
Abstract
Background:
Acute-on-chronic liver failure (ACLF) is a common complication of cirrhosis characterized by single or multiple organ failures and high short-term mortality. Treatment of ACLF consists of standard medical care (SMC) and organ(s) support. Whether the efficacy of artificial liver support (ALS) depends on the severity of ACLF or on the intensity of this treatment, or both, is unclear. This study aimed to further assess these issues.
Methods:
We performed an individual patient data meta-analysis assessing the efficacy of Molecular Adsorbent Recirculating System (MARS) in ACLF patients enrolled in prior randomized control trials (RCTs). The meta-analysis was designed to assess the effect of patient severity (ACLF grade) and treatment intensity [low-intensity therapy (LIT), SMC alone or SMC plus ⩽ 4 MARS sessions, high-intensity therapy (HIT), SMC plus > 4 MARS sessions] on mortality.
Results:
Three RCTs suitable for the meta-analysis (n = 285, ACLF patients = 165) were identified in a systematic review. SMC plus MARS (irrespective of the number of sessions) did not improve survival compared with SMC alone, neither in the complete population nor in the ACLF patients. Survival, however, was significantly improved in the subgroup of patients receiving HIT both in the entire cohort (10-day survival: 98.6% versus 82.8%, p = 0.001; 30-day survival: 73.9% versus 64.3%, p = 0.032) and within the ACLF patients (10-day survival: 97.8% versus 78.6%, p = 0.001; 30-day survival: 73.3% versus 58.5%, p = 0.041). Remarkably, HIT increased survival independently of ACLF grade. Independent predictors of survival were age, Model for End-Stage Liver Disease (MELD), ACLF grade, number of MARS sessions received, and intensity of MARS therapy.
Conclusion:
HIT with albumin dialysis may improve survival in patients with ACLF. Appropriate treatment schedules should be determined in future clinical trials.
Introduction
Acute-on-chronic liver failure (ACLF) is a frequent syndrome in patients with cirrhosis that is characterized by local and systemic inflammation, impairment in cardiovascular function, mitochondrial dysfunction, and increased apoptosis. Clinically, it is associated with organ failure and high (22–74%) 28-day mortality.1–4 Unfortunately, no specific therapies exist, and current treatment is limited to that of associated complications and organ support.
Artificial liver support systems (ALS) that aim to provide temporary support of liver and kidney function have been evaluated in patients with ACLF. 5 Several randomized controlled trials (RCTs) evaluating the Molecular Adsorbent Recirculating System (MARS), which has been the most studied ALS device, have shown improvements in biochemical parameters and hepatic encephalopathy (HE) following MARS, but its effect on survival remains unclear.6–9 In this regard, several meta-analyses have shown discrepant results.10–12 Importantly, the potential time-dependent effect of MARS on survival and the identification of robust predictors of response could not be assessed in those meta-analyses, as they were not based on individual data. No prognostic stratification of patients was used either,13,14 as the trials were performed before the new characterization of the ACLF syndrome. 1
In this study, we performed a meta-analysis using individual patient data to overcome these limitations. Our aims were: To compare the effect of MARS plus standard medical care (SMC) versus SMC alone on survival; to identify predictors of mortality, including the severity of ACLF and the intensity of MARS therapy; and to evaluate the safety profile of MARS therapy.
Methods
Study selection
The current meta-analysis was designed to pool individual patient data from RCTs comparing MARS-SMC versus SMC alone in cirrhotic patients with acute decompensations. A comprehensive search of the literature (PubMed, EMBASE, CT registries, and the Cochrane Library) was performed according to the following strategy [‘ACLF’ OR ‘acute-on-chronic liver failure (Mesh)’] and (‘MARS’ OR ‘albumin dialysis’). Identification of trials, the definition of outcomes, data processing, and statistical analysis was carried out following a prespecified plan. RCTs considered for evaluation were analyzed independently by two authors who decided which trials were eligible according to the following criteria: They were published as full articles; a random allocation of patients with an acute decompensation of cirrhosis received either ALS with the MARS system or SMC; and data of survival as a primary or secondary outcome.
Four RCTs fulfilled the predefined inclusion criteria (Figure 1(a)). We had access to the individual patient data directly from the original case report form (CRF) in three trials.7–9 It was not possible to obtain accurate individual information from the fourth trial. 6 The number of patients included in the meta-analysis represented over 90% of the randomized patients in the four studies. Table 1 summarizes the main characteristics of the three RCTs selected.

