
Abstract
Background and Aim:
Inhibition of gastric acid secretion is important for eradicating Helicobacter pylori. Vonoprazan (VPZ) is a strong, long-lasting inhibitor of gastric acid secretion. Studies that examined the effectiveness of VPZ-based triple therapy in second-line treatment have been performed. However, there have been no randomized controlled studies to compare the effect between VPZ-based triple therapy and proton pump inhibitor (PPI)-based triple therapy in second-line treatment, and it is not known which is more effective between VPZ-based and PPI-based therapies. This study aimed to compare the effectiveness of second-line triple therapies including VPZ or rabeprazole (RPZ) as the PPI.
Methods:
Eligible patients with H. pylori infection who failed first-line triple therapy were assigned randomly to the VPZ [VPZ40 mg/day, amoxicillin (AMPC) 1500 mg/day, metronidazole (MNZ) 500 mg/day] or RPZ (RPZ20 mg/day, AMPC1500 mg/day, MNZ500 mg/day) group. A 13C-urea breath test result of less than 2.5% was considered as successful eradication.
Results:
In total, 46 and 41 patients were analyzed as intention to treat (ITT) and per protocol (PP), respectively. Eradication rates in the VPZ and RPZ groups were 73.9% [95% confidence interval (CI) 51.6–89.8%] and 82.6% (95% CI 61.2–95.0%) based on ITT analysis, respectively (p = 0.72). Based on PP analysis, the eradication rates in the VPZ and RPZ groups were 89.5% (95% CI 66.9–98.7%) and 86.4% (95% CI 65.1–97.1%), respectively (p = 1.00). Two patients in the VPZ group and one in the RPZ group discontinued treatment due to side effects (p = 1.00).
Conclusion:
There were no significant differences in efficacy and safety between second-line therapies including VPZ or RPZ.
Background
Helicobacter pylori infection causes chronic active gastritis as well as gastric and duodenal ulcers,1–4 mucosa-associated lymphoid tissue lymphoma, 5 idiopathic thrombocytopenic purpura, 6 and gastric cancer.7,8 Therefore, the Kyoto global consensus report recommended that H. pylori-infected individuals receive eradication therapy, unless there are competing considerations, 9 and eradication therapy has been actively performed.
A major determinant of treatment failure of H. pylori infection is antimicrobial resistance of H. pylori.10,11 The Maastricht V/Florence Consensus Report suggested that proton pump inhibitor (PPI)-based triple therapy containing clarithromycin (CAM) should be abandoned when susceptibility testing is not performed before treatment and the CAM resistance rate in that region is more than 15%. 12 Moreover, in this Consensus Report, bismuth quadruple therapy or non-bismuth quadruple therapy containing a PPI, amoxicillin (AMPC), CAM, and nitroimidazole was recommended in regions where the CAM resistance rate is more than 15%. The Consensus Report suggested that bismuth quadruple therapy or a triple or quadruple therapy containing a fluoroquinolone as a second-line treatment should be performed if PPI-based first-line triple therapy containing CAM and AMPC fails. 12 In Japan, treatment for eradication of H. pylori in patients with gastric or duodenal ulcer has been covered by public health insurance since 2000, and, since 2013, treatment for eradication of H. pylori in all infected individuals has been covered by public health insurance. In Japan, a treatment protocol for eradication of H. pylori has been constructed, and it is necessary to follow the protocol in order to receive reimbursement by the health insurance. Initially, the eradication treatment regimens covered by insurance were a therapy that consisted of a PPI [lansoprazole at a dose of 30 mg, omeprazole at a dose of 20 mg, rabeprazole (RPZ) at a dose of 10 mg, or esomeprazole at a dose of 20 mg], AMPC at a dose of 750 mg and CAM at a dose of 200 mg or 400 mg after meals twice a day for 7 days as the first-line treatment, and a therapy that contains metronidazole at a dose of 250 mg instead of CAM as the second-line treatment. Since a potassium-competitive acid blocker (P-CAB) was developed in 2013, the use of a P-CAB instead of a PPI in these regimens has been covered by public health insurance in Japan.
