
Abstract
Potassium-competitive acid blocker (P-CAB) is a class of drug that competitively blocks the potassium-binding site of H+, K+-adenosine triphosphate (ATP)ase. Although the history of this class of drugs started over 30 years ago, clinical use of two P-CABs, revaprazan and vonoprazan, were only recently approved in Korea and Japan, respectively. Among them, vonoprazan has several advantages over conventional proton-pump inhibitors (PPIs), including rapid onset of action, long duration of acid suppression, fewer interindividual variations in terms of acid suppression, and minimum dietary influence on its action. These advantages of vonoprazan have been proved in clinical trials conducted for license approvals for several acid-related diseases. In this review article, current evidence of vonoprazan in the management of gastroesophageal reflux disease (GERD) will be summarized. Since the clinical trial data, as well as postmarketed clinical data, have consistently demonstrated superiority of vonoprazan over conventional PPIs in terms of achieving healing of mucosal breaks and maintaining the healing, it may provide an excellent, if not complete, option for fulfilling some of the unmet needs for current GERD therapy. The safety problem of vonoprazan is also discussed, as more pronounced hypergastrinemia inevitably ensues with its use.
Keywords
Introduction
Gastroesophageal reflux disease (GERD) is currently the most prevalent acid-related disease in Western countries. 1 While it was once thought of as a rare disease in Asian countries, GERD has now been recognized as an emerging disease, prevalence of which has reached over 10% in Japan, Taiwan, and India.2,3 Proton pump inhibitors (PPIs) remain the mainstay for the management of GERD. However, 10–20% of patients with Los Angeles C and D (LA-C/D) grade esophagitis do not heal despite 8 weeks of continuous double-dose PPI therapy. 4 Moreover, it has been well documented that achieving complete symptomatic relief with PPI is more difficult than simply healing mucosal breaks, resulting in dissatisfaction of current therapy in about one third of patients with GERD.5,6 To improve therapeutic gain, a histamine H2 receptor antagonist (H2RA) before sleep, in addition to twice daily PPI was proposed for controlling nocturnal acid breakthrough (NAB). 7 Despite successful control of NAB in the short term, the efficacy of the add-on H2RA eventually declined due to development of tolerance to H2RA. 8 For the daytime heartburn control, tentative sealing of ‘acid pocket’ occurring after meals with sodium alginate–antacid formulation has been reported to reduce post-prandial acid reflux.9,10 Obviously, however, this approach cannot be employed for NAB. Baclofen, a gamma-aminobutyric acid (GABA-B) receptor agonist, showed some effects on reducing reflux by tightening the lower esophageal sphincter (LES), 11 but adverse events such as drowsiness limit its use. Long-acting PPIs such as tenatoprazole 12 and modified-release (MR) formulation of dexlansoprazole MR improved 24 h pH control over conventional lansoprazole. 13 The former drug has not been marketed yet and the MR formulation of enantiomer of lansoprazole has not achieved full success for healing and symptom control in patients with GERD despite improved metabolic profile of enantiomer, dual-release formulation, and increased dosage, as compared with conventional lansoprazole. 14 One of the important limitations of dexlansoprazole MR is inadequate control during night time of pH > 4, even with higher doses. 13 Patients who continuously suffer from symptomatic or unhealed esophagitis under PPI therapies may require more invasive endoscopic or surgical therapies. Hence, there are definite unmet needs for more efficient therapies for managing GERD.
In Japan, vonoprazan, a novel potassium-competitive acid blocker (P-CAB), which may overcome some of the limitations of current PPI therapy, was approved for insurance coverage in 2014 and marketed in 2015 for treatment of gastric and duodenal ulcers, erosive esophagitis, eradication of Helicobacter pylori and prevention for recurrence in nonsteroidal anti-inflammatory-drug (NSAID) or low-dose-aspirin (LDA) ulcer. In this review, I will summarize current evidence on the efficacy and safety of vonoprazan focusing on the management of GERD.
What are potassium-competitive acid blockers?
