%, and 77%, respectively. In patients with CD, an established statistical model based on the breathograms of 10 discriminatory VOCs from breath samples also had a high sensitivity and specificity for the identification of remission and active patients.
32
Moreover, the model combined with urine ethylmalonate,
Metabolomic analysis and histological activity
Histological activity can persist in patients with IBD despite endoscopic remission and is now considered to be a significant indicator in predicting disease progression in patients with UC. 36 However, only one study has investigated the ability of metabolomics to assess histological activity. 31 Probert et al. performed plasma NMR spectroscopy to study the discrepant metabolite profile between patients with UC showing histological remission and moderate to severe histological activity. The study found that plasma concentrations of five lipoproteins were elevated in patients with histological activity, while concentrations of valine, glucose, and myo-inositol declined. Furthermore, the researchers built a model based on these metabolites to identify histological remission with an accuracy of 65%. In the future, additional studies are needed to explore the abilities of different methods of metabolomics or differently sourced samples for assessing histological activity in IBD.
Metabolomics for predicting the therapeutic response in IBD
Because of the heterogeneity of IBD, there is not one specific therapy that can satisfy all the patients. Thus, the prediction of therapeutic response and matching the right patients with the right treatment are essential in clinical practice. In this section, distinctive metabolomic signatures that might be useful for identifying different responses of patients with IBD after certain therapies are summarized (Table 2).
Metabolomic changes can reflect therapeutic response in IBD.

Anti-TNF, anti-tumor necrosis factor; AUC, area under receiver operator characteristic curve; CD, Crohn’s disease; EEN, exclusive enteral nutrition; FMT, fecal microbiota transplantation; GC, gas chromatography; HILIC-LC-MS/MS, hydrophilic interaction liquid chromatography coupled to mass spectrometry; IBD, inflammatory bowel disease; MS, mass spectrometry; NMR, nuclear magnetic resonance; Rem, remission; Res, responders; TOF-MS, time-of-flight mass spectrometer; UC, ulcerative colitis; UPLC-MS, ultra performance liquid chromatography mass spectrometry.
Metabolomic profiles and therapeutic response of biologics
In a recent guideline, anti-tumor necrosis factor (TNF) agents, such as infliximab, adalimumab, and certolizumab pegol, have been recommended to be used in patients with moderate-to-severe CD who are refractory to corticosteroids or immunomodulators. 49 It is also strongly recommended that vedolizumab, tofacitinib, or anti-TNF therapy including adalimumab, infliximab, or golimumab should be used for induction and maintenance of remission in moderately to severely active UC. 50 Nevertheless, around 30–50% of patients show primary or secondary nonresponse to biologics therapy.51,52 Thus, prediction of the therapeutic response to these biologic agents is important for optimizing disease management. Through metabolomic analysis, several studies have uncovered that metabolite concentration could reflect and even predict the therapeutic response of these biological agents in patients with IBD. Bjerrum et al. 48 conducted a retrospective cohort study including 87 patients with IBD and 37 healthy controls to investigate the variation of serum lipid metabolomic profiles after 14-week anti-TNF therapy. They demonstrated that the lipid profiles of patients with IBD were clear discriminated from the healthy controls before anti-TNF therapy. However, only the lipid profiles of patients with remission UC, instead of nonresponse UC or remission CD, became inseparable from the healthy controls after 14-week anti-TNF therapy. These results indicated that patients with UC who responded to anti-TNF treatment had a remarkable serum metabolomic change, which may help for discovering potential prognostic metabolites. In addition to different types of IBD, different biological agents also had distinct impacts in serum metabolites. A sustained increase in serum tryptophan (TRP) levels was observed in patients with IBD who responded to infliximab therapy, while patients nonresponding to infliximab or receiving vedolizumab therapy did not have a significant change in TRP levels. 39
Furthermore, metabolomics was capable of exploring promising metabolites or models to predict therapeutic response to biologics in IBD. Ding et al.