A bismuth formulation that is recommended for H. pylori eradication in overseas guidelines is not available in Japan. 12 The treatment regimens covered by health insurance in Japan were adopted based on their eradication success rates reported in published studies in overseas journals.13–18 In these studies, eradication rates of the first-line treatment and the second-line treatment were 83–89% and 87–92%, respectively. In recent years, the eradication success rate has decreased gradually due to an increase in drug-resistant bacteria, particularly clarithromycin-resistant bacteria. 19 Inhibition of gastric acid secretion is important for eradicating H. pylori.20–22 Recently, vonoprazan (VPZ), a P-CAB that is a strong and long-lasting inhibitor of gastric acid secretion, was developed and appeared on the market.23,24 A phase III randomized trial indicated that P-CAB-based triple therapy that consisted of VPZ, AMPC, and CAM was more effective than a PPI-based triple therapy that consisted of lansoprazole, AMPC, and CAM, and the eradication rate of the P-CAB-based therapy was 92.6% in the first-line treatment. 25 The eradication rate increased as the proportion of VPZ-containing regimens in the first-line eradication regimen increased. 26 However, it is not known whether P-CAB-based therapy or PPI-based therapy as the second-line treatment is more effective. In the phase III trial, some subjects who failed their allocated VPZ- or PPI-based first-line triple therapy received VPZ-based second-line triple therapy that consisted of VPZ, AMPC, and metronidazole (MTZ). 25 The eradication rate was high at 98%. To date, prospective single-arm studies and retrospective studies that examined the effect of P-CAB-based triple therapy in second-line treatment have been performed.26–28 However, there have been no randomized controlled studies to compare the treatment effect between P-CAB-based triple therapy and PPI-based triple therapy in second-line treatment. This study aimed to examine the differences in efficacy and safety between the second-line triple therapies that included VPZ or rabeprazole (RPZ) as the PPI.
Methods
Patients
H. pylori-positive patients who failed a first-line eradication therapy consisting of a PPI, AMPC, and CAM or a P-CAB, AMPC, and CAM were recruited for this study. Eradication failure was confirmed based on the result on the 13C-urea breath test of 2.5 per 1000 or greater, positivity for H. pylori antigen in stool, positive rapid urease test, or positive histological evaluation of H. pylori before enrollment in this study. The sensitivity and specificity of the result on the 13C-urea breath test with cutoff value of 2.5 per 1000 were reported to be 97.7% and 98.4%, respectively. 29 In the urea breath test procedure, after fasting at least 5 h, the patient, in a sitting position, swallows one tablet containing 100 mg of 13C-urea (Otsuka Pharmaceuticals Co., Ltd., Tokyo, Japan) without chewing the tablet, with 100 ml of water. Breath samples are collected into separate bags before and 20 min after taking the tablet. Patients who had received a PPI or P-CAB within 2 weeks of the study start, who had a past history of hypersensitivity to one or more drugs in the treatment regimens in this study, who had serious hepatic, renal, or cardiac disease, who were or might have been pregnant, or who were lactating, were excluded from this study.
The protocol used for this study was reviewed and approved by the Juntendo University Ethics Committee. This study was conducted in accordance with the principles of the Declaration of Helsinki, and written informed consent was obtained from each patient. This study was registered with the University Hospital Medical Information Network Clinical Trials Registry (identifier: UMIN000016601).
Study design
This was a randomized, open-label, parallel-group study conducted at two centers in Japan between March 2015 and March 2017. Eligible patients were allocated randomly to receive VPZ-based therapy that consisted of VPZ at a dose of 20 mg, AMPC at a dose of 750 mg, and MNZ at a dose of 250 mg (VPZ group), or RPZ-based therapy that consisted of RPZ at a dose of 10 mg, AMPC at a dose of 750 mg, and MNZ at a dose of 250mg (RPZ group) after meals twice a day for 7 days. Assessment of H. pylori eradication was performed at least 4 weeks after the end of treatment. A 13C-urea breath test result of 2.5% or less was considered as successful H. pylori eradication. The results of this randomized trial are reported according to the CONsolidated Standards of Reporting Trials (CONSORT) 2010 containing a 25-item checklist (Supplemental File) and flow diagram. 30
Procedures
At the beginning of the study, the patient’s background characteristics, including the type of first-line eradication treatment, method of diagnosing, and whether or not eradication was successful, were recorded. Subjects were allocated randomly in a 1:1 ratio to either the VPZ group or the RPZ group. The randomization sequence with a block size of four was generated using a web-based service. The randomization sequence was concealed in opaque numbered envelopes, which were opened in numerical order. During the study period, drug-related subjective adverse events and compliance rate were recorded. At the end of the study, drug-related objective adverse events were recorded. The primary endpoint was the eradication rate, and the secondary endpoint was safety, that is, the occurrence of drug-related adverse events.
