
Abstract
Clostridioides difficile infection (CDI) is a consequence of flagrant use of antibiotics, an aging population with increasing comorbidities, and increased hospitalizations. The treatment of choice for CDI is antibiotics (vancomycin or fidaxomicin), with a possibility of recurrent CDI despite lack of additional risk factors for CDI. For the last 10 years, fecal microbiota transplantation (FMT) has emerged as a promising therapy for recurrent CDI, with success rates of over 85% compared with less than 50% with antibiotics for multiple recurrent CDI. Along with the success of FMT, several adverse and serious adverse events with FMT have been reported. These range from self-limiting abdominal pain to death due to severe sepsis. This review focuses on the safety of FMT, emphasizing the reports of transmission of pathobionts like extended-spectrum beta lactamase Escherichia coli and Shiga toxin-producing E. coli. The severe acute respiratory syndrome coronavirus-2 is a potential pathogen that could be transmitted via FMT during the COVID-19 pandemic. The challenges faced by clinicians for donor screening, clinical trials, and other aspects of FMT during the pandemic are discussed.
Introduction
Clostridioides difficile infection (CDI) is the most prevalent healthcare-associated infection, not only in the USA, but across the whole world.1,2 From debilitating diarrhea to pseudomembranous colitis to toxic megacolon and fatal sepsis, CDI is associated with significant morbidity and high mortality. With an annual case burden of 223,900 cases in the USA, high rates of hospitalization, 12,800 deaths annually, and US$1 billion attributable costs, CDI is classified as an ‘urgent’ threat level by the US Centers for Disease Control and Prevention. 3 A major complication attributed to CDI is a high risk of recurrence (defined as a subsequent episode of CDI occurring within 8 weeks of a previous episode), usually without exposure to additional risk factors.4,5 The most important risk factor for recurrent CDI is recent CDI. With each subsequent episode, the rate of recurrence further increases. The estimated recurrence rate after the first episode is 20–25% and increases up to 60% after the third episode.6,7 In a study using an administrative database from 2001 to 2012, the incidence of primary CDI increased by 42.7% compared with a 188.8% increase in recurrent CDI. 8 Diagnosing CDI can also be a clinical challenge due to the high sensitivity of nucleic acid-based testing modalities. About 20% of patients who recover from CDI suffer from postinfection irritable bowel syndrome. 9 Testing patients who do not have CDI symptoms increases the rates of clinical false positives and over-treatment of CDI. 10
Management of CDI
Due to these considerations, an aging population with greater comorbidities and CDI affecting younger community dwellers, the treatment of CDI remains a clinical challenge. For a nonsevere first episode, either vancomycin or fidaxomicin are preferred (metronidazole may be used if these are not available). For a first severe episode either vancomycin or fidaxomicin are recommended. For a fulminant infection, a combination of high-dose vancomycin and intravenous metronidazole are used. For a first recurrence, either fidaxomicin (if vancomycin was used for the initial infection) or vancomycin (if metronidazole was used for the initial infection) should be prescribed. Another option is a pulsed and tapered vancomycin regimen 11 (Figure 1).

Standard pharmacologic management of Clostridioides difficile infection. A suggested regimen for vancomycin taper is as follows: 125 mg orally four times daily for 10–14 days, 125 mg orally two times daily for 7 days, 125 mg orally once daily for 7 days, and 125 mg orally every 2 or 3 days for 2–8 weeks. A rifaximin chaser regimen involves vancomycin 125 mg orally four times daily for 10 days followed by rifaximin 400 mg three times daily for 10 days.