37
performed a prospective, longitudinal cohort study of 76 patients with CD and found that many bile acids from feces, serum, and urine manifested differentiated signatures between responders and nonresponders. By combining changes in the levels of these representative markers in each sample type, especially in fecal samples, the anti-TNF response could be accurately predicted. Moreover, several lipid markers in serum and feces were reported to exhibit altered concentrations in responders compared to nonresponders, and the fecal lipid profile had a higher predictive accuracy than the serum lipid profile. Excitingly, another study found that response to infliximab in pediatric patients with CD could be predicted at baseline through fecal metabolomic approach.
47
Patients responding to infliximab showed relatively high levels of glycine, linoleic acid, and
Metabolomic profiles and therapeutic response of fecal microbiota transplantation
Fecal microbiota transplantation (FMT) is an effective method of directly changing the gut microbiota of recipients to normalize the composition, thereby achieving therapeutic benefits. 53 As previous studies have shown that FMT is proposed as a therapeutic approach to induce remission in patients with CD and UC.54,55 Several studies have found that changes in metabolomics can reflect disease remission after FMT treatment. One prospective study 46 proved that significant alterations in urinary metabolic profiles of patients with CD who experienced clinical improvement or remission were achieved at the pre-second FMT compared with those at pre-first FMT. In addition, Paramsothy et al. 44 found that the primary outcome of FMT treatment could be predicted at baseline according to the fecal metabolomic profiles. The increased levels of SCFA biosynthesis and secondary bile acids, as well as the decreased levels of heme and lipopolysaccharide biosynthesis, were considered as markers that enabled patients in remission at week 8 to be distinguished from those who did not achieve remission. Similarly, another study of fecal metabolomes of pediatric patients with UC 42 confirmed that in responders after FMT, there was a decrease in acetic acid levels and an increase in butyric acid levels. However, stool SCFAs, such as butyrate, were reported to have no correlation with either anaerobically prepared pooled donor FMT effect or disease activity of UC. 43 Hence, whether SCFAs can predict the therapeutic response of FMT is still controversial, and additional studies are needed to confirm their roles.
Metabolomic profiles and therapeutic response of exclusive enteral nutrition
Exclusive enteral nutrition (ENN), a nutritional intervention, is the treatment of choice for pediatric CD, the remission of which can be induced in up to 80% of cases. 56 EEN is effective as a corticosteroid in the induction of clinical remission and is also superior in inducing mucosal healing. 57 Studies have shown that the fecal metabolic profiles of children with CD are associated with a response to EEN treatment. A prospective multicenter cohort study 45 showed that the responses of pediatric CD patients to EEN could be predicted at baseline using fecal metabolic profiles. Many amino acids and several other metabolites in fecal samples were normalized in responders at follow-up but not in nonresponders, indicating their important role in reflecting therapeutic responses. In addition, another study of 15 pediatric patients with CD 40 analyzed fecal metabolites and found that at subsequent follow-up points during EEN, there was a decrease in the levels of butyric acid and an increase in the concentrations of total sulfide. The magnitude of these changes became larger when excluding the patients who did not experience clinical remission from the analysis, implying different metabolomic characteristics in patients who achieved remission after EEN treatment and those who did not. Metabolic trajectories of urinary metabolites over 8 weeks were also monitored in a pediatric retrospective cohort study of 26 patients with IBD who received corticosteroid or EEN therapy. 41 Urinary octanoyl glucuronide, pyridoxic acid, and pantothenic acid were shown as specific dietary biomarkers of clinical remission after EEN treatment in pediatric patients with IBD. These findings offer support for the utility of urinary metabolomics in the early therapeutic monitoring of pediatric patients.
Metabolomics for predicting disease relapse
IBD is a disease characteristic of a relapsing–remitting course. Approximately 10–30% of patients tend to experience a disease relapse annually despite achieving remission.58,59 Therefore, it is critical to pre-identify patients with a high risk of relapse so as to prospectively modify the strategies of disease management, which make it possible to conduct effective interventions for relapse prevention in patients. Several articles that elaborate the potential metabolic markers for the prediction of relapse are presented in this section (Table 3).
Metabolomics in predicting disease relapse in IBD.
