
Abstract
Background:
Current guidelines recommend performing esophagectomy after endoscopic resection for early esophageal cancer when the risk of lymph node metastasis or residual cancer is found to be significant and endoscopic treatment is therefore noncurative. Our aim was to assess the safety and oncological outcomes of esophagogastric resection in this specific clinical setting.
Patients and methods:
A retrospective review from 2012 to 2018 was performed at four tertiary referral centers. All patients had a noncurative endoscopic resection of a clinical T1 esophageal cancer, followed by esophagectomy. Outcome measures were the rates of T0N0 specimens, overall survival, disease-free and cancer-specific survival, postoperative morbidity and mortality.
Results:
A total of 30 patients (13 with squamous cell carcinoma and 17 with adenocarcinoma) were included. The reasons for noncurative endoscopic resection were: positive vertical margins (n = 12), squamous cell carcinoma with muscularis mucosae or submucosal layer invasion (n = 3 and 9), adenocarcinoma with deep submucosal invasion (n = 11), poorly differentiated tumor (n = 6) and lymphovascular invasion (n = 6). Overall, 63% of the esophagi were T0N0: most residual lesions were T1a metachronous lesions, and four (13%) patients had advanced pT status (n = 3) or lymph node metastases (n = 2). Overall survival, disease-free survival and cancer-specific survival were 83%, 75%, and 90% respectively. A total of 43% of patients had severe postoperative complications, and postoperative mortality was 7%.
Conclusion:
In this cohort, esophagectomy allowed the resection of residual advanced cancer or lymph node metastases in 13% of cases, at the cost of 43% severe morbidity and 7% mortality. Therefore, the possibility of close follow up needs to be balanced with a highly morbid surgical management in these patients.
Keywords
Introduction
Esophageal cancer is the sixth cause of cancer death with an increasing prevalence and a 5-year survival rate of 10–25%. 1 In recent decades, the rate of early esophageal cancer has increased through improved endoscopic detection. 2 Endoscopic resection is currently widely used for the resection of early esophageal neoplasia, 3 and represents a low morbidity alternative to surgery.4–6 Endoscopic mucosal resection 7 for early adenocarcinoma (EAC) and endoscopic submucosal dissection for squamous cell neoplasia (SCC) 8 are currently recommended for the resection of T1 lesions by the European Society of Gastrointestinal Endoscopy (ESGE) 9 and the American Society of Gastrointestinal Endoscopy. 10
Considering the risk of lymph node metastasis, esophagectomy is recommended in cases of noncurative endoscopic resection in the esophagus. 9 The first criteria to define noncurative endoscopic resection is the deepest intramural tumor extension. For SCC, the risk of lymph node metastasis ranges from 8% to 19% for lesions invading the muscularis mucosae (m3) or the submucosal layer below 200 μm and 30–54% for lesions invading the deep submucosa. For EAC, the risk is nil for mucosal lesions, 5–6% for lesions invading the submucosal layer below 500 μm and 19–21% for lesions invading the deep submucosa.3,9,11,12 The other criteria to define a noncurative endoscopic resection are a poorly differentiated tumor, or the presence of lymphovascular invasion, increasing the risk of lymph node involvement with an odds ratio of 4.04–9.73 and 35.8 respectively.3,13,14 Finally, the curative endoscopic resection of an early esophageal cancer implies an en bloc and histologically complete resection of a well to moderately differentiated lesion, with no lymphovascular invasion, limited to the shallow submucosa (for EAC) or the lamina propria (for SCC).
Esophagectomy and lymph node dissection leads to major complications in up to 40% of patients, and mortality in up to 10%.15–19 Most studies reporting on the outcomes of esophagectomy include patients with stage I and II diseases, with a small proportion of T1 lesions.15–20 Furthermore, the inclusion of patients after neoadjuvant treatment might overestimate the adverse event rates after esophagogastric surgical resection.
This study 21 aims to assess the outcomes of esophagectomy after noncurative endoscopic resection, in terms of pathology results, safety, and survival.
Patients and methods
Patients
This was a retrospective study performed at four French and Belgian tertiary referral centers for therapeutic endoscopy from 2012 to 2018. All patients had a T1 esophageal cancer with a noncurative endoscopic resection, followed by esophagectomy. Surgery was indicated by a multidisciplinary meeting involving gastrointestinal endoscopists, oncologists, surgeons, pathologists, radiotherapists and radiologists. Data were collected from the patients’ medical files, endoscopy and pathology reports.