For multiple recurrent CDI (three or more episodes) or refractory CDI (nonresponsive to medications), fecal microbiota transplantation (FMT) is recommended.11–13 This therapeutic modality restores a patients’ dysbiotic gut microbiome by transferring microbes from a stool of a healthy donor to a patient with recurrent CDI. A clinical trial from Europe compared vancomycin followed by FMT to fidaxomicin or vancomycin as treatment for recurrent CDI and demonstrated 92% success rates with FMT compared with 42% with fidaxomicin and 19% with vancomycin. 14 Another trial including patients with refractory CDI showed a 75% cure of refractory CDI with a single FMT infusion and 100% cure with multiple infusions. 15 FMT is cost effective and increases quality of life years (QALY) (and reduction in cost/QALY ratio) in patients compared with antibiotic treatments.16–18 A systematic review and meta-analysis of 7 randomized control trials and 30 case series showed resolution of symptoms in 92% of the patients who underwent FMT. 12 A systematic review and meta-analysis which included all studies on FMT until November 2019 showed that at 8 weeks post-FMT, a single dose had a efficacy of 84% [95% confidence interval (CI): 80–88%, I2 = 86%]. Repeat FMT was 91% (95% CI: 89–94%, I2 = 53%) effective. 19 It also concluded that delivery by lower gastrointestinal endoscopy was the most superior delivery method and repeat FMT significantly increased treatment efficacy. Another meta-analysis measuring the efficacy of oral FMT capsules showed 82.1% efficacy (95% CI: 76.2–87.4%) in preventing recurrent CDI. 20 In addition, FMT has also been associated with reduced bloodstream infections, shorter hospital length of stay, and a higher survival compared with patients receiving antibiotics for CDI. 21 The US Food and Drug Administration (FDA) classifies FMT as an experimental therapy.
It is important to ponder on the safety aspects of FMT. We have seen inadvertent consequences of advances in medicine such as hepatitis C transmission with blood transfusions. Newer therapies such as FMT should be carefully monitored for adverse events and potential long-term consequences. It is of the utmost necessity that FMT is carried out in a standardized manner with thorough donor screening and testing to prevent adverse events. The FDA has an enforcement discretion policy allowing the use of FMT to treat CDI not responsive to standard therapies (Table 1). 22 Below, we summarize the recent safety challenges associated with FMT and the impact of the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) pandemic on FMT for CDI.
Enforcement discretion policy regarding IND for FMT.

FMT, fecal microbiota transplantation; IND, investigational new drug.
Adverse events after FMT
Most commonly after FMT patients develop mild symptoms such as abdominal pain, cramping, bloating, nausea mild fever, and constipation, which tend to be self-limited.23–30 There may be a risk of a disease flare post-FMT for CDI in patients with underlying inflammatory bowel diseases.26,28 A case of unintentional weight gain of 41 pounds in 36 months after receiving FMT from an overweight donor has been reported, but the causality between FMT and obesity was not proven in larger studies.31,32 Autoimmune diseases post-FMT have been reported. 