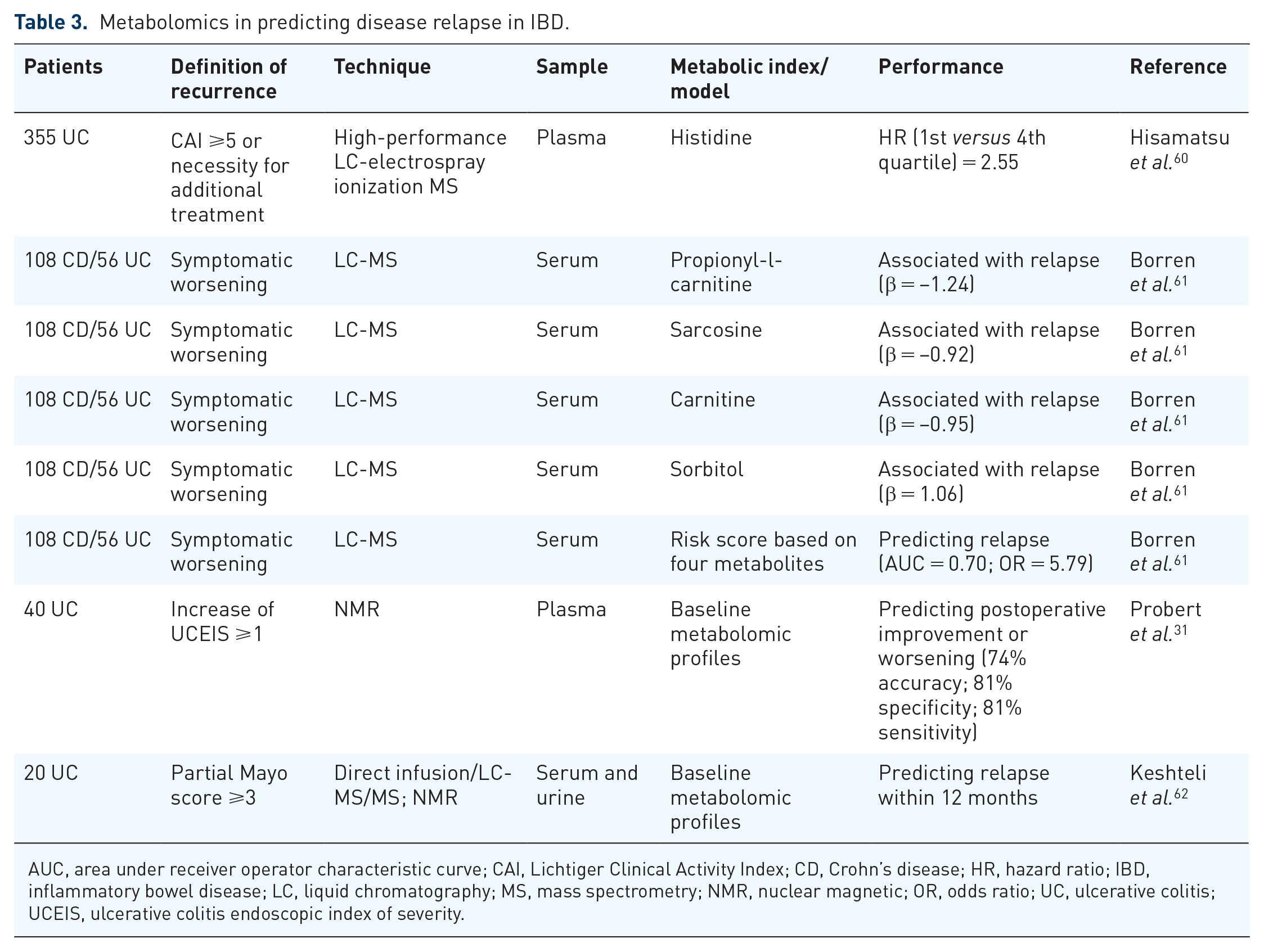
AUC, area under receiver operator characteristic curve; CAI, Lichtiger Clinical Activity Index; CD, Crohn’s disease; HR, hazard ratio; IBD, inflammatory bowel disease; LC, liquid chromatography; MS, mass spectrometry; NMR, nuclear magnetic; OR, odds ratio; UC, ulcerative colitis; UCEIS, ulcerative colitis endoscopic index of severity.