(a) Searching strategy. * Studies were excluded because of the absence of a control group, or random allocation, or because the study included patients with acute liver failure. (b)Number of MARS sessions received in LIT (⩽4 MARS sessions) and HIT groups (⩾5 MARS sessions).
Design of the randomized controlled trials (RCT) comparing MARS plus standard medical care (SMC) versus SMC in patients with ACLF.

ACLF, acute-on-liver failure; DIC, disseminated intravascular coagulation; HE, Hepatic encephalopathy; HRS, Hepatorenal syndrome; INR, International normalized ratio; MARS, Molecular Adsorbent Recirculating System; SMC, standard medical care.
Only one of the three studies included in the meta-analysis was originally designed to find differences in survival. 9 In the remaining two studies the primary endpoint was the resolution of HE and a sustained reduction of bilirubin.7,8 The 30-day survival was recorded in the three studies, and the 90-day survival was also recorded in one of them. 9
The meta-analysis
Duration and number of MARS sessions were prespecified in all RCTs. Patients received up to 10 sessions of 6–8 h in 2 studies, while the maximum of sessions allowed in the third study was 5. As per the protocol of RCT, MARS therapy was discontinued when patients reached the endpoint of the study, presented sustained improvement or underwent liver transplantation.
The individual patient data was extracted directly from the CRF, pooled and verified by three of the authors. The database was recorded and checked for completeness and internal consistency.
The obtained information was analyzed to reclassify the patients according to the ACLF-CANONIC definition (Supplementary materials). Because several important data for the diagnosis or stratification of ACLF was absent or insufficiently described in the CRFs, the following assumptions had to be considered:
(1) In one RCT, 7 prothrombin activity instead of INR was available. Conversion of prothrombin time was performed to calculate INR.
(2) If information about the fraction of inspired oxygen (FiO2) was not recorded in the CRF, a value of 0.21 was assumed.
(3) Precise information on vasoactive drug use could not be retrieved from the CRFs in many patients. Therefore 2 points was the maximum chronic liver failure organ failure (CLIF-C OF) score assigned to circulatory failure. This assumption was taken because, according to the CANONIC study, it would rarely affect ACLF grading, since circulatory failure in patients with ACLF grades 1 and 2 is extraordinarily infrequent.
To explore the impact of the intensity of MARS therapy on survival, a post hoc analysis was carried out. Patients were combined into a single cohort and restratified into two different groups according to the number of MARS sessions delivered, LIT, and HIT. A cutoff of four treatment sessions (the median number of sessions in the MARS treated patients) was selected for stratification. Consequently, the HIT group included patients receiving five or more MARS sessions, whereas the LIT group included patients allocated to SMC and patients receiving four or fewer MARS sessions.
Outcomes
The primary outcome was 30-day survival. In addition, 10-day survival was considered as an estimation of the survival within the period of active organ support. Data for patients who were transplanted before reaching the 30-day follow up were censored as of the date of transplantation.
Secondary outcomes were changes in bilirubin, creatinine, and severity of HE 4 days after enrolment. The 4-day period was selected because it is included within the most suitable period (3–7 days after enrolment) for the prediction of prognosis in ACLF patients. 14
Assessment of adverse events
Two out of three RCTs included in the meta-analysis had a predefined system for notification and monitoring of adverse events (AEs). One investigator, blinded to the group of interventions, reviewed the original CRFs to classify AEs according to their severity and type.
Comparison with the CANONIC cohort
A comparison between the patients with ACLF included in the meta-analysis and the 303 patients included in the CANONIC study with ACLF at enrolment (including clinical characteristics, and 10-day and 30-day survival) was performed.
Statistical analysis
Continuous variables are described by mean (standard deviation), the normality of continuous variables was evaluated using a Kolmogorov–Smirnov test. Paired and unpaired Student’s t test, one-way analysis of variance (ANOVA) and the chi-squared test (χ2) were used as appropriate. The Kaplan–Meier method and the Breslow test were used to evaluate survival differences.
Univariate and multivariate Cox proportional hazard models were used to identify risk factors for survival. The variables with a p value < 0.1 were included in the multivariate models. As we specifically aimed to evaluate the impact of intensity of therapy and the severity of ACLF, we developed the following modeling strategy. First, we performed a model including the MELD score as a covariate that estimates the severity of the liver disease. Then, we developed a second model in the population in which the presence and severity of ACLF could be obtained. In this model, ACLF grade was included as the covariate that specifically estimates severity. Finally, we developed a model including the ACLF grade and the number of MARS sessions.