33 Reports of aspiration following sedation used during an FMT procedure have been described.26,34 Toxic megacolon after FMT has been reported.35,36 In a study performed on patients with liver cirrhosis undergoing FMT, five serious adverse events were documented and classified as possibly related to the FMT. These were Crohn’s disease flare, fecal urgency, dehydration with acute kidney injury, worsening hepatic encephalopathy, melena, and anemia in a patient of portal hypertensive gastropathy post-FMT. 37 Another study from the FMT national registry showed two infections possibly related to FMT: Bacteroides fragilis bacteremia in one participant, enteropathogenic Escherichia coli on a multiplex polymerase chain reaction (PCR) stool panel in another. 38 A detailed risk stratification of side effects from several studies is outlined in Table 2.
Adverse effects and risk stratification of FMT.
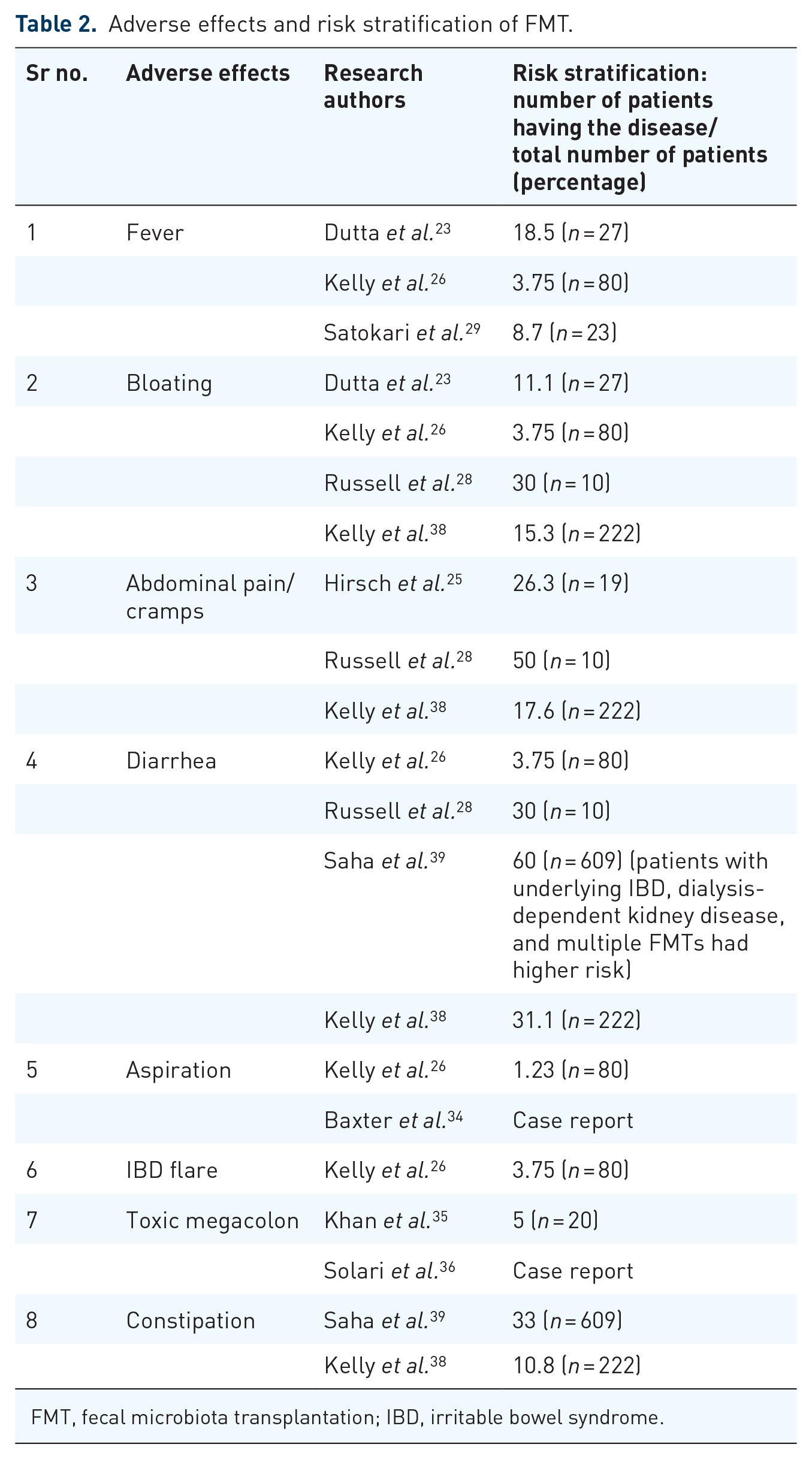
FMT, fecal microbiota transplantation; IBD, irritable bowel syndrome.
Lack of standardization of FMT
There have been case reports where improper knowledge and standardization of donor screening has led to side effects.40,41 Expert opinion and evidence-based donor screening protocols have been proposed to standardize donor screening processes.42,43 These protocols suggest that the screening should be a four-step process. The first step should consist of a prescreening survey (for assessing general health, risk of infectious diseases). It should be followed by a clinical assessment (to exclude risk factors for transmissible disease and potential microbiome-mediated conditions), stool and nasal screening [including carbapenem-resistant Enterobacteriaceae, extended-spectrum beta-lactamase-producing (ESBL) organisms, and methicillin-resistant Staphylococcus aureus besides other standard organisms], and serological screening (abnormal blood counts, liver tests, and infectious pathogens). In addition to this protocol, geographic areas should also have alterations in the screening protocol according to their local infectious disease epidemiology.
A systematic review of 85 studies demonstrated a significant heterogeneity in the reporting of different aspects of FMT. In this study, 83 of the 85 (98%) did not describe the material used for collecting stools or the preparation of donors for collecting stools. Most [n = 76 (89%)] did not specify the methods of dilution and homogenization or filtration of stools. In 82 reports (96%), the authors did not describe under what conditions stools were prepared or methods used for conservation of stools. Overall, 68 (80%) did not describe the type of stools used for infusion (e.g. fresh or frozen), volume of preparation, the amount of stool used, or duration of conservation of stools. A total of 51 reports (60%) did not specify the preparation of patients for transplantation, mode of administration of infusion, or number of infusions per patient. 44 Many preparations and methods of instillation of FMT, such as nasogastric, nasoduodenal, and colonoscopic, are used in clinical practice. One study carried out in 2013 used synthetic stool, that is, purified intestinal bacterial cultures derived from a single healthy donor stool. It was used to treat recurrent CDI in two patients who failed standard antibiotic treatment. This stool substitute preparation was given via colonoscopy. Both patients showed formed bowel movements within 1–3 days. They did not show any recurrence of CDI/loose stools at 24 weeks postprocedure even after receiving numerous antibiotics for recurrent urinary tract infections and skin infections within these 24 weeks. 45 In addition, standardized therapies which are enema-based (RBX2660) or capsule-based therapies (SER-109, CP101, RBX7455, VE303) are being developed.11,14,33,46–53 Details on these novel microbiome-based therapies are outlined in Table 3.