The first drug categorized as a P-CAB, SCH 28080 (Figure 1), was developed as an antisecretory drug more than 30 years ago.15,16 It was later found that SCH 28080 was a competitive ligand of the K+ site of H+, K+-adenosine triphosphate (ATP)ase,17,18 the mode of action distinct from PPIs that requires acid-catalyzed activation and covalent binding as sulfhydryl agents to H+, K+-ATPase. However, clinical development of SCH 28080 was stopped due to hepatotoxicity. Since then, another drug, AZD0865 (linaprazan) was developed. AZD0865 is a potent, but reversible, inhibitor of H+, K+-ATPase, with rapid onset of action. 19 In phase II and III trials, it exhibited similar efficacy with esomeprazole 40 mg in terms of healing of esophagitis and for symptom control for nonerosive reflux disease (NERD).20,21 However, further clinical development was suspended as the efficacy was not superior to esomeprazole and there was a concern on hepatotoxicity during these trials.20,21

Chemical structure of potassium-competitive acid blockers.
Among drugs categorized in P-CABs, the first P-CAB used in clinical practice was revaprazan (YH1885, Revanex®) (Figure 1), which was first marketed in South Korea.22,23 In common with previous P-CABs, it showed a rapid onset of action. However, the acid suppression with revaprazan was not superior to conventional PPIs, as the mean intragastric pH was pH 3.3 and 3.9 on the first and the seventh day, respectively, in healthy male volunteers given 200 mg of revaprazan. Furthermore, the pH > 4 holding time of the dose of revaprazan (200 mg) chosen for clinical use was < 12 h, 23 which was similar or even inferior to the value reported in conventional PPIs 24 (Table 1). Indeed, the efficacy of healing of ulcers after endoscopic submucosal dissection with revaprazan was similar to 20 mg of rabeprazole. 25 No publication was found for GERD treatment with revaprazan by PubMed search. Considering that the pH > 4 holding time is an important predictor of healing erosive esophagitis, 26 it may be presumed that the advantage of using revaprazan over PPI would be small, if any. Indeed, revaprazan has not yet been approved for GERD therapy from the regulatory authority (see Acknowledgments).
pH > 4 holding time (%) with proton-pump inhibitors and potassium-competitive acid blockers.

Data obtained from healthy volunteers. 24
Data obtained in healthy males. 22
Data obtained in healthy Japanese males or those in the UK. 34
JP, Japanese; UK, Subjects from the United Kingdom.
The second P-CAB introduced in actual clinical use is vonoprazan fumarate (TAK-438), which was marketed in Japan in early 2015 and has gained popularity because of its superior properties to conventional PPIs in terms of rapid onset of action, longer duration of action, consistent acid suppression irrespective of CYP2C19, and, most importantly, more potent acid suppression.
Currently, a phase III clinical trial [ClinicalTrials.gov identifier: NCT03006874] for reflux esophagitis is conducted in Korea to compare the safety and efficacy of new P-CAB, tegoprazan (RQ-00000004/CJ-12420) 50 and 100 mg with 40 mg of esomeprazole, the details of which are yet to be published.