A logistic regression model was also fitted to estimate the probability of 30-day mortality in patients receiving LIT and HIT at different levels of severity, as measured by the CLIF-C ACLF score. 13
Statistical analyses were performed using SPSS version 21 (SPSS, Chicago, IL, USA). All p values were two-tailed. All of the results are reported as per protocol because the intention to treat analysis was not possible in two of the three studies. This meta-analysis was conducted in accordance with the PRISMA guidelines and was exempted from ethical evaluation by the local institutional review board.
Results
Patients
The final database consisted of 285 patients, 147 allocated to MARS treatment and 138 to SMC. Evaluation of the presence and grade of ACLF was possible in 201 patients (70.5% of the total sample). Among the patients in which ACLF could be evaluated, 36 patients (17.9%) had no ACLF at enrolment, 49 patients (24.4%) presented ACLF 1, 53 patients (26.4%) had ACLF 2, and 63 patients (31.3%) had ACLF 3. Therefore, ACLF was present in 165 patients (82.1%).
In total 13 of the patients included in the meta-analysis (4.6%) underwent liver transplantation within a 30-day period (SMC = 5 patients versus MARS = 8 patients; p = 0.477. LIT = 10 patients versus HIT = 3 patients; p = 0.563).
Overall, there were no differences between groups regarding the etiology and severity of the liver disease, presence, and severity of ACLF, or the number of organ failures (Table 2). Additionally, there were no differences between the LIT and the HIT groups, apart from the LIT group having a higher proportion of patients with cerebral failure (41.9% versus 25.3%; p = 0.013) and a lower proportion of patients with liver failure (77.6% versus 89.0%; p = 0.034) (Table 2). The severity of ACLF was also similar.
Characteristics of patients included in the meta-analysis. The first number in each column denotes the total number in which the evaluated parameter was available.
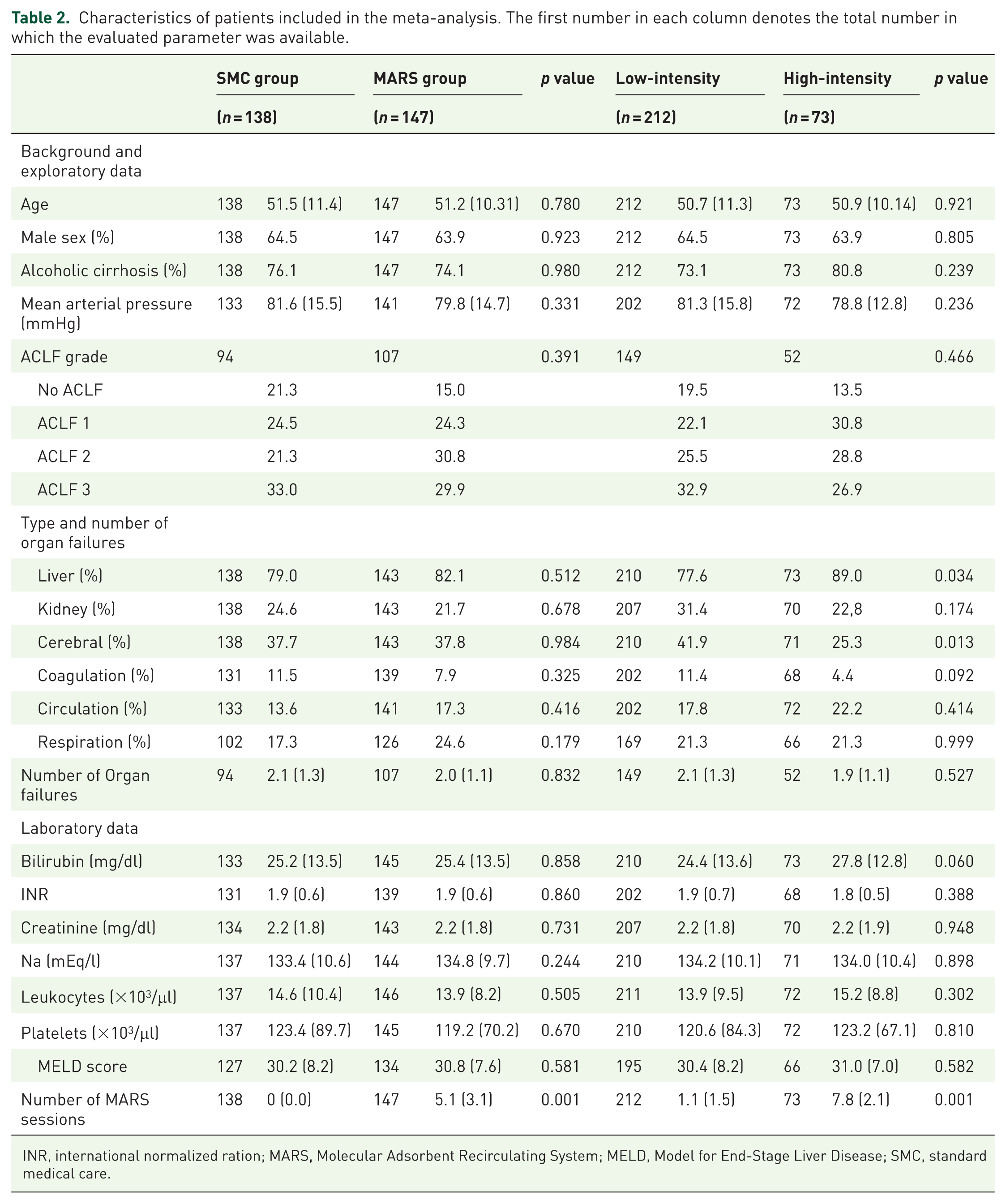
INR, international normalized ration; MARS, Molecular Adsorbent Recirculating System; MELD, Model for End-Stage Liver Disease; SMC, standard medical care.
Compared with the CANONIC study (Supplementary Table 1), the patients included in the present meta-analysis were younger (p = 0.001), had a higher proportion of alcoholic etiology (p = 0.011), presented more frequent liver, brain and respiratory failures (p = 0.001) and less kidney (p = 0.022) and coagulation (p = 0.003) failures, and had higher MELD and serum bilirubin (p = 0.001). Of note, patients in the meta-analysis also presented a lower prevalence of ACLF 1, a higher prevalence of ACLF 3 (p < 0.001), and a higher grade of systemic inflammation, as estimated by the white blood cells (WBC) (p = 0.001).