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki and has been approved by the ethical review committee for publications of the Cochin University Hospital (CLEP decision no. AAA-2018-08013) on 18 October 2018. All patients provided written informed consents for the endoscopic procedures and surgery.
Endoscopic resections
All endoscopic procedures were performed by experienced operators. Endoscopic mucosal resection was performed for SCC smaller than 10 mm and for Paris 0–IIa and 0–IIb EAC, that is, without endoscopic suspicion of deep submucosal invasion. Endoscopic submucosal dissection was performed for lesions larger than 10 mm for SCC, or when protruding or depressed features where found in EAC (Paris 0–Is and 0–IIc). 9 All resections were performed en bloc.
Histological analysis and indication for surgery
Resected specimens were pinned on polystyrene boards and fixed in 10% formalin for 24 h. After fixation, specimens were cut into 2–3-mm slices and embedded in paraffin. Blocks were further sliced at 4 μm and stained with hematoxylin–eosin–saffron. The following data were assessed: histological type, grade of differentiation, invasion of the lateral or vertical margins, deepest tumor extension (mucosal or submucosal invasion), and presence of lymphovascular involvement. 22 The length of the tumor was not considered. R0 resection was defined as an en bloc resection, with horizontal and vertical margins free of cancer. In cases of submucosal invasion, the depth of the tumor from the muscularis mucosae was measured. Curative endoscopic resection was defined as a R0 resection without deep mural infiltration or poor histoprognostic factors, as defined by the ESGE guidelines: absence of poorly differentiated cancer, absence of lymphovascular involvement 14 and absence of deep invasion: mucosal m3 or submucosal invasion for SCC and >500 µm submucosal invasion for EAC. 22
Surgical treatment
Open esophagectomy or minimally invasive esophagectomy were performed, under general anesthesia with endotracheal intubation, with intraoperative thoracic epidural analgesia. Esophagectomy and lymph node resection were performed by right transthoracic/Ivor Lewis, transhiatal or tri-incisional/McKeown techniques, according to the tumor localization and the surgeon’s choice.23,24 Cervical approach was performed above 25 cm and thoracic approach was performed below 25 cm. Extended total gastrectomy was used for Siewert II EAC in patients with major comorbid conditions. Histological examination of the surgical resection was performed by an expert pathologist and defined according to the pathologic TNM (pTNM) classification (AJCC 8th edition). Surgical complications were defined according to the Clavien–Dindo classification, 25 at day 30 and day 90. 19
Follow up
Patients were followed up with physical examination, blood tests, upper endoscopy and a thoraco-abdomino-pelvic computed tomography (CT) scan every 3 months for the first year and every 6 months for 5 years. Local recurrence was defined as a positive biopsy in the bed of the native esophagus. Metastatic recurrence was defined as the appearance of metastatic lesions with or without hypermetabolism on a positron emission tomography (PET)-CT scanner, in the distant organs or lymphadenopathies.
Statistical analysis
The main outcome measure was the rate of cancer-free surgical resection specimens. Secondary outcome measures were the rate of postoperative complications, including perioperative mortality and the overall survival, disease-free survival, and cancer-specific survival. Data were presented as median (range), and percentage. The overall survival rate was calculated from the date of surgery until death or the last follow up. The disease-free survival rate was calculated from the date of surgery until relapse or death from any cause. The cancer-specific survival was calculated from the date of surgery until relapse or death related to cancer. All statistical analyses were performed using the R Studio statistical software (version 3.4.4).
Results
Patient characteristics
A total of 30 patients (13 with esophageal SCC and 17 with EAC) with a median age of 65 years were included. There were 20 men and 10 women. Tumors were localized in the mid and lower esophagus for 15 patients in each category. The main patient characteristics are presented in Table 1.
Patient characteristics.

IQR, interquartile range.
Histological characteristics of the lesions resected endoscopically
Among the 13 patients with SCC, 11 tumors were well or moderately differentiated, and 2 were poorly differentiated. The depth of tumor invasion was: m2 in one patient, m3 in three patients, and deep submucosal invasion in nine patients. Lymphovascular invasion was observed in one patient. Histologically complete (R0) resection was performed in eight patients (62%). For the other cases, the vertical margin was positive in three patients, and impossible to assess (Rx) in two patients.