Vonoprazan fumarate, a potassium-competitive acid blocker with proven track records for gastroesophageal reflux disease
Vonoprazan fumarate has a different chemical structure defined as a pyrrole derivative which is different from previous P-CABs such as SCH 28080 and AZD0865 that have benzimidazole ring or revaprazan having pyrimidine ring 27 (Figure 1). Another notable difference from previous P-CABs is that vonoprazan has alkaline pKa of 9.06, which enabled its high level of accumulation in acid space such as intracellular canaliculi of the parietal cells. 28 In animal experiments, vonoprazan highly accumulated in the gastric gland both in the resting and in the active state; remarkably, the ratio of accumulation in the resting gastric gland was higher than that in the actively secreting gastric gland, as compared with lansoprazole. 29 The accumulation of vonoprazan in the resting gland might account for its rapid onset of action although further experiments are necessary to examine whether vonoprazan can accumulate in the tubulovesicles in the resting parietal cells, and inactivate H+, K+-ATPase. Furthermore, vonoprazan selectively accumulated in the gastric corpus mucosa, particularly in parietal cells as shown in an autoradiography study, 30 verifying specific targeting of this drug. It is rapidly absorbed and reaches to the maximum plasma level (Cmax) within 2 h but the plasma half-life (t1/2) was much longer (t1/2: about 7 h with 20 mg of vonoprazan taken on fasting) than conventional PPIs having much shorter half-lives (t1/2 = 1–2 h), as shown in the pharmacokinetic profile31–33 (Table 2, Figure 2), enabling once-daily dose for clinical use. As it does not require acid-catalyzed activation, similar efficacy of acid suppression with vonoprazan was shown irrespective of the administration before or after breakfast31,32 (Figure 2). Most importantly, vonoprazan exhibited potent, long-lasting acid suppression starting from the first day of administration which was dose-dependent and further increase in 7 days. At 40 mg, vonoprazan achieved almost total achlorhydria in both Japanese and UK patients 34 (Table 1, Figure 3). Thus, the acid suppression with vonoprazan was much quicker and more profound than conventional PPIs and this effect started from the first day of administration. Even at 7 days, when PPIs achieve steady-state acid suppression, vonoprazan showed superiority to esomeprazole (20 mg) or rabeprazole (10 mg) 35 (Figure 4) in terms of the 24 h pH > 4 holding time.
Pharmacokinetic property of proton-pump inhibitors and potassium-competitive acid blockers (single oral dose).

tmax, time to maximal plasma concentration; Cmax, maximal plasma concentration, AUC, area under the plasma concentration curve; t1/2, elimination half-life.
µg/l.
µg·hr/l.

Plasma concentration of vonoprazan after a single oral dose of 20 mg.
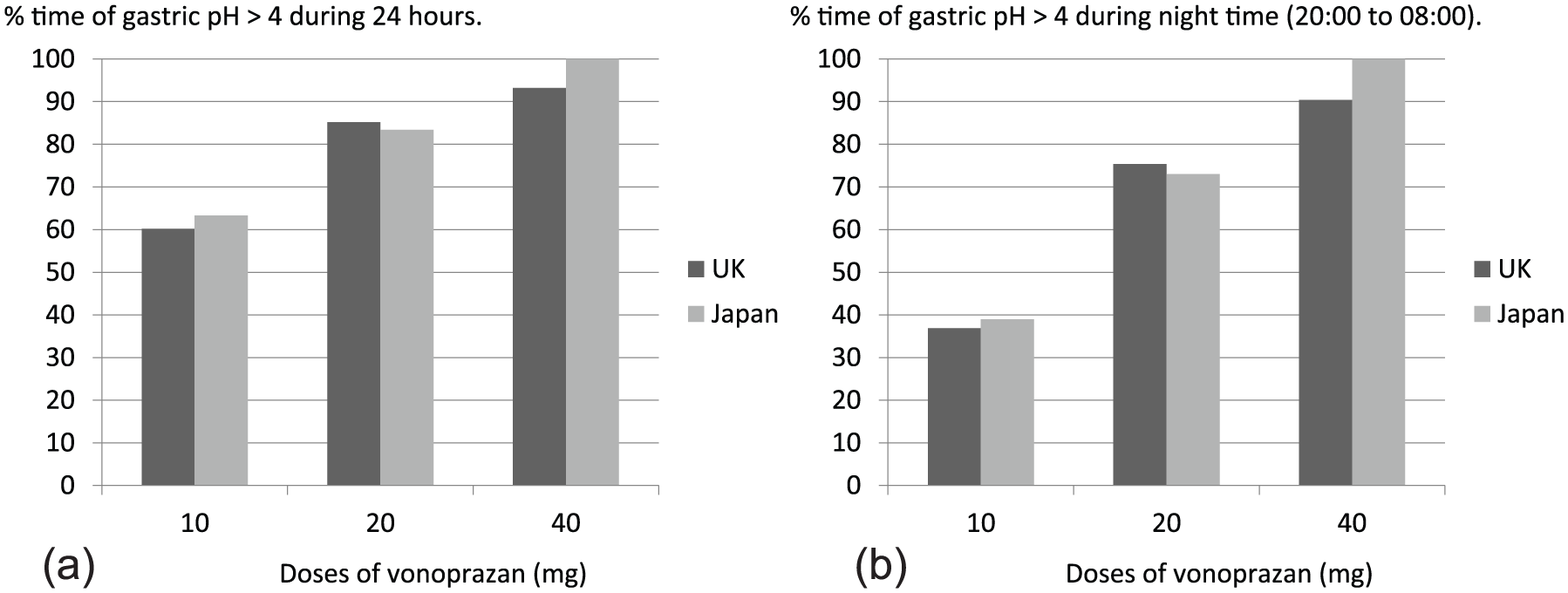
Response for pH > 4 holding time with various doses of vonoprazan.

