
Abstract
Treatment targets of inflammatory bowel diseases (IBD), ulcerative colitis (UC) and Crohn’s disease (CD) have evolved over the last decade. Goals of therapy consisting of symptom control and steroid sparing have shifted to control of disease activity with endoscopic remission being an important endpoint. Unfortunately, this requires ileocolonoscopy, an invasive procedure. Biomarkers [C-reactive protein (CRP) and fecal calprotectin (FCP)] have emerged as surrogates for endoscopic remission and disease activity, but also have limitations. Despite this evolution, we must not lose sight that CD involves transmural inflammation, not fully appreciated with ileocolonoscopy. Therefore, transmural assessment of disease activity by cross-sectional imaging, in particular with magnetic resonance enterography (MRE) and intestinal ultrasonography (IUS), is vital to fully understand disease control. Bowel-wall thickness (BWT) is the cornerstone in assessment of transmural inflammation and BWT normalization, with or without bloodflow normalization, the key element demonstrating resolution of transmural inflammation, namely transmural healing (TH) or transmural remission (TR). In small studies, achievement of TR has been associated with improved long-term clinical outcomes, including reduced hospitalization, surgery, escalation of treatment, and a decrease in clinical relapse over endoscopic remission alone. This review will focus on the existing literature investigating the concept of TR or residual transmural disease and its relation to other existing treatment targets. Current data suggest that TR may be the next logical step in the evolution of treatment targets.
Introduction
Inflammatory bowel disease (IBD) is a group of complex, chronic, immune-mediated diseases with increasing incidence around the world. 1 The two main diseases, Crohn’s disease (CD) and ulcerative colitis (UC) occur with a prevalence of 30–300/105 and 70–500/105 in Western countries affecting both sexes equally, with onset usually in early adulthood but can be diagnosed throughout life, with increasing severity with early onset. 2 The underlying pathophysiology remains poorly understood; however, is believed to be caused by an interplay of factors such as environmental exposures, intestinal microflora and genetic susceptibility, leading to a dysregulated intestinal immune response and altered epithelial barrier function. 3
CD has a progressive disease course ranging from an inflammatory phenotype to stricturing and penetrating disease over time, which is often associated with an increased need for surgery, morbidity and even mortality. 4 CD can lead to repeated need for hospitalization and/or surgery, contributing to impaired quality of life, and in severe cases, disability. Overall, the burden extends beyond the individual with a significant direct and indirect healthcare cost for society. 5
Therapeutic options have expanded over the last 2 decades with increased use of immune modulators and the emergence of monoclonal antibodies to tumor necrosis factor (TNF) alpha, the interleukin (IL)12/23 pathway, and integrins on the surface of leukocytes. Therapies aimed at novel targets, as well as those aimed at treating fibrosis, are on the horizon. New treatment options have led to better control of symptoms, endoscopic remission, as well as improved quality of life, decreased hospitalization, and surgical rates. Despite this, irreversible bowel damage continues to be a problem, which begs the question of whether we have a robust enough therapy, or perhaps our treatment goals need to be expanded to truly change the natural history of the disease.
The current review focuses on the current concept transmural remission (TR) in CD in relation to established treatment goals. Potential advantages and future perspectives of TR will be discussed, as well as current limitations. Even though UC may be regarded as transmural disease as well, the data on TR in UC are scarce. This review is therefore focusing on TR in CD.
The current state of treatment targets and their limitations
Management strategies for CD treatment have evolved, moving from a purely clinical-symptom-driven strategy, toward a ‘treat to target’ approach. 6 ‘Treat to target’ involves objective monitoring and tight disease control. There is growing evidence suggesting accurate, frequent, objective evaluation of disease to direct treatment decisions, achieves better outcomes and avoids further intestinal damage, hospitalization, or surgery. 7
Disease management by symptom control
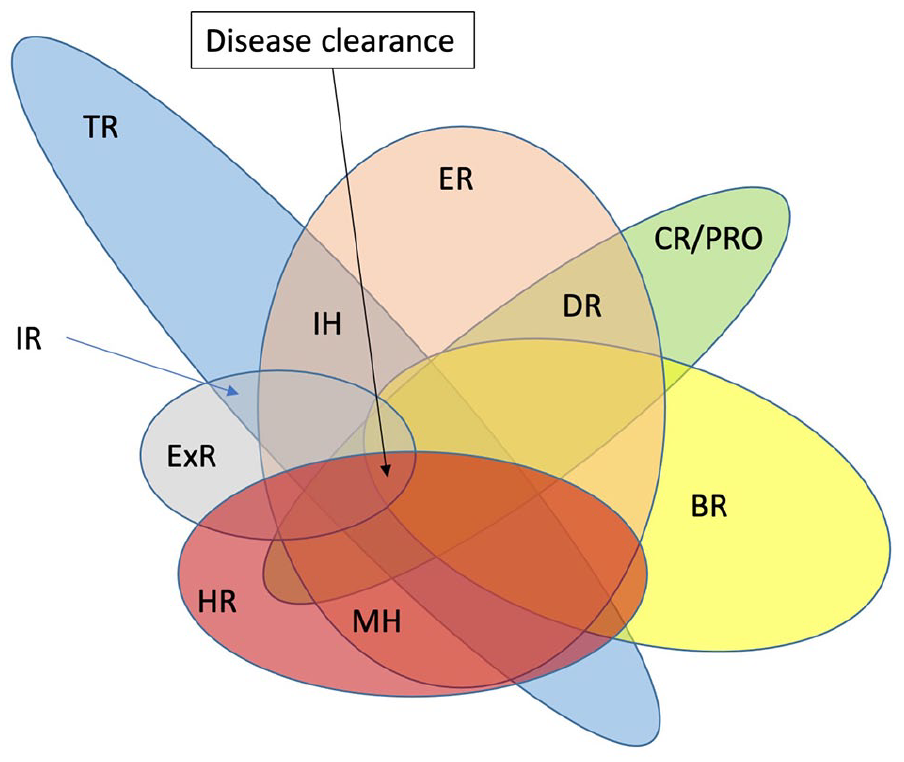
Symptom control will always be important to patients, as symptoms reflect their day-to-day disease experience and quality of life. Given the established discordance between symptoms and intestinal inflammation, treatment decisions focused solely on symptom control can result in over-/undertreatment.8,9 Irrespective of the disease entity, subclinical inflammation often persists, resulting in progressive structural damage and potentially disabling complications. 10 The CD Activity Index (CDAI) has been used as standard measure for clinical trials for decades, heavily weighted with subjective clinical symptoms. The accuracy of the CDAI to predict endoscopic healing is low in patients with CD. In addition, CD patients in clinical remission (CR) may not achieve C-reactive protein (CRP) normalization and/or endoscopic remission (ER), as previously demonstrated for steroids and other therapeutics.11,12 Similar observations have been made in the SONIC trial, where half the patients treated with azathioprine and/or infliximab in CR had endoscopic and/or CRP evidence of residual active CD, whereas other patients with endoscopic and CRP normalization had persistent symptoms. 13 The CDAI does not include objective measures of inflammation such as CRP or endoscopy. 14 The evolution of therapeutic goals reflects the recognized importance of objective measures of inflammation, while recognizing the value and importance of patient-reported outcomes (PROs); however, PROs cannot be used as the sole therapeutic goal (Figure 1).