Among the 17 patients with EAC, 13 tumors were well or moderately differentiated, and 4 were poorly differentiated. The depth of tumor invasion was: m2 in 1 patient, m3 in 1 patient, m4 in 2 patients, superficially invading the submucosa (<500 µm) in 3 patients and deeply invading the submucosa in 11 patients. Lymphovascular invasion was observed in five patients. R0 resection was performed in five patients (29.4%). For the other patients, the lateral margins were positive in two patients, the vertical margin was positive in nine patients and the quality of the resection was not evaluable for one patient (Rx).
The reasons for noncurative endoscopic resection were: positive vertical margins (n = 12), SCC invading the muscularis mucosae (n = 3) or the submucosal layer (n = 9), EAC invading the submucosal layer beyond 500 μm (n = 11), poorly differentiated tumors (n = 6) and presence of lymphovascular invasion (n = 6). In 15 (50%) cases, tumors exhibited more than one poor histoprognostic factor. These criteria are detailed in Table 2.
Criteria for surgery (noncurative endoscopic resection) for each patient according to the European Society of Gastrointestinal Endoscopy guidelines.
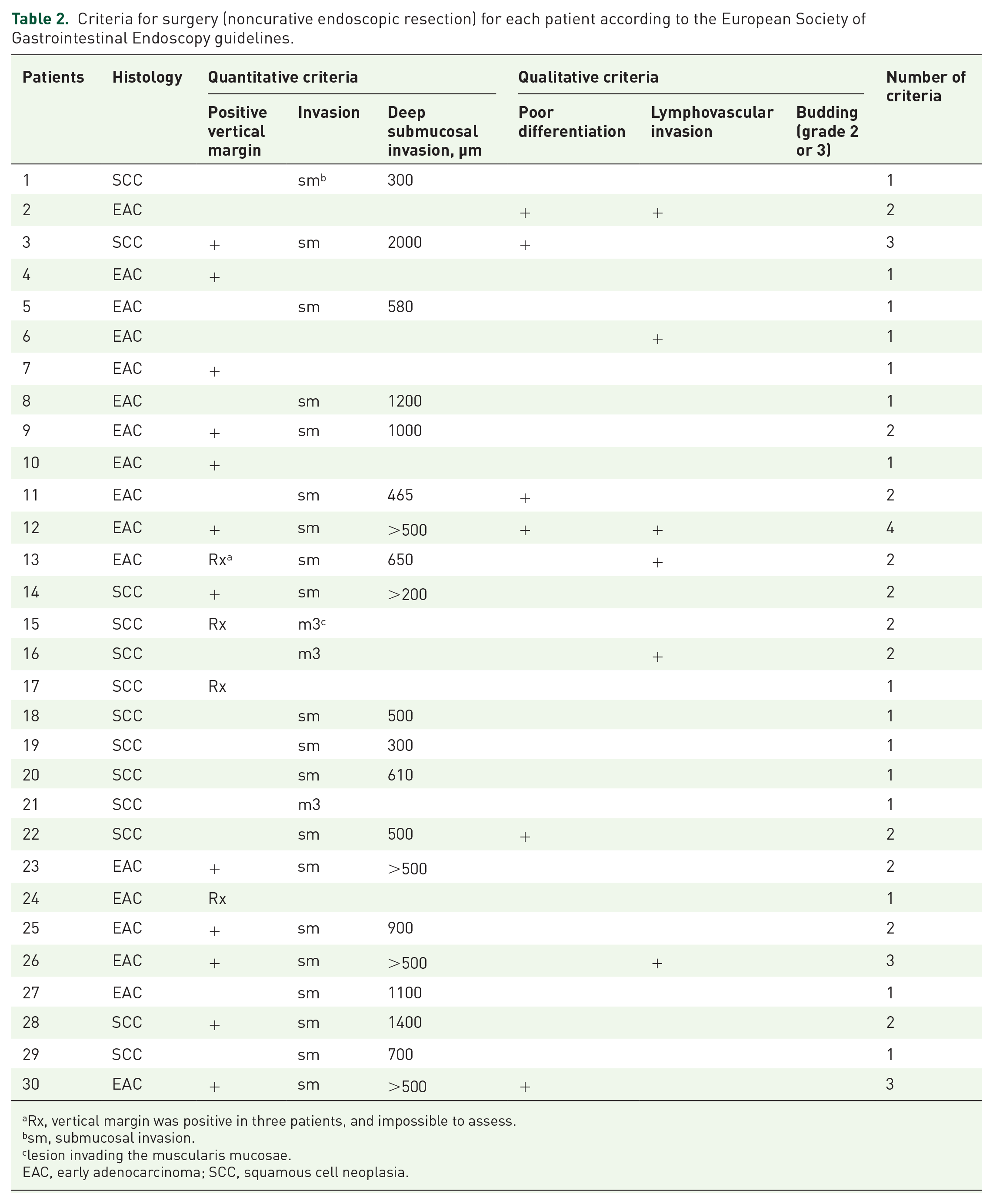
Rx, vertical margin was positive in three patients, and impossible to assess.
sm, submucosal invasion.
lesion invading the muscularis mucosae.