Effect of MARS and influence of treatment intensity on survival
The effect of MARS on survival was evaluated before and after the reclassification of the patients according to treatment intensity. For the latter, 212 patients were classified in the LIT group (138 patients treated with SMC and 74 with SMC plus ⩽4 sessions of MARS), and 73 in the HIT group (Figure 1(b)). When treatment intensity was not taken into account, the probability of survival was similar in patients treated with or without MARS [(10 day survival: 87.6% versus 86.1%; 30- day survival: 68.0% versus 65.4%); see Figure 2(a)]. However, reclassification by treatment intensity indicated that 30-day survival was higher in the HIT group than in the LIT group [(73.9% versus 64.2% p = 0.032); see Figure 2(b)). To ascertain whether the relationship between treatment intensity and survival was due to the potential influence of early mortality on the number of MARS sessions received rather than to a real beneficial effect of MARS, we performed a Cox regression analysis including the number of MARS sessions delivered as a continuous variable (Supplementary Table 2 model 3). Remarkably, the number of MARS sessions was also independently associated with survival [HR 0.90 (CI 95% 0.83–0.98); p = 0.021]. Additionally, the chronological relationship between MARS discontinuation and death was evaluated in all patients included in the LIT group. MARS discontinuation that occurred within 24 h prior to death was considered death-related (5 out of 28 patients). In the remaining patients, discontinuation occurred 2 days (two patients), 3 days (one patient), and 5 or more days (20 patients) before death, suggesting that MARS discontinuation might have been related to death in only a minority of patients. Furthermore, the probability of 10-day survival after excluding from the analysis the five patients with MARS discontinuation within 24 h prior to death remained higher in the HIT group (98.6% versus 81.8%, p = 0.012; Supplementary Figure 1). MARS therapy was also associated with improvements of diverse laboratory parameters and of HE on day 4 (see Supplementary materials).

(a) 30-day survival according to allocation to SMC or MARS. (b) 30-day survival according to allocation to LIT or HIT. (c) 30-day survival according to allocation to MARS-SMC or SMC in ACLF patients. (d) 30-day survival according to allocation to LIT or HIT in ACLF patients.