A prospective cohort study of 40 patients with UC showed that a baseline plasma metabolite profile performed well in predicting worsening of postoperative endoscopic activity with an accuracy of 74%.
31
Two studies have investigated the relationship between the probability of clinical recurrence of UC and the metabolome. A total of 355 patients with remission UC were observed prospectively in one of the studies,
60
and it was shown that a decreased concentration of plasma histidine was associated with an increased risk of relapse. In another study,
62
patients with clinical relapse were demonstrated to have significantly higher levels of serum 3-hydroxybutyrate, acetoacetate, acetone, and urinary trans-aconitate, while urinary acetamide and cystine levels decreased. In addition, a prospective cohort study of 164 patients with IBD
61
identified four serum metabolomic markers, sarcosine, carnitine, propionyl-
Other applications of metabolomic profiling in the management of IBD
Some studies have mentioned other possible utilities of metabolomic profiling in IBD management. As noted in a prospective follow-up study of 535 patients with IBD, 39 a lower concentration of serum TRP was linked with a higher probability of the need for surgery in patients with IBD. Moreover, Clerc et al. 63 found the associations between plasma glycosylation patterns and disease progression, and the need for increased drug potency or surgery, suggesting a reference for therapy and prognosis. In addition, fecal alanine levels were found to be significantly different between pediatric patients with IBD with high perceived stress and low perceived stress. 64 Since the stress level was considered as one of the impact factors of future disease activity in patients with IBD,65,66 fecal alanine levels may assist in predicting disease progression and recurrence. Fatigue has been reported as a disabling symptom in many patients with IBD despite being in remission. Its etiology remains unclear, limiting treatment pertinency. 67 In a prospective study of 166 patients with IBD, 18 serum metabolites, such as methionine, TRP, proline, and sarcosine, were found to be significantly different between patients with and without fatigue, which advanced our understanding of the mechanisms of fatigue and the possible therapeutic targets. 68 Moreover, fecal isocaproyltaurine was confirmed as a useful joint marker for identifying Clostridioides difficile infection in patients with IBD. 69
Limitations of metabolomics and corresponding solutions
There remain some limitations of metabolomics that, to some extent, hamper the transition between laboratory research and the clinical application of metabolomics in IBD.
Above all, previous studies have demonstrated that age, gender, and environmental factors such as diet, lifestyle, toxins, and cultural trends can influence metabolic phenotypes.70–73 Therefore, both clinical research and applications of metabolomics should take the influence of these confounding factors into account, especially urinary metabolomics, which are thought to be more susceptible to environmental factors than metabolomics of other sample types.70,72 Otherwise, biased results and even erroneous conclusion may be drawn. As noted in a prospective study for relapse prediction of UC, concentrations of plasma histidine and glutamate are affected by age and gender in patients with UC. 60 After gender and age adjustment, the association between histidine and the risk of relapse was more obvious, while the opposite was true for glutamate. Moreover, disease severity, concomitant therapy, and genetic variants in patients with IBD are also non-negligible confounders in prognostic studies with metabolomics.13,74 For example, the metabolism and drug toxicity of thiopurine, a widely used drug in IBD, is strongly influenced by the genetic variants of NUDT15, TPMT, and HLA.75–77 If these genetic biomarkers are not considered in metabolomics research concerning the therapeutic efficacy of thiopurine, biased results will be generated. Thus, it is important to have an appropriate study design and perform robust statistical adjustments for potential confounders to make metabolomic profiles reliable for application in clinical practice.
In addition, some contradictory results have been reported in previous studies, which may result from the heterogeneity of cohorts, sampling techniques, or analytical methods. Previous studies have revealed that the quality of acquired metabolomic data can be strongly influenced by sample preparation and the analytic approaches undertaken, which is likely to lead to significant variability in the final metabolomic profiles.78–80 Since the metabolome of an organism is highly complex, there is no single and uniform strategy to analyze all metabolites, 81 resulting in distinct analytic methods and instruments used for different sample types and research purposes, which makes it difficult to compare and integrate the results from different studies. Therefore, it is necessary to further verify the role of metabolites that have been identified as predictive biomarkers in the disease management and prognosis of IBD following the standardized procedures from sample preparation to analysis, and to determine the most appropriate sampling and analytical methods according to the properties of the target metabolites for clinical application.