pH > 4 holding time on the 1st and 7th day.
Other investigators also demonstrated that gastric acid suppression with vonoprazan 20 mg given either as once or twice per day was superior to esomeprazole 20 mg given either as once or twice per day irrespective of CYP2C19 status. 36 One of the unmet needs, NAB, therefore, can be controlled by vonoprazan because pH > 4 holding time in the night time was about 75%, and over 90% with a single morning dose of 20 mg and 40 mg, respectively, 34 and almost 100% when 20 mg was given in two divided doses. 36
Vonoprazan is mainly metabolized in the liver via CYP3A4 of cytochrome P45031,32 (Figure 5), which is distinct from PPIs whose metabolisms are mostly through CYP2C19 pathway. Interference of the metabolism of vonoprazan with clarithromycin, a potent inhibitor of CYP3A4, supports that the major metabolic disposition pathway of vonoprazan occurs through CYP3A4 in humans. 37 Since CYP2C19 status has clinically relevant differences between individuals with extensive metabolizer phenotype versus poor metabolism in terms of the efficacy of PPIs and also influences drug activation process via CYP2C19 such as thienopyridines. Since thienopyridines are often used together with PPIs, this raised a serious concern, as the antiplatelet effect of thienopyridines, if compromised, can lead to grave outcomes, which prompted the US Food and Drug Administration to issue a warning. Metabolic disposition of vonoprazan, less dependent on CYP2C19, provides smaller interindividual variations in the efficacy and less drug interactions through this pathway. However, drugs metabolized through the CYP3A4 pathway can interfere with the metabolism, and conversely, vonoprazan can affect the drugs metabolized through this pathway requiring attention.32,37

Metabolic disposition pathways of vonoprazan.
Effect of vonoprazan for gastroesophageal reflux disease (GERD)
A phase II clinical trial comparing various doses (5–40 mg once per day) of vonoprazan with lansoprazole (30 mg once per day) showed excellent therapeutic effect on erosive esophagitis, reflecting longer 24 h gastric pH > 4 holding time with vonoprazan. 38 Remarkably, 20 and 40 mg of vonoprazan almost completely healed erosions in patients with high grades of erosive esophagitis (LA-C/D) in 4 weeks, whereas healing rate in LA-C/D esophagitis with lansoprazole at 4 weeks was 87%. No serious adverse events were observed in this trial, even with the highest tested dose of vonoprazan (40 mg). Based on the phase II results, the pivotal randomized controlled phase III trial comparing daily dose of 20 mg of vonoprazan with lansoprazole 30 mg for 8 weeks was conducted. This trial was designed to demonstrate the noninferiority of vonoprazan against lansoprazole 30 mg in healing erosive esophagitis as a required step for getting insurance approval from the regulatory authority. Another purpose of this trial was to study a long-term safety and efficacy of vonoprazan. Patients who were healed by 8 weeks of both arms (vonoprazan and lansoprazole) of therapy were assigned to a maintenance dose of either 10 or 20 mg of vonoprazan and followed up for up to 52 weeks. 