Effect of MARS and influence of the ACLF grade and treatment intensity on survival in patients in whom the presence of ACLF could be assessed and graded
Among patients where the presence of ACLF could be confirmed (n = 165), there were no significant differences in the 30-day (61.5% versus 63.5%) and 10-day (80.8% versus 86.5%) probability of survival between patients treated with SMC and those treated with MARS (Figure 2(c)). Remarkably, reclassification of ACLF patients according to treatment intensity indicated again that survival was improved in the HIT group compared with the LIT group [(10-day survival: 97.8% versus 78.6%, p = 0.001; 30-day survival: 73.3 versus 58.5, p = 0.041); see Figure 2(d)].
Patients with ACLF 1 and ACLF 2 in the HIT group showed significantly higher 10-day probability of survival (p = 0.001) than patients in the LIT group (Figure 3(a) and (b)). Among the patients with ACLF 3, those treated with HIT also showed a clear trend for a higher 10-day (p = 0.10) and a 30-day survival (p = 0.086) compared with those treated with LIT (Figure 3(c)). To further account for the reported nonlinear effect of ACLF on mortality, we estimated the 30-day probability of death in LIT, HIT and CANONIC patients (Supplementary Figure 2). Importantly, the curve corresponding to HIT patients was almost significantly shifted to the right (p = 0.074) when compared with LIT and CANONIC patients when the probability of death for patients belonging to HIT or LIT was estimated for the different values of the CLIF-C ACLF score, indicating that mortality tended to be lower in HIT patients for identical values of the score.
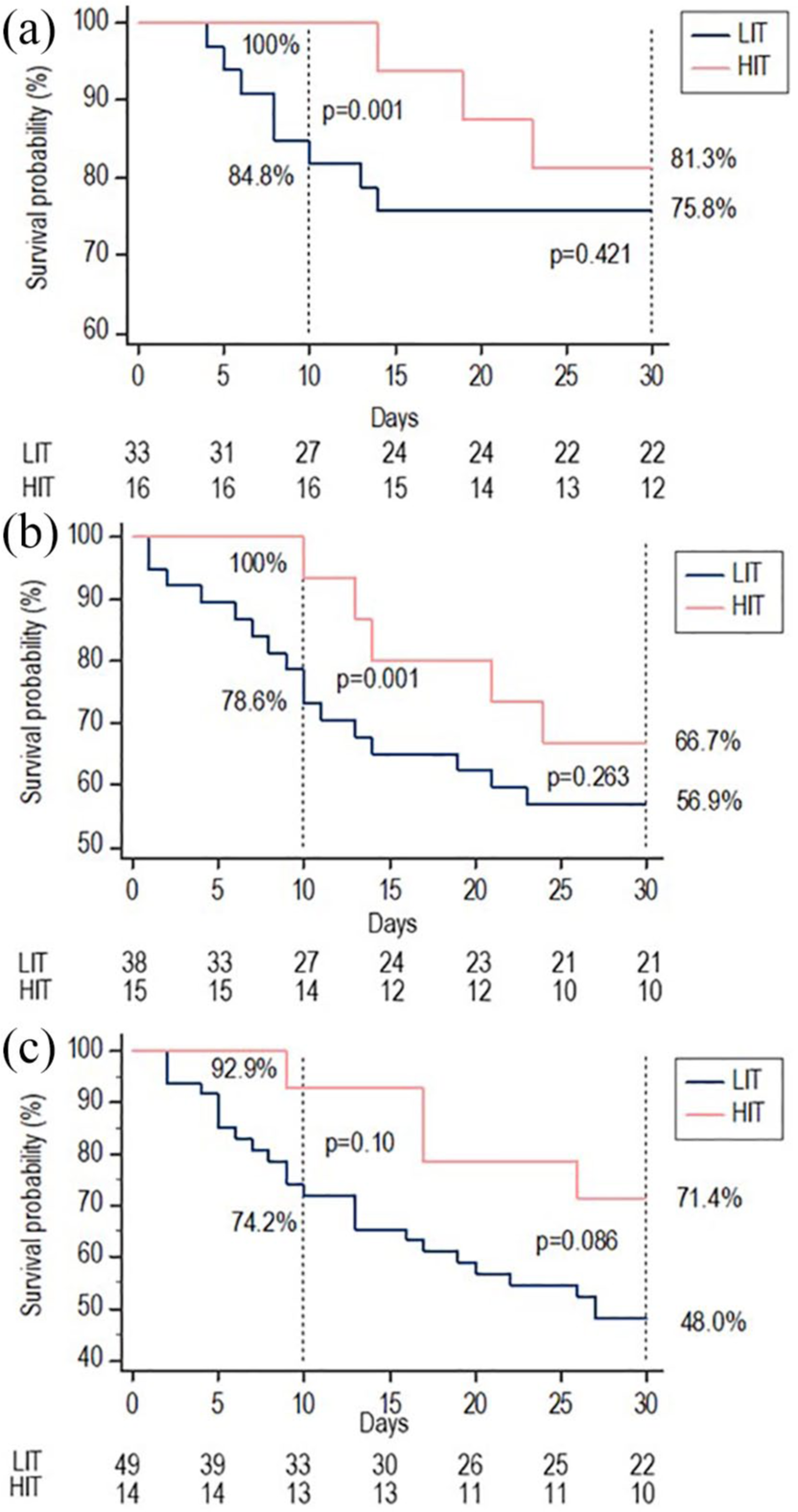
30-day survival according to allocation to LIT or HIT: (a) ACLF 1; (b) ACLF 2; (c) ACLF 3.
Survival in ACLF patients included in the CANONIC study and contextualization of findings in the ACLF patients included in the meta-analysis