EAC, early adenocarcinoma; SCC, squamous cell neoplasia.
Histological characteristics of the esophagectomy specimen
Surgical techniques were transthoracic esophagectomy (n = 18), transhiatal esophagectomy (n = 5), McKeown esophagectomy (n = 3) and extended total gastrectomy (n = 4).
A total of 60% of patients had an open esophagectomy and 40% had a minimally invasive esophagectomy. The lymph node harvest [median (range)] was 18 (9–29).
The median time [interquartile range (IQR)] between endoscopic resection and surgery was 90 days (55–112).
All patients had macroscopically and histologically complete resection (R0) of all neoplasia by esophagectomy. Overall, 11 (37%) patients had residual cancer on the surgical specimen: 9 with local residual tumor only, 1 with lymph node involvement only and 1 with both. Table 3 shows the detailed histological characteristics of the esophagectomy specimen with residual cancer. Only 2 of 30 (7%) patients had lymph node involvement on the surgical specimen: 1 EAC with a positive vertical margin and residual cancer on the resection site, and 1 SCC with deep submucosal invasion on the endoscopic specimen but no residual cancer on the resection site.
Histological characteristics of the esophagectomy specimens with residual cancer.
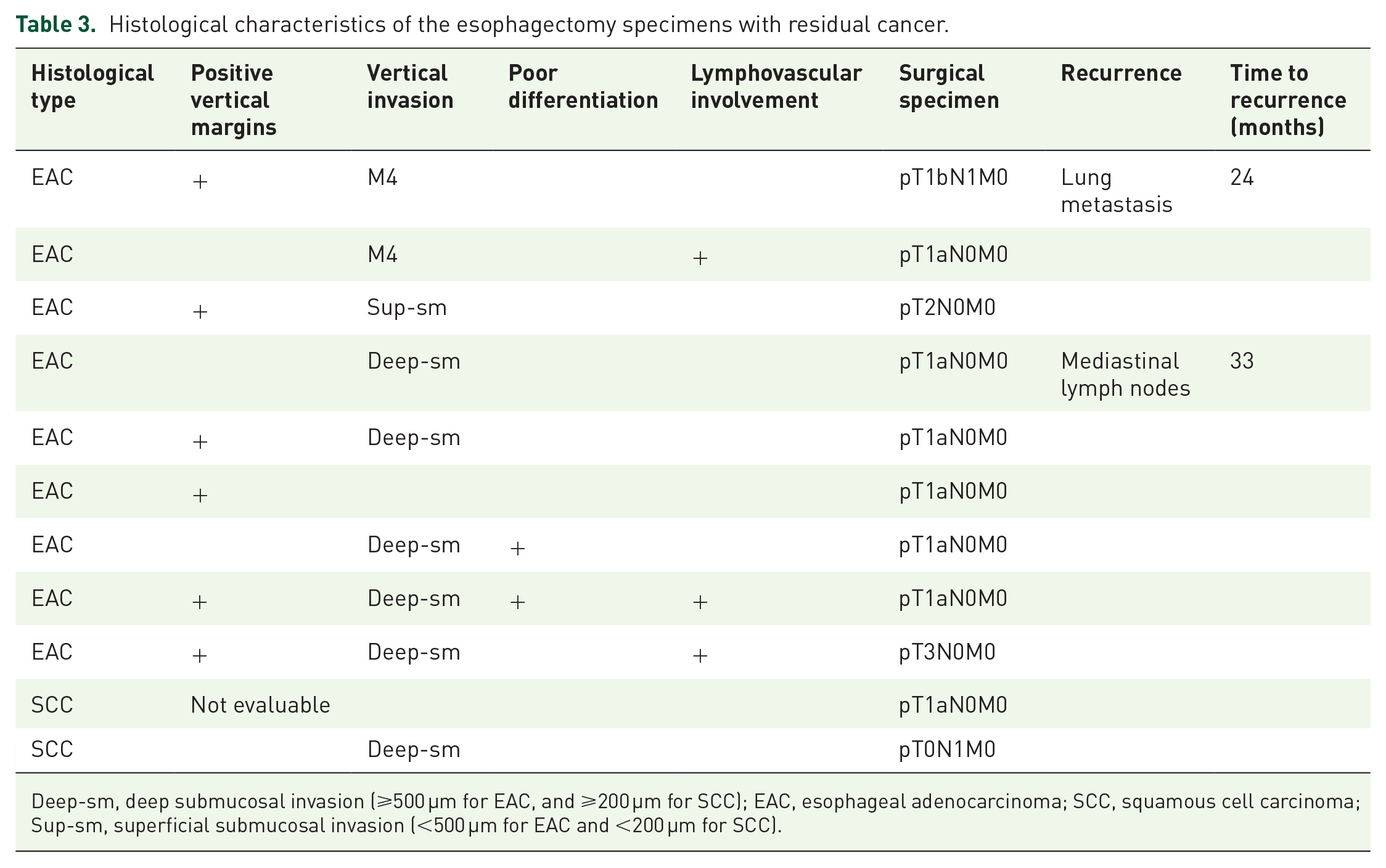
Deep-sm, deep submucosal invasion (⩾500 µm for EAC, and ⩾200 µm for SCC); EAC, esophageal adenocarcinoma; SCC, squamous cell carcinoma; Sup-sm, superficial submucosal invasion (<500 µm for EAC and <200 µm for SCC).
Morbidity and mortality after surgery
A total of 19 patients had one or more postoperative complications. Overall, 43% of the patients (13/30) had severe early (before postoperative day 30) morbidity according to the Clavien–Dindo classification: IIIa (n = 3), IIIb (n = 4), IVa (n = 3) and IVb (n = 3). The in-hospital postoperative mortality (Clavien–Dindo grade V) was 7% (2/30) as shown in Table 4. The 30-day and 90-day mortality rates were 3% and 7% respectively. The main surgical complications were: intrathoracic anastomotic leak (n = 12), intracervical anastomotic leak (n = 2), chylothorax (n = 2), vocal cord palsy (n = 2), plasty necrosis (n = 1), pneumothorax (n = 1), occlusion (n = 1). Finally, nine patients had pulmonary complications, with respiratory failure and the need for invasive ventilation in two of three cases. Late postoperative morbidity cases were anastomotic strictures, observed in two patients.