Evolution of treatment targets.
Monitoring disease with biomarkers
Biomarkers such as CRP and fecal calprotectin (FCP) have gained prominence as non-invasive tools used to monitor disease activity. Although CRP indirectly reflects inflammation, it correlates better with the endoscopic disease compared with CDAI.15,16 CRP has some limitations: normalization does not always correlate with complete resolution of symptoms or intestinal inflammation. 17 False negative results occur in up to 20% of patients, particularly in patients with small-bowel involvement and those with proctitis. 18 Similar to CRP, FCP may normalize after therapy despite the fact that endoscopic inflammation can still be detected. 17
FCP is considered part of a standard monitoring regimen for CD, despite the absence of clear, agreed-upon thresholds for definitive activity, it has been shown to respond to therapy and to predict relapse better than CRP. 19 There are, however, recognized limitations, most important of which is that colonic disease activity is better predicted compared with small-bowel or more proximal disease. 20
Endoscopic remission as a treatment goal
The terms ER and mucosal healing (MH) are used as synonyms with inconsistent definitions in the literature. However, ER is used for the endoscopic evaluation, and MH now includes ER combined with histologic remission (HR).21,22 For consistency, we use the term ER in the current review, where MH has been used as a synonym in the literature (Table 1, Figure 2). As gastroenterologists trained in endoscopic evaluation, IBD activity is intuitively graded through the lens of the endoscope. Accordingly, resolution of activity suggests disease control. ER is best defined as an absence of ulcers in CD, since this has been shown to reduce the likelihood of clinical relapse, reduce the risk of surgery and hospitalization.23,24 The contribution of HR is less clear in CD, but HR in ileal disease may also be an important predictor of outcome. 25 In a ‘treat to target’ strategy in CD (STRIDE), deep remission has become the therapeutic goal. 6 Deep remission includes clinical (steroid-free)/patient-reported outcome remission (defined as resolution of abdominal pain and diarrhea) and ER (i.e. ER, defined as resolution of ulceration at ileocolonoscopy), or resolution of findings of inflammation on cross-sectional imaging in patients who cannot be adequately assessed with ileocolonoscopy. A revision of the STRIDE guidelines (STRIDE II) has recently been published, 21 suggesting a three-step approach that includes clinical response as an immediate treatment target, CR, and normalization of CRP and FCP as intermediate treatment targets, and finally, ER and absence of disability and normalized health-related quality of life as long-term treatment targets. ER may also not sufficiently reflect the transmural and peri-intestinal or extramural inflammatory burden of CD.21,26 Although this is acknowledged in the new guidelines, imaging outcomes are endorsed as an important adjunct to ER that should be considered but is not currently considered a formal target. 21
Proposed terminology for types of remission (R) and their common definition. 27 .

BWT, bowel-wall thickness; CDAI, Crohn’s Disease Activity Index; CDEIS, Crohn’s Disease Endoscopic Index of Severity; CRP, C-reactive protein; FCP, fecal calprotectin; HBI, Harvey Bradshaw Index; LN, Lymph Nodes; MaRIA, a validated weighted MRE segmental score depending on relative contrast enhancement between baseline scan and 70 s; NHI, Nancy Histological Index; RHI, Robarts Histopathology Index; TI, Terminal ileum; SES-CD, Simple Endoscopic Score for Crohn’s Disease.
Proposed terminology for types of remission and their common definition.
Taken together, with several limitations of the existing targets outlined above, the question remains whether ER is still a sufficient endpoint, as CD is a transmural disease where damage can persist despite the presence of ER at endoscopy. 30 In a recent prospective study of children with CD, one third of patients had healing of the mucosa or the bowel wall, but not both. 31 Furthermore, in another study on pediatric CD patients, almost every fourth patient with ER showed signs of transmural inflammation. 32 It remains questionable whether ER adequately mirrors complete resolution of inflammation known to be systemic. 33 Therefore, more inclusive TR may be a more appropriate therapeutic goal than ER.34–36 Hence, TR defined as the resolution of not only mucosal ulcerations but also of trans- and potentially extramural-disease-related alterations might represent a more stringent target in routine medical practice.34–38
Evaluating transmural disease activity
There are three different cross-sectional imaging methods routinely used to measure transmural disease activity: computed tomography ± enterography (CT/E), magnetic resonance enterography (MRE), and IUS. A metanalysis from 2008 by Horsthuis et al. 39 could not detect a significant difference in diagnostic accuracy among these imaging methods. Mean per-bowel-segment sensitivity estimates were 73.5% for IUS, 70.4% for MRE, and 67.4% for CT, with significant gains in accuracy since this publication. The mean per-bowel-segment specificity estimates were 92.9% for IUS, 94.0% for MRE, and 90.2 Similarly, a systematic review by Panes et al. 40 found comparable results in respect to evaluation of disease activity: IUS (sensitivity 84%, specificity 92%) and MRE (sensitivity 93%, specificity 90%) with a lower accuracy for IUS for disease proximal to the terminal ileum. A more recent multicenter trial comparing the accuracy of MRE and IUS for detection of disease extent and activity in CD confirmed a high sensitivity for detecting small bowel CD with MRE [97% (91–99)] and IUS [92% (84–96)], but with less sensitivity in colonic disease, MRE [64% (50–75)] and IUS [73% (59–83)]. 41 Lemann index is designed to assess progressive disease in CD by cross-sectional imaging, and as a consequence, treatment response is less optimally assessed using this index.