Overall survival of patients included in the meta-analysis was similar to the CANONIC patients despite the increased ACLF severity in the former (Supplementary Table 1). Importantly, the probability of survival, when analyzed according to treatment intensity, was lower in the LIT group and higher in the HIT group compared with patients in the CANONIC study (10-day survival: CANONIC 80.5% versus LIT 75.1% versus HIT 95.6%; 30-day survival: 66.4% versus 58.5% versus 73.3%) (Supplementary Figure 3).
Variables associated with 30-day survival in patients with ACLF
The severity of ACLF, age, MELD score, creatinine, number of organ failures, the intensity of therapy, and the number of MARS sessions were associated with 30-day survival in univariate analysis (Supplementary Table 2). Due to the relatively high number of patients where ACLF could not be evaluated, we performed two different models to test the robustness of the association between intensity of therapy and survival, adjusting the 30-day survival by the severity of liver disease as estimated by MELD and by ACLF grade. As shown in Supplementary Table 2, the number of MARS sessions and also the intensity of treatment were independently associated with survival in both models.
The safety profile of MARS
Overall, the proportion of AEs in the MARS group and the SMC group was similar (45.7% versus 45.6%, p = 1; Table 3). Infection, bleeding, and development of severe coagulopathy was the most frequent AEs. Infection and severe coagulopathy were similarly distributed, but bleeding (of any source and severity) was significantly higher in the MARS group (24.1% versus 10.2%, p = 0.007). The proportion of deaths related to severe AEs, however, was similar in both groups (7.5% versus 11.1%; p = 0.482). The incidence of AEs was also similar in the LIT and HIT groups. Interestingly, the incidence and type of adverse effects were also similar in the SMC and MARS groups and in the HIT and LIT groups across the different ACLF grades (Supplementary Tables 3 and 4).
Adverse events.