Novel microbiome restoration therapies.

Serious infection transmission associated with FMT
In 2019, two immunocompromised patients were reported to have contracted ESBL E. coli infection after FMT from a common stool donor. 41 The donor was not tested for the presence of ESBL E. coli and this screening was made standard practice after these instances. One patient with end-stage liver disease was administered FMT via oral capsules for hepatic encephalopathy as part of a clinical trial. The patient developed cough, fever, and chest infiltrates suggestive of pneumonia 17 days after FMT. Fluoroquinolone treatment led to no clinical improvement and blood cultures demonstrated Gram-negative bacilli identified as ESBL E. coli. He was managed with a carbapenem with eventual resolution. The second patient had undergone hematopoietic stem-cell transplantation for myelodysplastic syndrome. The patient was given FMT as part of a clinical trial to prevent graft versus host disease. On day 8 after FMT, he developed fever, chills, and altered mental status progressing to hypoxia. Blood cultures demonstrated Gram-negative bacteremia with ESBL E. coli. Despite treatment with a carbapenem, he died 2 days later from severe sepsis. On further investigation, both bacterial isolates had a similar antibiotic resistance pattern and the same multilocus sequence type 131 and serotype O25:H4. The single nucleotide polymorphism (SNP) analysis of the bacterial samples from the patients and the donor stool sample showed SNP similarities suggesting transmission from the same donor. A few other patients who received capsules derived from this donor’s stool showed ESBL E. coli in their stools but they did not suffer from bacteremia despite some being immunocompromised. The FDA issued a safety alert in June 2019 regarding the use of FMT and risk of serious adverse reactions due to transmission of multidrug-resistant organisms. 63
After the consultation with the FDA on 10 March 2020, OpenBiome (a non-profit stool bank in USA) started testing all donor stool prospectively for Shiga toxin type 1 and type 2 producing genes (stx1/2) by nucleic acid amplification testing rather than enzyme immunoassay. 64 This was a result of adverse events due to infectious transmission. 40 In February 2020, OpenBiome received reports of two patients developing abdominal pain and diarrhea after FMT who had received stool from the same donor. Stool from a stored aliquot of this donor was positive for the stx1/2 genes (the genes responsible for producing Shiga toxin type 1 and type 2). Six serious adverse events (diarrhea and abdominal pain) and one non-serious adverse event were reported. There were two deaths but these were eventually determined to be unrelated to FMT. 40 All stored stool samples from this donor underwent both PCR and enzyme immunoassay (EIA) testing. Out of 20 samples tested, 11 were positive via PCR but were negative via EIA (which was used as the initial mode of screening by OpenBiome), suggesting that PCR has higher sensitivity than EIA in this setting. The donor and one available patient isolates were assessed for clonality and isolates were deemed to belong to the same serotype H7:O117 and were clonal (0–1 SNP differences between the two donor isolates and 0–6 SNPs between the donor and the patient isolate). Isolates with a distance of less than 10 SNPs are considered to be a part of a transmission cluster.65–67 This event emphasizes the importance of using a method of high-sensitivity testing rather than low-sensitivity testing for donor screening as donors are asymptomatic. This event suggests the importance of strong surveillance and quality measures to establish causality.
A 19-year-old man with primary immunoglobulin A deficiency status underwent FMT via colonoscopy for recurrent CDI with stool sourced from a commercial stool bank. At 10 days after FMT, he presented with explosive bloody diarrhea with 20 bowel movements a day, leukocytopenia, fever, chills, and night sweats. Stool was examined and found positive for enteropathogenic E. coli, enterotoxigenic E. coli, and Shiga toxin-producing E. coli. 68 These events emphasize the need to practice caution whenever FMT is carried out in an immunocompromised patient.
A study investigating fecal specimens from 66 recipients and the RBX2660 product in a multicenter, randomized, double-blind, placebo-controlled phase IIb study showed that RBX2660 not only shifted the taxonomic structure of the intestinal microbiome in the recipient group, but it also lead to dynamic changes in their antibiotic resistance patterns. 69 Besides decreasing the overall antibiotic resistance in the microbiome, it also simultaneously introduced RBX2660-origin antibiotic-resistant genes (ARGs) in a dose-dependent manner. This emphasizes the importance of screening fecal transplant samples for medically important ARGs via highly sensitive molecular methods.