39 The first phase of this trial looking at healing rate of erosive esophagitis as the primary outcome recapitulated the results of the phase II trial. Overall healing rate at 8 weeks with 20 mg of vonoprazan and 30 mg of lansoprazole was 99.0% and 95.5%, respectively, thus noninferiority of vonoprazan against lansoprazole was verified. Actually, post hoc analysis showed that vonoprazan was significantly better in healing erosive esophagitis than lansoprazole. In a subgroup analysis, vonoprazan scored a significantly higher healing rate (98.7% at 8 weeks) as compared with lansoprazole 30 mg (87.5% at 8 weeks) in those with severe esophagitis (LA-C/D) (Figure 6). In the latter part of this trial studying a long-term efficacy and safety of maintenance dose of vonoprazan 10 or 20 mg per day, recurrence rates at 52 weeks with either dose of vonoprazan were similar and <10% (Table 3). Another trial comparing efficacy of lansoprazole 15 mg, the dose approved for maintenance therapy for GERD in Japan, versus vonoprazan 10 and 20 mg to prevent recurrence of erosive esophagitis for 24 weeks, was conducted. Although the results of this trial have not been published yet, either dose of vonoprazan was clearly superior to lansoprazole 15 mg in preventing recurrence of esophagitis according to the government report 32 (Table 3). Based on these two trials, 10 mg of vonoprazan was approved for maintenance therapy to prevent recurrence of erosive reflux disease in Japan. In case of failure with this dose, however, 20 mg of vonoprazan can be used for maintenance. In previous reports, clinical data on maintaining healing of esophagitis with lansoprazole 15 mg, or esomeprazole 10 mg were published.40,41 Considering similarity with the clinical trial data comparing vonoprazan with lansoprazole 32 and the similarity with independent PPI data, vonoprazan 10 mg seemed to show better preventive effect in maintaining healing of erosive esophagitis (Table 3). Moreover, recurrence rates reported in the maintenance therapy with 10 or 20 mg of vonoprazan was numerically lower than those reported for maintenance therapy using regular doses of PPIs.42,43 Because of many demographic factors such as ethnicity, obesity, and severity of erosive reflux disease in the patients enrolled, this difference should not be interpreted that vonoprazan maintenance with 10 or 20 mg is better than maintenance therapy with regular doses of PPIs. Thus, direct head-to-head comparisons between vonoprazan and regular-dose PPIs are necessary to ascertain whether vonoprazan actually is superior to regular-dose PPIs for maintaining healing. It is unfortunate that recurrence rates according to the baseline severity of reflux disease were not reported in the latter part of this trial. Such information would help physicians understand that vonoprazan should be used for long-term maintenance in patients with severe grade esophagitis, often refractory to PPI maintenance. Although more information is necessary, low rate of recurrence with vonoprazan corroborated well with the data that pH > 4 holding time was important in preventing relapse of healed reflux esophagitis, 44 and provided us with a new armament to protect esophageal mucosal break.