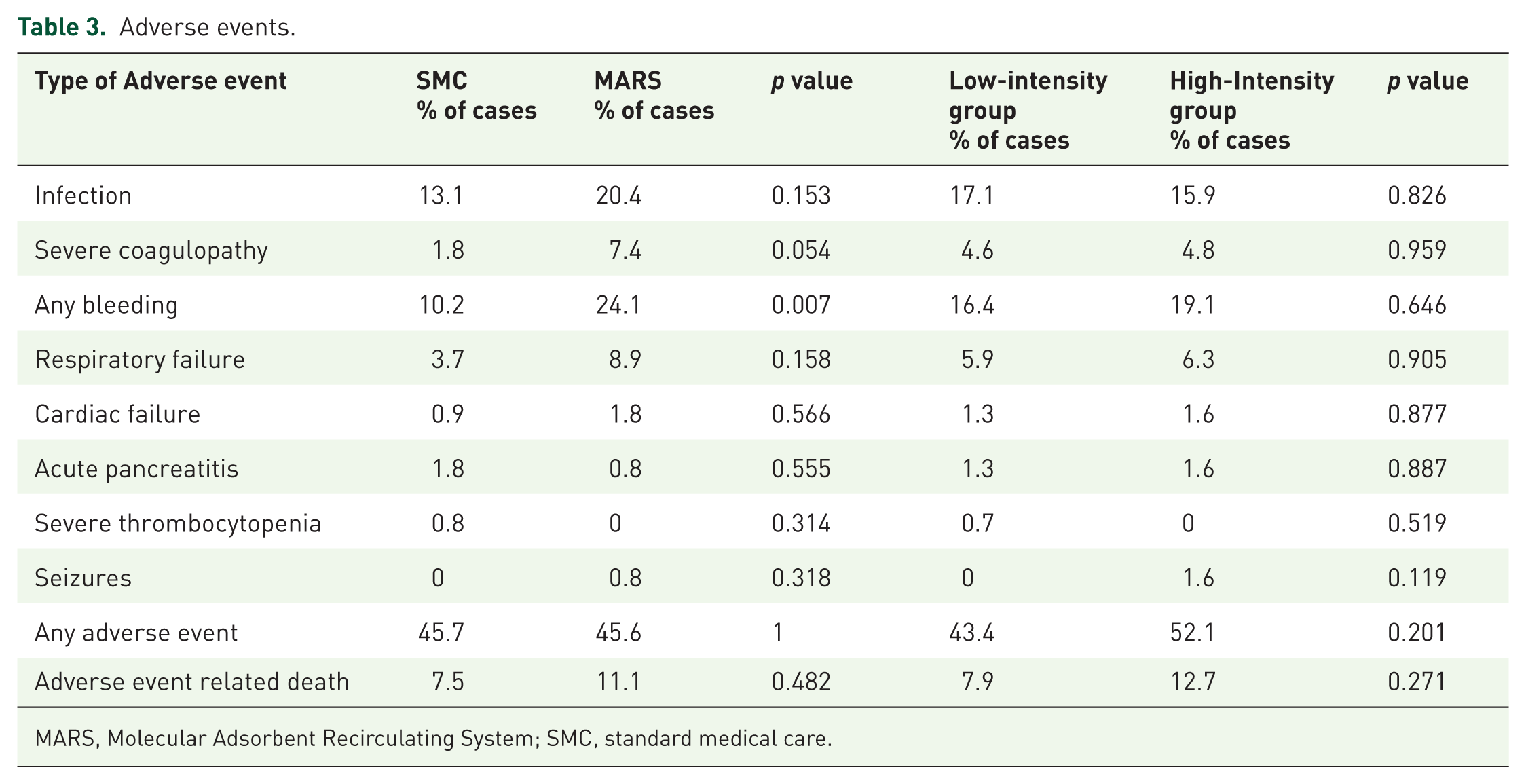
MARS, Molecular Adsorbent Recirculating System; SMC, standard medical care.
Discussion
ACLF has no specific treatment other than the management of the associated complications of cirrhosis and organ support and is a major worldwide healthcare problem.1,15–18 Initial investigations suggested that ALS systems, and MARS, in particular, provided clinical benefit, but this was not confirmed by subsequent RCTs.7–9 These later studies, which were performed prior to the CANONIC study, showed that MARS significantly improved liver, renal, and cerebral functions but it did not result in survival benefit. The present study was justified for several reasons: Exploring the effect of MARS through an individual patient data meta-analysis of patients with ACLF defined according to the CANONIC study may give essential information for the design of future RCTs assessing ALS systems; to assess the influence of the severity of ACLF on the efficacy of ALS systems; and to assess the intensity of MARS treatment as a determinant of response and survival in prior studies. Importantly, to the best of our knowledge, the last two factors have never been explored in prior RCTs or meta-analysis.
In all of the 285 patients included in the present meta-analysis, we confirmed several results previously described in the RCTs. First, MARS significantly improved serum bilirubin and creatinine levels within a short period of time (4 days). Second, MARS showed a consistent beneficial effect on brain function leading to a reduction in the proportion of patients with clinically-significant HE. Finally, the beneficial effects of MARS were not accompanied by the improvement of survival. These observations were also reproduced in 165 patients with a confirmed diagnosis of ACLF.