Considering unintentional pathogen transmission via FMT and the lack of protocols to test asymptomatic recipients, it is indubitably true that the donor screening is still an imperfect science which will continue to be iterative over time. The COVID-19 pandemic increases the complexity of donor screening. There have been reports of SARS-CoV-2 shedding in stools of asymptomatic patients and in post-COVID recovery patients (who are negative on respiratory testing).70,71 There are no validated stool assays available for asymptomatic or symptomatic people. According to the recent guidance from the FDA for studies performing FMT under an investigational new drug application, donor stool obtained and banked before 1 December 2019 must be stored separately from the stool donated and stored after 1 December 2019. 72 In this era, a more cautious approach is warranted. In order to consider a person to be a stool donor, travel history, contact with a recent symptomatic individual, past history of COVID-19 infection, and symptoms suggestive of COVID-19 should be added in the screening questionnaire. Donors donating stool after December 2019 should be screened for COVID-19 symptoms and exposure. Donors who pass the screening should undergo COVID-19 testing along with the usual donor screening. Rescue FMT should be used in fulminant patients with no response to initial antibiotic treatment. If the symptoms improve, the antibiotic dosage should be tapered to the lowest effective dosage and should be continued until the COVID-19 pandemic is over. 72 Considering the heavy impact COVID-19 had on our healthcare and economy, an improved approach should be in place for managing patients with recurrent CDI during the COVID-19 era.73,74 The largest stool bank in the USA, OpenBiome, has ceased operations as of the time of writing this manuscript. If FMT is not available, prolonged courses of antibiotics such as vancomycin at their lowest effective dosage may be used as the treatment of choice in those with multiple recurrent CDI and FMT performed once available.
Challenges and opportunities in 2020 and beyond
The future of microbiome restoration therapies is exciting. Besides patients with CDI, FMT has been effective in a different spectrum of patients.75–78 There is emerging evidence which supports the association of dysbiosis and autoimmunity, metabolic diseases, etc., suggesting a role of microbiota restoration to treat diseases beyond FMT.79,80 FMT is being explored for obesity, nonalcoholic steatohepatitis, primary sclerosing cholangitis, and autism.75–78 Methodologies for stool treatment to eliminate viral or bacterial pathogens and synthetically grown defined microbial consortia would avoid the risk of transmitting pathogens, including SARS-CoV-2.
The Infectious Disease Society of America/Society of Healthcare Epidemiology of America 2017 guidelines recommended FMT for multiple recurrent CDI despite “moderate quality” evidence, reflecting the great unmet need. 13 Recently, two large phase III studies of standardized microbiome-based therapies have shown positive initial results and final results are awaited.81,82 Availability of these products will help further streamline access to FMT and help minimize side effects. FMT-maintained remission of CDI larger treatment trials are needed to prove its efficacy in treating an acute onset CDI. Designing and rationalizing trials for evaluating FMT’s efficacy in these diseases would be a challenge. These Covid-19 times provokes us to sharpen our imperfect donor screening so that pathogenic organism transmission could be prevented.
There remain diagnostic challenges for CDI in 2020. Stool EIA (rather than PCR) should be used to include or exclude patients in clinical trials as PCR has high rates of false positivity for recurrent CDI. 83 Using PCR for diagnosis raises the question of whether the patient was really suffering from recurrent CDI or the diagnosis was a false positive.
In conclusion, CDI is a very rampant disease in hospital settings and FMT helps prevent recurrent CDI. It has previously been thought to have an excellent safety profile. More recently, transmission of Shiga toxin-producing E. coli and ESBL-producing E. coli emphasizes the importance of a comprehensive and universal screening protocol and standardization of FMT to mitigate adverse events in the future. As FMT is considered an experimental therapy and donor screening is an imperfect science, protocols should be in place to back trace the stool aliquots so that causalities can be established in future. The COVID-19 pandemic has made FMT increasingly challenging. The availability of standardized microbiome-based therapies will help to mitigate risks from FMT even further.
Footnotes
Conflict of interest statement
SK has received research grants from Rebiotix Inc. and consulting fees from Shire, Premier Inc., Facile Therapeutics, and Probiotech International, outside of the submitted work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.