Statistical analysis
This study was a pilot study without sample size calculation. Initially, we planned to recruit 70 subjects with 35 subjects in the VPZ group and 35 in the RPZ group. However, as it took much time to recruit subjects, we changed the target number of patients to 46. For efficacy analysis, we performed both intention to treat (ITT) analysis and per protocol (PP) analysis. Baseline characteristics of the VPZ and RPZ groups were compared using Fisher’s exact test for categorical variables, or unpaired Student’s t test for continuous variables. The eradication rate and incidence of adverse events were compared using Fisher’s exact test. P values less than 0.05 were considered to be statistically significant; 95% confidence intervals (CIs) were also calculated. All analyses were undertaken using SAS software version 9.4 (SAS Institute, Cary, NC, USA).
Results
A total of 46 patients who were considered to have fulfilled the inclusion and exclusion criteria for recruitment, were randomized to the VPZ group or RPZ group in equal numbers. However, it was subsequently found that one patient in the VPZ group did not fulfill the inclusion criteria. One patient in the VPZ group did not return to our hospital for assessment of H. pylori eradication and was withdrawn from the study. Two patients in the VPZ group and one patient in the RPZ group who discontinued the respective treatment due to adverse events were withdrawn from the study. Therefore, 46 patients were available for ITT analysis and 41 patients were available for PP analysis. Figure 1 shows the CONSORT flow diagram. The baseline characteristics of the VPZ and RPZ groups were similar (Table 1). Treatment compliance was 100%, except in the two patients in the VPZ group and one patient in the RPZ group who discontinued the respective treatment due to adverse events.
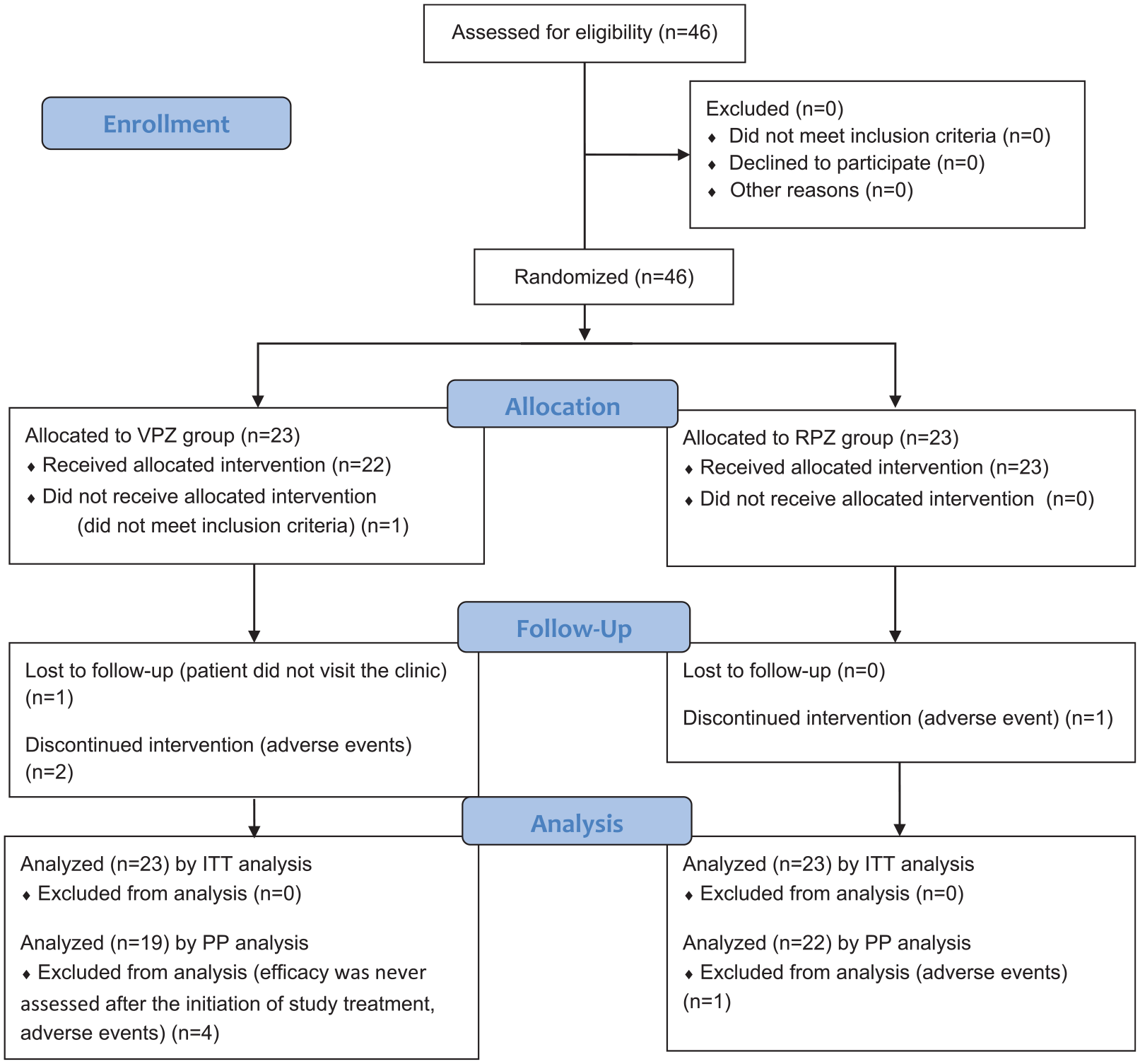
CONSORT 2010 flow diagram.
Baseline characteristics of the Helicobacter pylori-positive subjects.