Another limitation of metabolomics is that metabolomic profile alterations in patients with different disease activity or prognosis are hard to interpret since the mechanism behind these changes remains unknown. Fortunately, the integration of metabolomics and other omics, especially the microbiome, can provide more comprehensive and profound insights into metabolic characterization. Metabolites are downstream of the genome–transcriptome–proteome and are affected by the metabolism of various microbiota in vivo, so that multiomics studies create an opportunity to explore the interactions of genes, proteins, metabolites, and microbiota and to uncover the pathophysiological mechanisms behind the characteristics of metabolomics.11,82,83 This enables to explain the causes of metabolic changes in patients with IBD. In addition, the integration of multiomics may enable the identification of an optimal set of biomarkers for the management of IBD. For instance, a multivariable model combining metabolomic and proteomic risk scores to predict clinical relapse in IBD exhibited a superior performance to a metabolomic or proteomic model alone in a prospective cohort study. 61 Similarly, another study revealed that a model of baseline clinical, proteomic, metabolomic, and metagenomic markers showed a higher predictive value in predicting the biologic therapeutic response than a model of microbial taxa alone. 84 Therefore, metabolomics is still a promising and reliable technology to facilitate the personalized managements in IBD when addressing these limitations.
Conclusion
Owing to the advantages of satisfactory sensitivity and precision, high throughput, convenient sampling, and noninvasive characteristics, metabolomics has attracted increasing attention in IBD research in recent years. The potential of metabolomic profiling in the management of IBD is gradually being recognized. Many metabolites from different types of samples were found to be candidate predictors of disease activity, therapeutic response, or relapse. Several statistical models based on some of the representative metabolites were considered to have good performance in distinguishing patients with active IBD from those in remission or in identifying responders from nonresponders during treatment. Much of this evidence shows that high-throughput and high-sensitivity metabolomics technology not only allows for the quantification of small changes in a single metabolite but can also integrate the changes of multiple metabolites with the help of multivariate analysis to obtain a comprehensive judgment of metabolic characteristics. This assists in monitoring the progress of the disease and in evaluating the therapeutic effect, which has broad prospects in the clinical management of IBD.
Although previous studies showed the promising role of metabolomics in the personalized management of IBD, more efforts are warranted for adopting metabolomics in real-world medicine. On one hand, the predictive ability and generalization of established metabolomic profiles need further validation in research with large sample sizes because of the numerous variables in the metabolomic profiles and the heterogeneity of IBD. On the other hand, the mechanisms of metabolite alteration in IBD patients with different disease activity or prognosis should be elucidated through basic research or multiomics studies, so that clinicians can perform a more targeted management with a profound interpretation of metabolomic profiles. Fortunately, the fact that metabolomics can be applied in clinical practice has been supported by the routine employment of the targeted metabolomic profiling of some metabolites, such as steroids, organic acids, amino acids, biogenic amines, and acylcarnitines, in newborn screening, especially in detecting inborn metabolism errors.85–88 Furthermore, metabolomics also exerts an important role in personalized medicine with respect to diabetes and cancer. 78 All of these applications in other fields provide references for the clinical establishment of metabolomics in IBD. It is believed that the adoption of metabolomics in practical medicine of IBD will be witnessed in the near future.
Footnotes
Author contributions
SZ is the guarantor of the article. SZ, MC, and LL designed the study and revised the review. RC and JZ wrote and revised the manuscript. SZ, CL, KC, and ZZ revised the contents of the manuscript. All authors approved the final manuscript and agreed to be responsible for this review.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the National Natural Science Foundation of China (Nos 81630018, 82070538, 81870374, 82000520), Guangzhou Science and Technology Department (No. 202002030041), and Guangdong Science and Technology Department (Nos 2017A030306021, 2020A1515010249)
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.