When selecting the appropriate modality for transmural assessment, a number of factors need to be considered. CT for example, as reflected in ECCO-ESGAR diagnostic guideline, is not recommended for routine monitoring, or follow up of treatment response given radiation exposure, and thus should be limited to emergency situations. 42 Alternatively, MRE exhibits high accuracy and can be used for measuring treatment response. However, access, high cost, and the need for preparation (oral and intravenous) contributes to diminished patient preference and may limit the use of MRE for frequent and short-term follow up, to measure transmural response and activity. IUS in contrast, does not require any preparation, can be performed in a point-of-care setting directly by the treating gastroenterologist, is less time and cost intensive, and allows direct interaction with the patient improving compliance. 43 Therefore, when considering all the pros and cons, IUS appears to be the most promising cross-sectional imaging method for routine monitoring of transmural activity in cross-section. However, lack of local expertise may be a challenge. 44
Exploring definitions of transmural remission and transmural response
Changes to the small and/or large bowel wall and possibly the surrounding mesentery in response to treatment, present attractive therapeutic targets. This section will review current definitions of radiologic response and healing in CD. A review of the limitations of current definitions will be outlined. The terms transmural healing (TH) and TR are used as synonyms with inconsistent definitions in the literature. For consistency, we use the term TR in the current review.
The parameters central to CD activity on imaging, and thus response, are largely common to all imaging modalities. The most important and reliable parameter with the strongest prediction of disease activity and response is bowel-wall thickening45,46 (BWT) as seen on CT, MRE, or IUS (>3 mm being the most common threshold for pathology), measured in the most affected part of the bowel36,45,47–54 (see Figure 3 for TR defined by IUS). However, BWT may reflect both active and chronic (fibrotic or muscular hypertrophy/-plasia) disease. 55 Within the thickened bowel wall, additional mural changes that may respond to therapy can be assessed in a semiquantitative or qualitative manner. These pathological findings include bowel-wall edema, represented by T2 hypersignal on MRE, and presence/absence of bowel-wall stratification (BWS) on IUS.36,54,56 Other structural findings like ulcers are described on MRE 57 and IUS as protrusions in the bowel wall or focal loss of stratification.55,58 Increased blood volume in the bowel wall can also be assessed semiquantitatively or as relative perfusion changes using both MRE and contrast-enhanced IUS. However, this presents technical challenges55,59 and as a consequence, a more qualitative assessment describing intensity and layers with enhancement 60 or an ordinal evaluation of detected vessels by color Doppler imaging on IUS can be used.54,56,61–63 Proliferation of inflammatory mesenteric tissue (inflammatory fat) is clearly seen as a bright mass-like formation that abuts the mesenteric serosal layer. On MRE/CT there is a higher signal on T2, and scattered areas of enhancement. The extramural findings of enlarged mesenteric lymph nodes and peri-enteric free fluid reflect disease activity; however, with less significant, consistent contribution to disease activity. 64
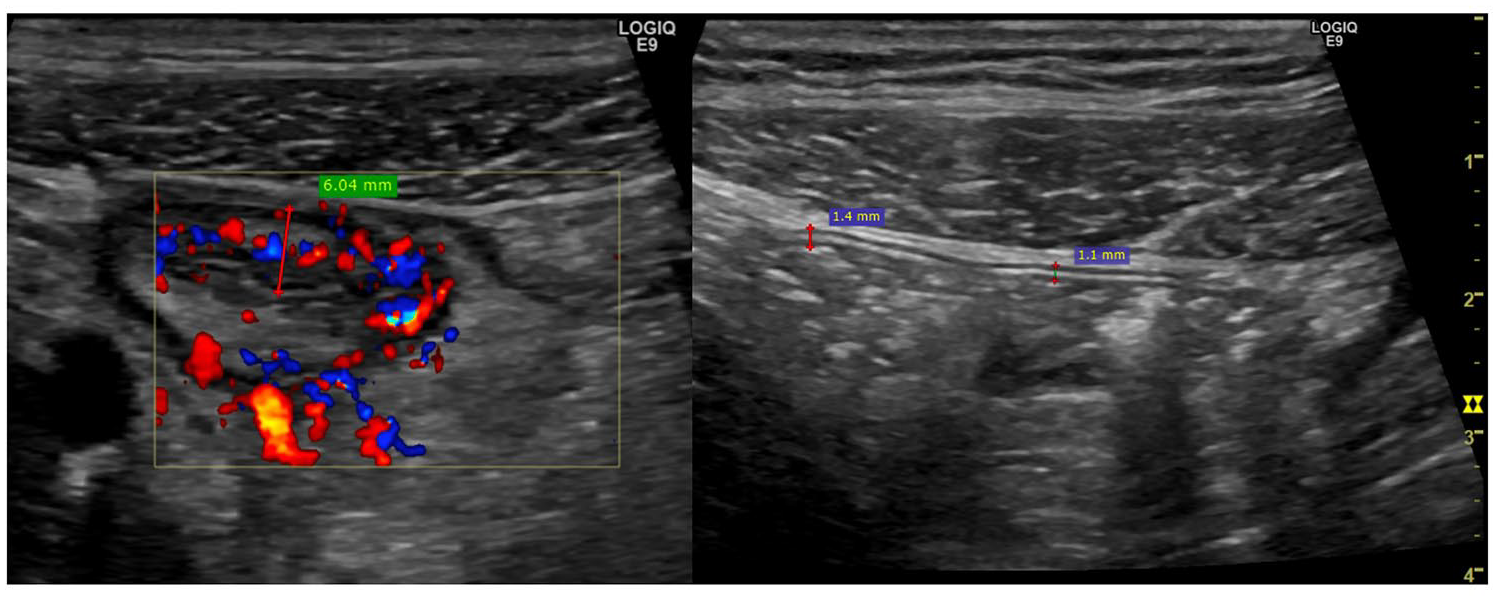
Example of achieved transmural remission in a 19-year-old male.