n.s., not significant; PPI, proton pump inhibitor; RPZ, rabeprazole; SD, standard deviation; VPZ, vonoprazan.
The H. pylori eradication rates were 73.9% (95% CI 51.6–89.8%) in the VPZ group and 82.6% (95% CI 61.2–95.0%) in the RPZ group based on ITT analysis (p = 0.72) (Figure 2a). Based on PP analysis, the H. pylori eradication rates were 89.5% (95% CI 66.9–98.7%) in the VPZ group and 86.4% (95% CI 65.1–97.1%) in the RPZ group (P = 1.00) (Figure 2b). Among patients who had received first-line triple therapy that included VPZ, eradication rates were 80% (95% CI 28.4–99.5%) in the VPZ group and 60.0% (95%CI 14.7–94.7%) in the RPZ group based on ITT analysis (p = 1.00) (Figure 3a). Among patients who had received first-line triple therapy that included a PPI, eradication rates were 72.2% (95% CI 46.5–90.3%) in the VPZ group and 88.9% (95% CI 65.3–98.6%) in the RPZ group based on ITT analysis (p = 0.40) (Figure 3b). Among patients who had received first-line triple therapy that included VPZ, eradication rates were 100% (95% CI 39.8–100%) in the VPZ group and 60.0% (95% CI 14.7–94.7%) in the RPZ group based on PP analysis (p = 0.44) (Figure 4a). Among patients who had received first-line triple therapy that included a PPI, eradication rates were 86.7% (95% CI 59.5–98.3%) in the VPZ group and 94.1% (95% CI 71.3–99.9%) in the RPZ group based on PP analysis (p = 0.59) (Figure 4b).

Comparison of Helicobacter pylori eradication rates in the VPZ and RPZ groups in (a) ITT analysis; and (b) PP analysis. Number of patients is shown in parentheses. 95% CIs are shown in square brackets. P values were calculated by Fisher’s exact test.

Helicobacter pylori eradication rates according to whether the first-line triple therapy that the patients had received included VPZ (a) or PPI (b) based on ITT analysis.

Helicobacter pylori eradication rates according to whether the first-line triple therapy that the patients had received included VPZ (a) or PPI (b) based on PP analysis.