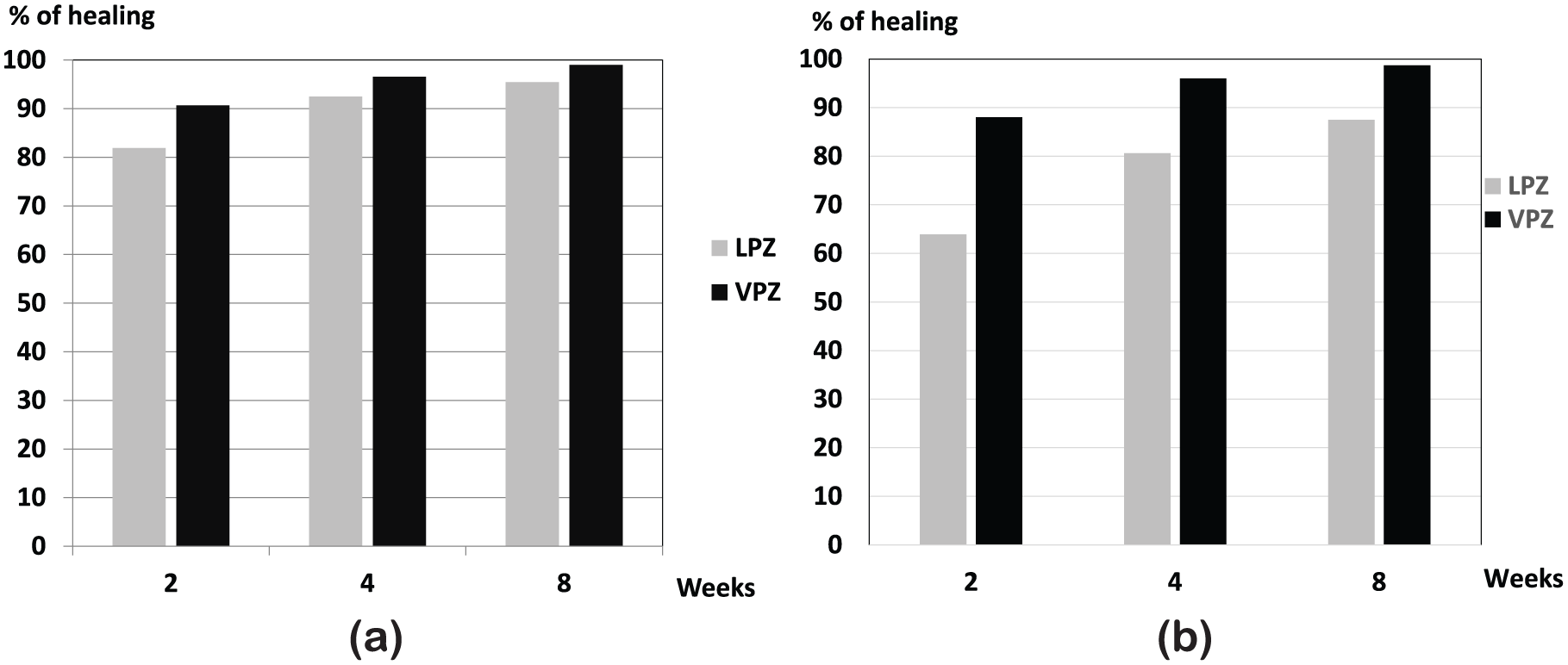
Efficacy of vonoprazan 20 mg for healing erosive esophagitis.
Recurrence rate of erosive esophagitis during maintenance therapy (up to 52 weeks) in Japanese patients.

Data from Ashida et al. 39
Data from the Pharmaceuticals and Medical Devices Agency of Japan. 32
Data from Kawamura et al. 40
Data from Kinoshita et al. 41
Vonoprazan was also shown to exhibit an excellent healing for PPI-resistant esophagitis,45–47 indicating its potential role for fulfilling an unmet need for treating difficult reflux esophagitis.