Response and remission may be defined by either change noted in individual activity parameters, or by composite indices reflecting activity and responsiveness to therapy (Table 2). A number of activity indices have been developed for IUS, with a number of limitations including lack of prospective validation and/or responsiveness to therapy.45,65 Similarly, MRE indices exist, with at least partial validation and responsiveness (Table 2).
Response definitions for studies investigating transmural remission.

Residual abnormal enhancement with improvement in BWT and recovery of normal T2 signal was determined to be resolution of the active inflammation but with underlying fibrosis, and thus would be classified as no active inflammation.
Active inflammation [enhancement, length, dilated vasa recta/Comb sign, peri-enteric inflammation (edema, phlegmon, or abscess)], or fistulizing (internal penetrating) disease.
BWT >3 mm, stenosis, Target sign, Comb sign, lymphadenopathy, abscess, fistula, sinus tract, fibrofatty proliferation, peri-enteric stranding, free fluid.
BWT >7 mm, bowel wall or segmental post-gadolinum hyperintensity (T2 weeks) compared with normal small bowel, lymphadenopathy, Comb sign, Stricture, Fistula, Abscess.
Ulcerations (1), ADC (ΔADC >+10%) (1), RCE (ΔRCE >−30%), enlarged (1), lymphadenopathy (1), sclerolipomatosis (1; inflammatory fat).
BWT >3 mm, mural hyperenhancement, mesenteric fat proliferation, mesenteric fat densification, Comb sign, strictures (luminal narrowing and upstream dilatation >30 mm).
Scoring from International Bowel Ultrasound Group Segmental Activity Score: 54 color Doppler signal (CDS) range 0–3, BWS range 0–3.
CDAI 14 is the Crohn’s Disease Activity Index, a weighted summarized score based on clinical [# of liquid/very soft stools/week × 2, abdominal pain (0–3 × 5), general wellbeing (0–4 × 7); extra intestinal/systemic manifestation (0–6 points total × 20); anti-diarrheal medication (0–1 × 30); laboratory markers (hematocrit level below normal × 6); abdominal mass (0/2/5 × 10); and weight loss (kg × 0.5)].
PGA is the Physician Global Assessment.
HBI 80 is the Harvey Bradshaw Index: a non-weighted summarized score based on ordinal assessment of clinical [general wellbeing (0–4); abdominal pain (0–3); #liquid stools/day; abdominal mass (0–3); complications (0–8)].
SES-CD score 81 is the Simple Endoscopic Score for Crohn’s Disease, a non-weighted ordinal summarized point score with ordinal grading (0–3) of ulcer size, ulcerated surface, affected surface, and presence of narrowings.
SEAS-CD score 82 is the Simple Enterographic Activity Score for Crohn’s Disease, a non-weighted, non-validated summarized point score with ordinal grading (1–3) for extent of disease in small bowel; (0–2) for BWT, contrast enhancement, fat wrapping, proliferation of mesenteric vasculature, mesenteric lymphadenopathy, ulcerations, stenotic complication; and (0–1) for intra-abdominal fistulas.
CDEIS 83 is the Crohn’s Disease Endoscopic Index of Severity, a weighted summarized index for five intestinal segments (rectum, sigmoid and left colon, transverse colon, right colon, ileum) each segment scored for deep ulceration (12), superficial ulceration (6), disease involvement (surface in cm), ulcerated surface (cm).
The Nancy Score is a non-weighted summarized score for six segments (rectum, sigmoid, left colon, transverse colon, right colon, and terminal ileum): (0–1) for ulceration, parietal oedema, BWT >3 mm, differentiation between [sub]mucosa and muscularis propria, rapid contrast enhancement, and DWI hyperintensity.
MaRIA 84 is a validated weighted MRE segmental score depending on relative contrast enhancement (RCE) between baseline scan and 70 s: MaRIA (segment) = 1.5 × WT (mm) + 0.02 × RCE + 5 × edema + 10 × ulceration.
London Index 64 (acute inflammation scoring) = 1.79 + 1.34 mural thickness (0–3) + 0.94 mural T2 score (0–3).
ADC, apparent diffusion coefficient; BL, baseline; BWS, bowel-wall stratification; BWT, bowel-wall thickness; CD, Crohn’s disease; CRP, C-reactive protein; CT, computed tomography; CTE, computed tomography enterography; DWI, diffusion weighted imaging; IC, ileocolonoscopy; IUS, intestinal ultrasonography; MRE, magnetic resonance enterography; TH, transmural healing. T1, Longitudinal relazation time, T2, transverse relaxation time.
IUS treatment response has been clearly documented: the German TRUST study group demonstrated response in established sonographic parameters after treatment at 3 months including BWT, BWS (improvement), color Doppler signal (CDS; bloodflow), mesenteric inflammatory fat proliferation, and lymph nodes, in addition to complications (fistulae and strictures). 63 Similarly, response on IUS can be categorized, much like CT and MRE, ranging from TR to sonographic ‘improvement’ and ‘worsened’ disease. 72 Zorzi et al. 38 followed 80 patients with established CD for at least 1 year, and based on BWT, extent of disease, and presence of complications categorized patients as complete or partial responders or non-responders. Although there is still some debate about which parameter contributes most to response to treatment, there is no doubt changes in these activity parameters have been clearly documented.45,65,85
TR is most commonly defined on IUS, CT, and MRE by BWT <3 mm.7,73,86,87 Unlike some of the other parameters, the reliability of this measure is high and reduction in thickness quantifiable, while other parameters such as BWS or inflammatory fat reduction/absence can be more challenging to reliably measure changes. 54 Other imaging findings are commonly considered in the assessment of imaging remission, including absence of contrast enhancement, and reduction/resolution in inflammatory fat.53,88 One of the potential limitations to having a stringent threshold based on BWT is the potential exclusion of cases of inactive, longstanding chronic disease where thickening persists given irreversible wall changes secondary to fibrosis or muscular hypertrophy/-plasia.89–92 In the absence of active inflammation, it is unclear whether BWT above the established threshold is predictive of a poorer outcome; although Albshesh et al. 93 recently demonstrated a persistent BWT >4 mm after therapy was the only factor associated with treatment failure. Additional factors reflecting systemic disease activity are an important additional reflection of disease activity and may be an even more important indicator of pathogenic disease activity, such as mesenteric inflammatory fat. 79
In summary, current data are inconsistent and there is currently no general accepted definition for TR or transmural response.