Postoperative complications according to the Clavien–Dindo classification. 25

Oncological outcomes
We diagnosed two distant cancer recurrences (mediastinal lymph nodes and lung metastases) during a median (IQR) follow up of 15 (8–37) months. The patient with lung metastases developed a recurrence 24 months after surgery for an incompletely resected T1b EAC with residual tumor and lymph node involvement on the surgical specimen (Table 3). The patient with mediastinal lymph nodes was diagnosed with disease recurrence 33 months after surgery and had an incompletely resected T1b EAC with deep submucosal invasion and residual tumor without lymph node involvement on the surgical specimen (Table 3). No local recurrence was diagnosed. There were five deaths during the follow up: two postoperative in-hospital deaths, one caused by aspiration pneumonia due to a postoperative esophageal stricture 16 months after surgery, one death related to cancer recurrence and one noncancer-related death. At the end of the follow up, overall survival, disease-free survival and cancer-specific survival were 83% (25/30), 75% (24/30), and 96% (25/26) respectively. At 1 year, overall survival, disease-free survival and cancer-specific survival were 63%, 70%, and 93% respectively.
In this group of nine patients (five transhiatal surgery and four gastrectomy), we observed six (67%) local residual tumors and no lymph node involvement in the esophagectomy specimen. Furthermore, we observed one relapse (mediastinal lymph nodes; 11%), and two deaths (one for transhiatal surgery and one for gastrectomy; 22%).
Discussion
Esophagectomy is currently the standard therapeutic approach after noncurative endoscopic resection of early esophageal cancer. In this study, surgery provided a high curative rate with an overall and cancer-specific survival of 83% and 96% respectively. However, these results were associated with 43% severe morbidity and 7% perioperative mortality, while only four (13%) patients had an advanced pT status or lymph node metastases, actually indicating esophagogastric resection. Indeed, 7 out of the 11 esophagectomy specimens containing neoplasia exhibited metachronous T1a lesions amenable to endoscopic treatment.