Unfortunately, in terms of symptom control, another important therapeutic goal for the management of GERD, detailed results were not provided in the phase III trial of vonoprazan. The only statement given on the control of reflux or regurgitation symptoms in this report was that there were no differences between vonoprazan and lansoprazole. 39 No account for the symptomatic control during the maintenance phase of this trial was given, either. Considering the early onset of acid control with vonoprazan, it would be interesting to know whether it provides early symptomatic control over conventional PPIs. However, the performance of vonoprazan may not be so promising in terms of symptomatic control. Indeed, the first randomized placebo-controlled trial comparing vonoprazan 10 mg or 20 mg in patients with NERD failed to show superiority over placebo on the primary outcome measure of the proportion of heartburn-free days. 48 In this trial, NERD patients were classified into two subgroups: patients with no mucosal change (Grade N) and those with minimal mucosal changes such as mucosal redness, or turbidity (Grade M). In the latter group, presence of regurgitation of gastric acid has been strongly indicated, as chromostaining or narrow-band imaging could disclose elements of mucosal damages not identifiable by conventional white light endoscopy. 49 Vonoprazan 20 mg showed significant improvement in heartburn symptoms in the grade M subgroup, as expected. It also decreased the mean severity of heartburn. Since the results of the first trial was close to showing significant difference, a second RCT [ClinicalTrials.gov identifier: NCT02954848] with vonoprazan 10 mg in patients with NERD is currently underway and may be reported in the future. In a smaller-scale retrospective study to examine the effect of vonoprazan on GERD symptoms, successful control of symptoms achieved by 20 mg of vonoprazan was not so impressive: 75% in patients with erosive esophagitis and 60% in patients with NERD. 50 Consistent with this report, vonoprazan was shown to provide symptom resolution in about half of reflux symptoms in PPI-refractory GERD patients. 51 These rather suboptimal response rates indicate causes other than acid are responsible for symptom generation in this group of patients. This problem has been highlighted as therapeutic performance of PPI for NERD patients being inferior to that for erosive esophagitis. 52 Several reasons have been given to explain this unsatisfactory performance of PPIs: increased sensitivity to acid or weakly acidic reflux, motor dysfunction, and perception disorder in the central nervous system are some of the explanations. For instance, patients with functional heartburn are defined as a group of patients whose symptoms are unrelated to acid reflux. Therefore, these patients should be managed by other modalities, although a portion of the patients may respond to PPIs. 53
A recent report also showed that vonoprazan might be effective in patients with eosinophilic esophagitis who were refractory to PPI therapy. 54 Further detailed study is warranted to confirm this preliminary finding.
Safety of vonoprazan
Throughout the course of clinical development, safety of vonoprazan has been surveyed, with particular attention to liver toxicity, as this has been a problem with previous P-CABs.30,33,34 Overall, no serious drug-related treatment-emerged adverse events (TEAEs) were noticed during the clinical trials, including those for GERD. In the abovementioned phase III trial, 39 the safety profile of vonoprazan in the maintenance phase up to 52 weeks was similar to that of lansoprazole. 34 It should be noted that the rate of abnormality in liver function tests in groups assigned to vonoprazan were similar to that of lansoprazole during the 8 weeks. No increase in liver toxicity was noticed during the long-term phase of the study in either group of vonoprazan, 10 or 20 mg. 39
Since vonoprazan suppressed acid inhibition more profoundly than PPIs, increase in serum gastrin level was far greater in patients with vonoprazan than lansoprazole 30 mg. During the 8 weeks of trial, serum gastrin in the group taking vonoprazan 20 mg elevated about one-and-a-half times (about 300 pg/ml) of lansoprazole 30 mg. At the end of the chronic maintenance phase (52 weeks) of continuous administration of vonoprazan either 10 or 20 mg, further increase in serum gastrin was noted in both groups: 317.5 ± 336.42 to 777.6 ± 678.64 (pg/ml) in vonoprazan 20 mg group, and 291.0 ± 219.59 to 514.4 ± 435.53 (pg/ml) in vonoprazan 10 mg, respectively. In animal carcinogenicity experiments using a much higher dose of vonoprazan (5 mg/kg in rat to 6 mg/kg in mouse) for 2 years, increased incidence of gastric endocrine tumor was reported in rodents.31,32 As rodents have been well known for their susceptibility to developing gastric endocrine tumors with acid suppression by histamine H2RA or PPI, this should be interpreted cautiously, considering extremely high doses of vonoprazan. In the long-term prevention trial for GERD, slight increase in gastric endocrine cells was noted at 52 weeks in both vonoprazan 10 and 20 mg groups. 39 For the moment, the longest safety data available for continuous administration for vonoprazan in this regard, are from the low-dose aspirin (LDA) prevention trial with 10 mg of vonoprazan spanning up to 104 weeks. As with maintenance therapy for reflux esophagitis, no gastric endocrine cell tumors were reported, despite higher gastrin level in the patients enrolled in the LDA-prevention trial. 55 Despite the safety data so far obtained in vonoprazan trials, cautious monitoring of endocrine cell hyperplasia and potential development of endocrine cell tumors is mandatory when continuous use of vonoprazan is required, since the development of carcinoid tumor was reported with prolonged use (>10 years in most cases) of PPI. 56 As has been a problem with PPIs, bacterial overgrowth in the gut will inevitably ensue because of the loss of protection conferred by gastric acid. Indeed, profound change in the microbiota was recently reported with 4-week administration of 20 mg of vonoprazan in young healthy volunteers. 57 Long-term consequences of the altered gut microbiota for the host metabolism and health need further vigilance.