Association of transmural disease, transmural remission, and transmural response with disease activity
Transmural disease and disease indices
The prospectively developed Simple US Score in CD (SUS-CD) correlates well (p = 0.78) with the Simple Endoscopic Score for Crohn’s Disease (SES-CD), although responsiveness has not yet been shown. 85 For MRE, additional parameters of importance are mural edema (T2 hypersignal),56,64,94,95 presence of ulcers56,94,95 and hyperenhancement, 56 diffusion-weighted imaging, 94 or fat stranding. 95 Responsiveness (against Crohn’s Disease Endoscopic Index of Severity) has been shown for both the MaRIA, 56 simplified MaRIA, 95 and Clermont score with good correlation with ER. 96
Transmural remission and mucosal healing
Discrepancies between ER and TR have been observed in several studies (see also Figure 2). Castiglione et al. 71 found 25% (17/66) in 2-year biologics maintenance therapy to achieve TR (defined as <3 mm for the entire bowel assessed with IUS) and 38% (25/66) to achieve ER. All but two with TR also had ER, K = 0.63. These findings were confirmed by the same group in a new study after 2 years of biological treatment. 34 TR occurred in 23% (9/40) on IUS and 25% (10/40) on MRE. TR was possible mainly for those with a lower SES-CD score and shorter disease duration, and rarely (16%) in strictures, and for none with penetrating disease. TR and ER correlate significantly, since all with TR also had ER. However, 13% of those with ER did not achieve TR. TR assessed by IUS is also in good agreement with TR assessed by MRE with K = 0.84, TR (IUS) and TR (MRE) versus ER K = 0.63–0.64 and ER K = 0.64 and for CRP K = 0.77–0.79 respectively. 34 Finally, in a large prospective study of 214 CD patients, Castiglione again assessed outcome after 2 years of biological treatment and found ER in 28% (60/214) and TR in 32% (68/214) in which all but two also had ER.
Applying a different perspective and approach, Rimola et al. 30 investigated 28 CD patients with severe lesions at baseline, that all achieved ER after 1 year of biological treatment (n = 14) or haemotopoietic stem-cell transplantation (n = 14). All patients had an MRE at baseline and after 1 year. Analysis was based on segments inflamed at baseline and revealed that 68% (49/72) of segments with ER also reached TR (BWT <3 mm). Authors also found significant reduction in contrast enhancement, T2 hypersignal, ulcers, fat stranding, and lymph nodes, but not in enteric fat deposition or creeping fat, that remained, to a large extent.
Changes in transmural disease activity with medical therapy
Transmural remission has been shown to occur in around 20% after exclusive enteral nutrition for 8 weeks in children. 97 These findings are not consistent though, since only 14% reached TR on biologics after 9–12 months in another pediatric cohort. Significant transmural improvement was seen in those with endoscopic response or remission for BWT, CDS, inflammatory-fat but not BWS or strictures opposed to endoscopic non-responders without any improvement. 32 Transmural improvement or response may occur fast in children, as shown by Dillman et al.98 in a study without dividing a pediatric population into responders versus non-responders, but nevertheless, finding a significant improvement to infliximab (IFX) after 2 weeks of treatment. Significant improvement was found for disease length, BWT, CDS, and mesenteric CDS, all with strong association with FCP. TR was not defined or assessed in this study. In one of the first trials investigating transmural response (defined as a 50% reduction of an MRE inflammatory score) to biologics (specifically, IFX), Van Assche et al. 88 found 40% of responders within 26 weeks of treatment and a total of 13% reached TR. In 2006 Ripollés et al. 73 investigated 51 CD patients with IUS/ contrast enhanced ultrasonography (CEUS) and found increasing response and likelihood of TR after anti-TNF therapy initiation. After 12 weeks, TH was reached in 14%, increasing to 30% at 52 weeks. In a recent, large, German multicenter IUS trial with only 20% on biologic therapy, response was assessed every 3 months, and reported, based on large versus small bowel, IUS remission defined as BWT <2 mm for terminal ileum (TI) and <3 mm for colon was reached in 25% for TI increasing to 40% after 3 and 12 months, respectively, whereas for colon, response was 20–25% at 3 months with a slight to no further increase after 12 months. 63 In the TRUST BEYOND follow-up IUS study focused on biologics and JAK inhibitors (CD and UC), segmental improvement from pathological to normal BWT (TR) occurred in 30% within 12 weeks. 99 These findings are in line with another prospective international IUS trial on ustekinumab treatment in CD, where TR was more likely to occur in large bowel 25% (16 weeks) and 50% (48 weeks) versus small bowel 5% (16 weeks) and 13% (48 weeks), respectively. 77 In a very recent MRE study assessing both MaRIA and Clermont score without specifically examining TR, improvement was found to be most prominent within the first 12 weeks of treatment for ulcer healing, oedema, reduction of BWT, Comb sign, and even complications, although Clermont and MaRIA score continued to improve slightly till 52 weeks. Mesenteric fat did not seem to improve over time. 75 From the VERSIFY study, vedolizumab multicenter phase IIIb study, TR (MaRIA <7) was achieved in 22% (7/32) after 26 weeks, and increasing to 38% (8/21) at 52 weeks, with a good association with SES-CD of r = 0.74. 100
Transmural remission as a predictor of long-term outcomes in IBD
Transmural remission and clinical activity/relapse