To our knowledge, eight retrospective studies26–33 have examined the outcomes of esophagectomy after endoscopic resection for superficial esophageal cancer (Table 5). The presence of lymph node metastases was low, ranging from 0% to 30%. The overall survival and disease-free survival were high, ranging from 85% to 100% and from 86% to 100% respectively, as also observed in our study. The perioperative mortality was poorly reported, with heterogenous figures, ranging from 0% to 14%. Similarly, perioperative morbidity was scarcely reported, from 26% to 34%, and no long-term morbidity data are available (Table 5). Finally, the indication for surgery after endoscopic treatment was often unclear.
Studies reporting outcomes of esophagectomy after noncurative endoscopic resection.

EAC, esophageal adenocarcinoma; DFS, disease-free survival; NA, not available; OS, overall survival; SCC, squamous cell carcinoma.
Zhang and colleagues recently performed a large retrospective study in patients with T1 SCC treated by esophagectomy (n = 274). The overall survival and cancer-specific survival were 89.1% and 92.6%, respectively, after a median follow up of 21 months. 35 In another study involving patients with surgically resected T1 EAC, the 5-year overall survival and 3-year disease-free survival were 62% and 80% respectively. 36 These data, in line with most surgical series 37 confirm that surgical resection does not prevent late distant recurrences of T1 esophageal cancer, with or without previous endoscopic resection. 34
Given the complication rates recently reported in the Netherlands after esophageal or gastric resection for cancer, 38 the complication rates after esophagectomy in our study can seem high. First, these results could be partly explained by a recruitment bias: indeed, a frequent reason for referring a patient for endoscopic resection is a poor performance status or the presence of multiple comorbid conditions making the patient a poor surgical candidate. 39 As confirmed by Zhang and colleagues, the morbidity and mortality are largely impacted by the patient’s general condition, with morbidity rates ranging from 17.9% to 61.5% and mortality rates from 1.8% to 23.1%, depending on the patients performance status. 40 Second, the surgical techniques were heterogenous. Minimally invasive esophagectomy was performed in only 40% of patients, and McKeown esophagectomy was performed in three patients (10% of cases), with important severe postoperative adverse events (2/3), whereas this surgical technique is typically dedicated to salvage surgery following chemoradiotherapy (CRT) in clinical practice. 24 However, the numbers we found are in line with the findings of a recent national survey on 3286 esophagectomies across France finding a 7.9% in-hospital mortality after esophagectomy. 41
The ESGE guidelines advise the consideration of CRT, along with surgery, after noncurative endoscopic resection. 9 Several small retrospective studies reported the outcomes of patients treated by CRT in this setting.42–47 The disease-free and overall survival ranged from 73% to 100% and 64% to 100%, respectively. Furthermore, a large prospective Japanese study involving 102 patients with noncurative endoscopic resection of a T1 SCC treated by two different CRT protocols found this treatment approach to be feasible with a 89.7% progression-free survival, and over 20% severe toxicity. 48 These findings, limited to SCC, indicate that CRT is an interesting approach with acceptable results and less treatment toxicity, particularly for patients with a poor performance status. Furthermore, CRT seemed to be less toxic than surgery: indeed, no treatment-related death was reported in any of these studies.42,44–48
To our knowledge, this is the first study to precisely report the outcomes of esophagectomy after a noncurative endoscopic resection, as defined by the ESGE. The limitations of our work include its retrospective design, a short follow up, a heterogeneous group in terms of histology and histoprognostic factors, a relatively small number of cases, and the absence of a control group of similar patients managed nonoperatively.
Conclusion
In this cohort, esophagectomy after noncurative endoscopic resection of early esophageal cancer allowed the resection of residual advanced cancer or lymph node metastases in 13% of cases, at the cost of 43% severe morbidity and 7% perioperative mortality. These data suggest that the patient’s general condition and the risk of lymph node involvement in superficial esophageal cancer should be carefully assessed in multidisciplinary meetings. Furthermore, the possibility of close follow up needs to be balanced with a highly morbid surgical management, in a setting where 63% of esophageal resections are tumor free.
Key summary
- Surgery is recommended in cases of noncurative endoscopic resection considering the risk of lymph node metastasis. - Surgery provides a high curative treatment rate after noncurative endoscopic resection.
- Esophagectomy in this clinical setting allowed the resection of advanced residual cancer in 13% of cases and lymph node metastases in only 7% of cases. - Risk of lymph node metastasis should be weighed against the mortality and morbidity rates of esophagectomy.