As drug absorption can be influenced by gastric acid, coprescription of vonoprazan with atazanavir or rilpivirine is contraindicated due to diminished absorption of these drugs.
PPIs have been widely used for nearly 3 decades and their overall safety has been established. However, a number of safety concerns associated with their long-term use have been raised (Table 4). Recent guidelines from the American Gastroenterological Association did not recommend increasing intake of calcium, vitamin B12, or magnesium beyond the recommended dietary allowance or monitoring of bone mineral density, serum creatinine, magnesium, or vitamin B12. 58 So far, no report concerning these nutritional, metabolic, renal and infectious problems has been published on vonoprazan. Nevertheless, continuous attention should be required for picking up such adverse events associated with vonoprazan, considering its capability of more profound and prolonged acid suppression.
Adverse events associated with chronic proton-pump inhibitor use.

Conclusion
Introduction of more potent, long-acting vonoprazan into clinical use would fulfill at least a part, if not all, of unmet needs of GERD management. For instance, it has a potential to overcome the problem of nocturnal acid breakthrough because acid suppression with a single high dose of vonoprazan or two divided regular doses could cover the night period in the majority of healthy patients. Moreover, efficacy of vonoprazan for patients having a more severe grade of esophagitis in the phase III clinical trial in Japan and for PPI-refractory cases was documented in a small case series, again indicating a promise for fulfilling one of the unmet needs for GERD therapy.39,45–47 Further large-scale, prospective, randomized controlled studies with PPI as a comparator, however, are imperative to verify this potential. For maintaining healing, vonoprazan, even in a low dose showed an excellent result. We need to explore which of the strategies, vonoprazan first and stepped down to PPI; PPI first and stepped up to vonoprazan; or continuous vonoprazan with dose reduction after healing, would be more advantageous in terms of patient satisfaction, required cost and long-term safety concerns associated with hypergastrinemia and hypochlorhydria.
Another unmet need with conventional PPIs has been a rather poor symptomatic control in patients with NERD. Unfortunately, very few data are available with vonoprazan, requiring further evidence in this aspect of managing GERD.
Of course, we need to carefully watch the long-term safety of vonoprazan, including the development of gastric neuroendocrine tumors, influence on nutrient deficiency, increase in infection, and alteration of gut microbiota among others.
For the moment, vonoprazan is available only in Japan, but an international trial of comparing vonoprazan with lansoprazole in patients with erosive reflux disease in Asia, including China, Korea, Taiwan and Malaysia is underway. It is expected that it would be launched for use for GERD patients in some of the Asian countries in 2018. Considering highly efficient eradication results with vonoprazan-based triple therapy for Helicobacter pylori, 59 further expanded license for this indication is expected, as the disease burden associated with this infection, such as gastric cancer, is high in this part of the world. A phase II clinical trial of vonoprazan in Europe has been initiated and that of the USA is under consideration, where the demand for better therapy for GERD patients is high. Thus, vonoprazan might have a potential to play a pivotal role in the management of GERD internationally in the future.
Footnotes
Acknowledgements
I am grateful to Professor Nayoung Kim, Bundang Seoul National University Hospital, for providing me with the information on revaprazan.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
KS has received lecture fees from Takeda Pharma Inc., EA Pharma and Astra Zeneca.