Eder et al. 66 followed 26 CD patients retrospectively with primary anti-TNF after induction, then followed with maintenance therapy for a total of 1 year. Major outcome definitions were: TR (MRE: simple enterographic activity score <50% at baseline and weeks 9–12); ER (in this study defined as SES-CD ⩾50% reduction from baseline at weeks 9–12) and intestinal healing (IH; combination of ER and TR). After 1 year of anti-TNF therapy, therapy was discontinued for those in CR (CDAI <150) and patients were followed, for a median of 29 months [interquartile range (IQR) 14–46], to establish long-term response. Only IH 31% (8/26) was able to predict long-term response 38%, p < 0.02 (10/26), although there was a clear trend that those with clinical relapse were more likely not to achieve either ER or TR. Sauer et al. 67 investigated outcome from an MRE database including 101 children with clinical follow up >1 year after a single MRE (MRE remission = lack of active disease: pathologic BWT, abnormal T2 signal, ± hyperenhancement). With a median follow up of 2.4 years, CR was still present in 89% (32/36) with MRE remission, as opposed to 45% (29/65) in the active MRE population, as determined by physician global assessment, p < 0.001. Change in medication (anytime) also, not surprisingly, occurred more frequently in the active MRE population, p < 0.001. For IUS, the group of Castiglione et al. further continued their previous work with a recent publication, 7 where they prospectively investigated 1-year outcomes depending on treatment status after 2 years of biological therapy treatment. Patients were categorized into ‘no objective signs of healing’, ER (SES-CD ⩽2), TR (BWT <3 mm). 7 TR was achieved by 31% (and all but two also exhibited ER) after 2 years of biological treatment, as opposed to 28% achieving ER only, 41% did not achieve any healing, or no healing (NH). For all clinical outcomes, TR was superior to ER and highly superior to NH. Only switch or swap of biological therapy at 1 year was significantly lower compared with the no-treatment group. Steroid-free CR at 1 year was thus 96%, 75%, and 41% for TR, ER, and NH, respectively, p < 0.001.
Transmural remission and need for therapy intensification
Deepak et al. 78 retrospectively identified 150 CD patients with a CTE/MRE index scan and follow-up scan of more than 26 weeks combined with >1 year of total clinical follow up. Radiological response was defined as improvement (but not resolution) with reduction in length and enhancement without worsening of other parameters. With a follow up of up to 10 years, authors found a significant reduced need for rescue corticosteroids in the radiological responders (hazard ratio 0.37, p < 0.001) and partial responders (hazard ratio 0.45, p < 0.005) when compared with non-responders. In a retrospective observational study by Fernandes et al. 35 with CD patients examined with ileocolonoscopy (ulcers yes/no or Rutgeerts score ⩾i2 for active disease) and MRE (active disease if BWT >3 mm or increased contrast enhancement or complications) within 6 months apart, were followed clinically for 1 year. Diagnostic outcomes were divided into ER 24% (52/214), TH 15% (33/214), and IH (ER and inactive MRE), or NH on ileocolonoscopy 60% (129/214). More than half needed therapy escalation when NH was observed, which was significantly worse than those with ER (37%, p = 0.023) or TR (15%, p < 0.001). TR also performed significantly better than only ER (p = 0.023). Hallé et al. 69 retrospectively reviewed medical records of patients with CD. They identified 115 patients with two successive MRE scans within 3–12 months with clinical follow up for ⩾1 year. Radiological responders were compared for outcome measurements with non-responders. No differences were seen, p = 0.81 for treatment adjustment in this study. TR was prospectively defined as BWT ⩽3 mm, absence of CDS and complications, by Ripollés et al. 73 who followed a cohort treated with biologics, assessing at weeks 12 and 52. TR was reached in 29% (15/51) and of those who remained on anti-TNF treatment, 93% (13/14) with TR stayed on the same treatment, as opposed to those without IUS improvement, where only 35% (7/20) did not require treatment intensification. In another study by the same group, 72 TR was defined as BWT ⩽3 mm and color Doppler grade 0 or 1. Treatment intensification during follow up of a median of 48 months was lower for TR 3% versus 26% for no TR [p = not significant(NS)]. However, only poor outcome, defined as a combination of treatment intensification and surgery reached significance between groups, p = 0.01. In a recently published retrospective paper from Suárez et al., 76 277 patients scanned with IUS were included with a median follow up after last IUS of 24 months (range 5–73). Time to activity outbreak (defined as surgery or initiation/escalation of therapy) was significantly longer for those with TR (BWT <3 mm without Doppler signal), as opposed to those with IUS activity (BWT >4.5 mm), 47 months versus 18 months, respectively, p < 0.0001.
Transmural remission and disease-related hospitalization
In the study by Deepak et al. 78 hospitalization was also significantly reduced for radiological responders (hazard ratio 0.27, p < 0.001) and partial responders (hazard ratio 0.57, p = 0.04). Fernandes et al. 35 also managed to show significant improvement with TR (3%, p = 0.003) on hospitalization needs within 12 months, as opposed to NH (24%), TR was, again, better (p = 0.044) than ER (17%, NS) and ER did not show significant approval over NH. Hallé et al. 69 also looked at risk of hospitalization between radiological responders versus non-responders and found no significant difference p = 0.75, with total hospitalization of 18% at 24 months follow up. In the study by Castiglione et al., 7 hospitalizations were much improved when therapy resulted in TR (9%) compared with both ER (28%) and NH (67%), respectively, p < 0.001.
Transmural remission and surgery
Several studies have addressed the question of whether or not TR impacts surgical rates. Deepak et al. 78 could again show better outcomes for radiological response (hazard ratio 0.32, p < 0.001) but not partial response (hazard ratio 0.70, p = 0.23) for any CD-related surgery. Impact of TR on surgery was nicely shown by Fernandes et al., 35 with none (p = 0.027) going to the operating room within 1 year, as opposed to 12% and 11% for NH and ER, respectively. Hallé et al. 69 demonstrated surgery 14/115 and endoscopic dilatation 5/115 were more common in the non-responder group when compared with radiological responders, p = 0.04 at 24 months. Thierry et al. 70 retrospectively identified 96 CD patients undergoing MRE with diffusion-weighted imaging and evaluation of the Nancy score, combined with a subsequent ileocolonoscopy before introduction of biologics. Segmental Nancy score <2 and total <6 predicted ER, with significantly fewer operated on compared with those with higher Nancy scores (p = 0.025). In the IUS study by Castiglione et al., none in the TR group underwent surgery after 1 year, which was significantly fewer than those achieving ER (10%, p = 0.009) or NH (36%, p < 0.001).