The percentage of patients who complained of adverse events was 47.8% (11/23) and 30.4% (7/23) in the VPZ group and in the RPZ group, respectively (p = 0.37) (Table 2). Two patients in the VPZ group and one patient in the RPZ group discontinued treatment due to adverse events (p = 1.00). The adverse events that caused patients to discontinue treatment in the VPZ group were skin eruption and dizziness, and the adverse event that caused the patient to discontinue treatment in the RPZ group was skin eruption. There were no significant differences in the incidence of each adverse event between the VPZ and RPZ groups.
Summary of drug-related adverse events.

Data are expressed as number of subjects with percentage in parentheses.
One patient in each group dropped out of the study due to skin eruption.
One patient in the VPZ group dropped out of the study due to dizziness.
RPZ, rabeprazole; VPZ, vonoprazan.
Discussion
The results of the current study showed that there were no significant differences in efficacy and safety between the second-line triple therapies including VPZ or RPZ. AMPC inhibits cell wall synthesis. As a result, microorganisms in the growth phase die.22–24 CAM inhibits protein synthesis. Protein synthesis is required for cell division and is rarely required during the stationary phase. Therefore, both AMPC and CAM work well against H. pylori in the growth phase. 22 H. pylori survives and grows between pH 6.0 and pH 8.0, and it survives but does not grow between pH 4.0 and pH 5.0 in vitro in the absence of urea.23,24 Although the usual gastric pH is acidic at around pH 1.0, the urease activity of H. pylori increases the periplasmic pH to 4.0–8.0, allowing H. pylori to survive in the stomach. 31 By suppressing gastric acid secretion, and raising the gastric pH to more than 5, H. pylori moves into the growth phase. Moreover, H. pylori modifies its morphology from a viable spiral-shaped form to a viable but non-culturable coccoid form in an acidic environment. Strong inhibition of acid secretion could promote its transition from the coccoid form to the spiral-shaped form. 32 Accordingly, it is most important to increase gastric pH in order to increase the eradication rate, especially in the first-line triple therapy containing AMPC and CAM. The high eradication rate of P-CAB-based first-line triple therapy supports this theory. In the second-line treatment, MNZ is used. MNZ targets DNA; therefore, the efficacy of MNZ does not depend on whether H. pylori is in the growth phase or the stationary phase, 22 and thus it is not affected by intragastric pH. Although the efficacy of AMPC is affected by intragastric pH, if MNZ plays a more important role than AMPC in the second-line treatment, the eradication rate may not depend on whether PPI or P-CAB is used in the second-line treatment. Moreover, the eradication rate of second-line triple therapy including PPI is already high. 33
However, it was expected that the second-line eradication rate of VPZ-based triple therapy would be higher than that of RPZ-based triple therapy among patients who failed the first-line triple therapy that included a PPI even if MNZ is a key drug in the second-line treatment. In the current study, second-line eradication rates among patients who had received first-line triple therapy that included a PPI were 72.2% in the VPZ group and 88.9% in the RPZ group. The number of subjects who had received first-line eradication treatment containing VPZ was small at 10, and the sample size may have been insufficient to infer the properties of the population. It was also not possible to make a statistical comparison as to whether VPZ-based triple therapy or RPZ- based triple therapy was more effective as the second-line eradication treatment among patients who had received first-line eradication treatment including VPZ. However, the second-line eradication rate in the RPZ group was sufficiently high. It was reported that the minimum inhibitory concentration of AMPC for H. pylori remained reasonably stable at various pH values from 5.7 to 8.0 34 ; therefore, enhancement of the bactericidal action of AMPC against H. pylori by VPZ may not be very strong. Because the presence of CAM-resistant H. pylori greatly influences the treatment success of the first-line eradication treatment in Japan, 10 second-line eradication treatment that does not include CAM is expected to result in a high eradication rate regardless of whether it includes a PPI or P-CAB. Moreover, RPZ itself has been indicated to possess antibiotic effects against H. pylori, 35 and it might have helped to increase the eradication rate.
Although the percentage of patients who complained of adverse events was 52.4% in the VPZ group and 30.4% in the RPZ group, both treatments were well tolerated, with two and one subjects who dropped out of the study due to adverse events in the VPZ group and RPZ group, respectively.