Discussion and future perspectives
Current concepts
The concept of TR can be attributed to Castiglione et al. 101 This group has led the way in defining the field over the last several years, culminating in their seminal paper demonstrating significant improvements in clinical outcomes at 1 year, compared with ER and symptomatic remission. A number of other studies published to date, demonstrate the importance of achieving TR. Despite this, there remains controversy on the significance of this endpoint. However, consensus seems to have evolved from ileocolonoscopy as the indisputable gold standard, and disqualifying cross-sectional imaging as false positive when residual disease was detected, to investigating residual transmural disease as a true and integrated concept of CD. 30 Cross-sectional imaging has demonstrated superiority to ileocolonoscopy in small-bowel disease,102,103 and now TR is considered one of the more ambitious treatment targets, with evident superior long-term clinical outcome performance compared with ER. 7 In this paper, we have presented the essential work published to date outlining the concepts and outcomes of TR. One of the main limitations is the lack of a clear and standardized definition for TR. Some authors focus only on the transmural aspect of the disease, while others incorporate extramural activity and healing as part of the model. 104 TR is most commonly defined as BWT ⩽3 mm; however, BWT up to 7 mm is considered as TR by some. 69 It is well recognized that these discrepancies are not unique to TR: there is debate and absence of certain agreement for ER and CR, even though these concepts have existed for decades. The importance of bloodflow or perfusion within the normalized bowel wall is also still debatable. In addition, several of the studies outlined here are retrospective66,70,78 or insufficiently powered; 74 thus, to achieve consensus for a TR definition, well-designed prospective multicenter trials are paramount.
Transmural remission versus residual transmural disease
TR is a logical treatment target, acknowledging the contention of residual transmural disease, defined as ER with evident abnormal/pathological increased BWT or increased bloodflow in the normal bowel wall (Figure 4). In most studies, TR will typically only occur with coexisting ER, whereas the opposite is not the case, highlighting the importance of residual transmural disease. Future trials should reflect this issue in the study design, power, and research question, to facilitate further understanding of the pathophysiological concept and clinical outcomes between those with inflammation resolution beneath the mucosa and those who do not. In fact, the potential overlap between ER with microscopic/HR and TR has not been adequately addressed to date.
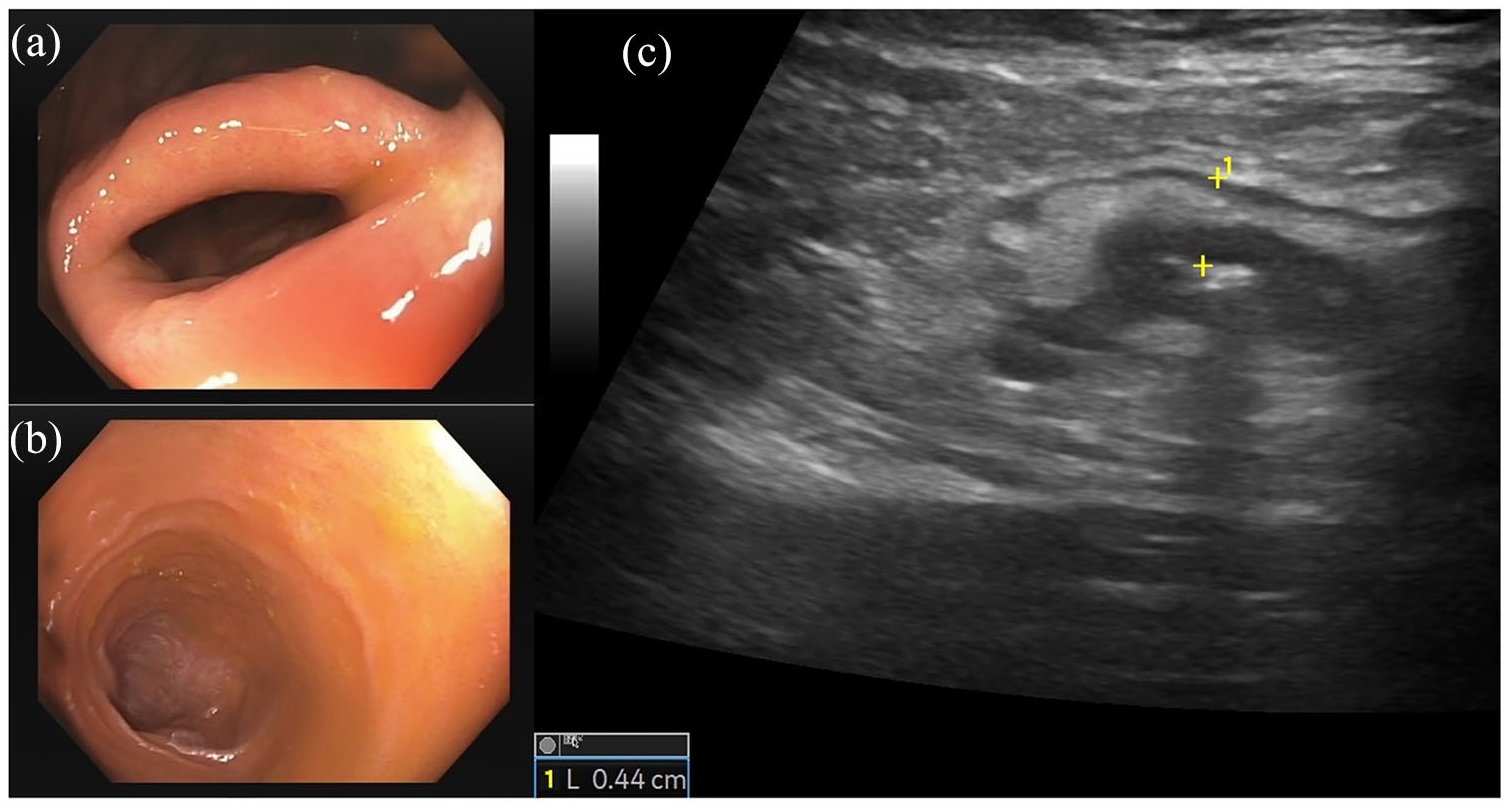
Discrepancy between endoscopic remission (ER) and transmural remission (TR) in a Crohn’s disease (CD) patient.
Will transmural remission become a new target?
Although one can argue TR is an obvious treatment target, the question remains regarding broad application, and if this treatment goal is feasible considering the current treatment options and their limitations, for example, in treating fibrosis. Unfortunately, existing studies have not presented convincing data to predict the attainment of TR. It does, however, appear chances are higher for those with less severe disease, shorter disease duration, longer treatment periods and fewer symptoms at baseline,7,34,71 since they may not have developed fibrotic or chronic changes yet. The proportion of patients reaching TR seems to vary between 5% and 50% depending on time of assessment and segment of the bowel, with colonic disease exhibiting greater likelihood of healing faster compared with ileum. 77 For some, ER may be an overly ambitious target, whereas the most aggressive treatment target present today may be the treat-to-clear concept 33 with the goal of clearing the disease and changing the natural history of disease or achieving every measurable symptom state, including HR and TR. Current diagnostic features are, however, not sufficient to determine these goals. We need appropriate tools that allow us to look behind the ‘mucosal wallpaper’ to elucidate the transmural nature of inflammation and structural damage in CD.
Intestinal ultrasound as the optimal tool for assessment of transmural remission
IUS could be this ideal tool for assessment of relevant information beyond the mucosa, used to develop new treatment targets that can be evaluated over and over again. IUS is a low-cost modality, with high accuracy, readily available, safe, and without a significant patient burden.44,105 Compared with MRE, IUS even performs better for colonic disease41,106 and is mostly regarded as equivalent to MRE for small bowel disease.39,42
Limitations of the TR concept: scientific and practical
Similar to the discussion of MH 15 years ago, and the evolution of the term, TR is an aspirational goal. Despite the already mentioned limitation of a lack of consensus definition for TR, imaging modalities such as IUS are still not available in many countries. TR can therefore not be determined in the vast majority of patients. A further limitation might be that most of the current therapies and strategies are not sufficient to reach the goal of TR in a relevant population of CD patients. TR may only be important at the individual patient level and only some patients will achieve this goal with the current therapeutic strategies. Fibrosis is likely to play a relevant role in most patients where TR cannot be achieved. However, as TR in some CD patients is observed several months and even years after starting already existing therapies, it is likely that even the current anti-inflammatory drugs exert anti-fibrotic effects in the long term, at least to some extent. Similar anti-fibrotic effects are observed in patients with liver cirrhosis where fibrosis can be partially reverted during anti-inflammatory treatment. 107
Presently, the questions raised above can unfortunately not be answered based on the current literature. Bringing the concept of TR forward will lead to an increase in studying strategies and novel therapeutic approaches. Further well-designed, high-quality prospective trials will help to guide us in the future. Effectiveness of future drugs might be evaluated regarding their ability to direct immune responses toward anti-fibrotic activity and to induce TR. IUS may be a suitable diagnostic tool to determine these effects.
Conclusion
Residual transmural and extramural findings of inflammation depicted on cross-sectional imaging are clearly important entities increasingly being acknowledged. Complete resolution of transmural disease, TR is an evolving target of therapeutic response showing superior long-term clinical outcomes and surgery-free survival. Further standardization of response and remission measurement and their respective definitions, in addition to the development of validated indices with demonstrable responsiveness, are important to ensure broader application of this important endpoint, both clinically and in multicenter prospective therapeutic trial investigation with long-term follow up. With the increasing use of IUS in randomized controlled trials, we may come up with validated parameters which allow us to include TR as a relevant target in CD in the near future.
Footnotes
Author contributions
Conception and design of the study: RW, TK.
Preparing first draft: RW, TK, KN, CM, RP.
Revising the work critically for important intellectual content: all authors.
All authors approved the final version of the manuscript, edited, and added intellectual content.
RW is the guarantor of this article.
Conflict of interest statement
RW received consulting fees/speaker’s honoraria from AbbVie, Takeda, Janssen, and Pfizer.
KN reports advisory board fees from AbbVie, Janssen, Pfizer, Ferring, Pendopharm and Takeda; speaker’s fees from AbbVie, Amgen, Janssen, Falk Foundation and Pfizer; and research support from AbbVie and Janssen.
CM reports advisory and/or consultation fees from AbbVie, Arena, Biogen, Celgene, Gilead/Galapagos, Falk Foundation, Ferring, Janssen, Pfizer, Roche, and Takeda.
RP reports advisory and/or consultation fess for AI4GI, AbbVie, Arena Pharmaceuticals Amgen, Atlantic Healthcare, BioBalance, Boehringer-Ingelheim, Bristol-Myers Squibb, Celgene, Cosmo Technologies, Coronado Biosciences, Eagle, Eisai Medical Research, Elan, EnGene, Eli Lilly, Ferring, Genentech, Sanofi Genzyme, Gilead, Given Imaging, GlaxoSmithKline, Janssen, Lycera, Meda, Merck & Co., Merck Research Laboratories, Novo Nordisk, PDL Biopharma, Pfizer, Robarts Clinical Trials, Prometheus Laboratories, Protagonist, Receptos, Sandoz, Shire Pharmaceuticals, Sigmoid Pharma, Specialty Rx, Sublimity, Takeda, Theradvance, Satisfai Health, and Innomar.
TK received consultative fees and advisory board fees from AbbVie, Arena, Janssen, Celgene, Celltrion, Galapagos, Gilead, Pfizer, Falk Pharma, Ferring, Takeda, Pfizer, Roche, UCB, and research support from AbbVie and Janssen.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.