All PPIs are eliminated from the body by hepatic enzymatic metabolism; CYP2C19 is primarily responsible for the elimination rate.36,37 PPIs are also metabolized by CYP3A4 with considerable variability depending on the type of PPI. Genetic polymorphism of CYP2C19 has been identified. 36 The ability of CYP2C19 to metabolize a part of PPIs varies depending on CYP2C19 gene polymorphism. In individuals with homozygosity for the wild-type allele, that part of PPIs is metabolized extensively by CYP2C19, and in individuals with two mutant alleles, that part of PPIs is metabolized poorly by CYP2C19. Therefore, the therapeutic efficacy of PPIs varies greatly depending on the CYP2C19 genotype.38–40 However, because VPZ is metabolized mainly by CYP3A4 and partially by CYP2B6, CYP2C19, CYP2D6, and SULT2A1, 41 the therapeutic efficacy of VPZ is least affected by the CYP2C19 genotype. Among PPIs, RPZ is metabolized both by enzymatic reactions via CYP2C19 and by nonenzymatic reactions 36 ; therefore, RPZ among PPIs is the least affected by the CYP2C19 genotype. Accordingly, we chose RPZ as the PPI in PPI-based triple therapy in the second-line treatment. The PPI-induced increase in intragastric pH varies depending on the CYP2C19 phenotype such as poor metabolizer (PM) or extensive metabolizer (EM); the 24 h mean intragastric pH is much higher in PMs than in Ems. 42 Among Japanese people, 15–22.5% have been reported to be PMs.43–45 When PPIs that are strongly affected by the CYP2C19 genotype are used instead of RPZ, various differences in eradication rate might occur depending on phenotypic differences among the subjects.
A major limitation of this study is that the sample size was limited, and studies with such small sample sizes cannot show statistically significant differences precisely. Moreover, the fact that the bismuth formulation that is used for H. pylori eradication worldwide is not available in Japan, and the fact that only a 7-day PPI- or P-CAB-based triple therapy both in the first-line and in the second-line eradication treatment regimens has been approved by the government agency of health insurance in Japan, may be a limitation of our study. A recent systematic review has shown that bismuth quadruple therapies that did not contain quinolone are effective, and that the eradication rate increased as the treatment period increased from 7 days to 10 days or more. 46 Moreover, dual therapy consisting of high doses and multiple doses of amoxicillin and PPI has also been reported to be useful as a rescue therapy.47,48 Unfortunately, we cannot administer these therapies in Japan under insurance restrictions. Thus, the results of our study may be useful not in other countries but only in Japan. As the eradication rate of a 7-day PPI-based triple therapy is as high as 90% or more, this regimen could be considered as one of the options for second-line eradication treatment in Japan.
In conclusion, this study showed that there were no significant differences in efficacy and safety between the second-line triple therapies that included VPZ or RPZ, although the statistical power was insufficient. Shinozaki et al. proposed VPZ-based triple therapy as the second-line eradication treatment on the basis of the results of their systematic review of the effectiveness and safety of eradication treatment. 49 However, their study had some limitations. About half of the selected articles in the review were written in Japanese, no randomized controlled studies were included, and there is a time-frame shift between the VPZ-based therapy and PPI-based therapy. It remains unclear whether VPZ-based therapy is more effective than PPI-based therapy. Even now that VPZ has been used instead of PPI for the first-line eradication treatment in Japan, it has become clear that a regimen including PPI remains one of the second-line treatment regimens.
Supplemental Material
Supplementary_File – Supplemental material for Randomized controlled study on the effects of triple therapy including vonoprazan or rabeprazole for the second-line treatment of Helicobacter pylori infection
Supplemental material, Supplementary_File for Randomized controlled study on the effects of triple therapy including vonoprazan or rabeprazole for the second-line treatment of Helicobacter pylori infection by Mariko Hojo, Daisuke Asaoka, Tsutomu Takeda, Yuji Shimada, Kenshi Matsumoto, Kohei Matsumoto, Noboru Yatagai, Yoichi Akazawa, Kumiko Ueda, Hiroya Ueyama and Akihito Nagahara in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
We thank Shuko Nojiri at Department of Medical Technology Innovation Center of Juntendo University School of Medicine for her help with statistical analysis.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.