Meta-analyses are useful for the proposal of new hypotheses. Therefore, we performed a post hoc analysis to explore the potential effect of treatment intensity. Importantly, the number of MARS sessions was independently associated with survival in the multivariate analysis both in the whole group of patients and in patients with confirmed ACLF. In addition, patients who received a high number of sessions (more than four) presented a higher survival compared with those who received fewer sessions. These findings suggest that the use of albumin dialysis may prolong survival if given at an appropriate dosage. Interestingly, HIT with MARS improved survival independent of the severity of the syndrome in patients with confirmed ACLF, and was an independent predictor of survival in the multivariate analysis.
It is conceivable that the beneficial effect on survival in the HIT group may result from the fact that patients that remain alive longer can receive more MARS sessions. In contrast, our results suggest that the discontinuation of MARS treatment was unrelated to early mortality in most patients receiving LIT. Additionally, discontinuation of therapy was not related to a higher prevalence of adverse effects, because such prevalence was similar in the LIT and the HIT groups. Of note, the concept by which we defined the two groups of patients according to the ‘intensity of therapy’ refers to the absolute sum of effective MARS sessions, and it should not be confused with frequency or the technical issues of each single MARS treatment.
The use of ALS systems in cirrhosis has suffered from the negative impact of the lack of positive effects on survival obtained in the RELIEF study, but the current meta-analysis strongly suggests that this concept should be revisited. The CANONIC study has shown that ACLF is a heterogeneous condition that requires large and complex RCTs for treatment assessment. These RCTs should be sufficiently powered and should include age, etiology of cirrhosis, type of precipitating events, and number and type of organ failures as relevant covariates. Importantly, our meta-analysis suggests that treatment intensity should also be considered in the design of future clinical trials. Furthermore, two recent studies14,19 have shown that the probability of survival was similar in patients with grade 2–3 ACLF and in cirrhotic patients without ACLF undergoing early liver transplantation, suggesting that early liver transplantation may be indicated for patients with ACLF grade 2–3. The short-term improvement of survival observed in our meta-analysis in patients with ACLF receiving HIT opens the potential for the use of MARS in a more intensive way as a bridge for early liver transplantation.
The methodological approach based on individual patient data meta-analysis provides a more robust effect estimation and is a major strength of the present study. The comparison of characteristics and outcomes with the patients included in the CANONIC study gives further relevance to the results of the present work. As with all meta-analyses, however, the generalizability of the results to new populations and settings is limited, considering that data are based in RCTs with different inclusion and exclusion criteria. Several methodological issues should also be mentioned. (i) The diagnosis of organ failure was based on individual CRFs, but its estimation was retrospective and therefore it has risk of bias; in addition, organ failure could not be properly assessed in a considerable proportion of patients due to lack of information in the CRF. (ii) We cannot completely exclude a publication bias, although the comprehensive search we used makes this possibility unlikely. (iii) Grading of intensity of therapy was adopted post hoc and may have introduced a selection bias, but the independent value of the number of sessions observed in the multivariate analysis supports the importance of the concept. (iv) The main reasons for discontinuing MARS therapy could not be obtained in this meta-analysis precluding the possibility to characterize the relationship between MARS discontinuation and outcomes. (v) Our results cannot be directly extrapolated to other ALS systems. Finally, there was one trial that we could not obtain individual data information from, but the number of patients enrolled in that study was very low and it is thus unlikely to change our results.
In conclusion, the results of this new meta-analysis of pooled individual patient data indicated that MARS therapy improved liver, renal, and brain function in patients with ACLF but it did not have an impact on survival. However, a robust post hoc analysis suggested that MARS systems may have a beneficial effect on short-term survival in patients with ACLF if given at an appropriate dose. The effect of high-intensity MARS therapy was independent of other well-known prognostic factors such as MELD or the number of organ failures. These relevant factors should be considered in the design of new trials assessing the effect of ALS devices in patients with ACLF.
Conclusion
ACLF is a common complication of cirrhosis that severely impacts the natural course of the disease.
This individual patient data meta-analysis shows that albumin dialysis in patients with ACLF ameliorated liver, and renal function improved HE but did not significantly impact survival. However, a robust post hoc analysis suggests that patients who received the appropriate dosage may present a better survival. Adequately delivered albumin dialysis may have a potential beneficial effect in ACLF patients. A suitable dosage should be evaluated in future clinical trials.
Supplemental Material
MARS_supplementary_table_and_figures – Supplemental material for Meta-analysis of individual patient data of albumin dialysis in acute-on-chronic liver failure: focus on treatment intensity
Supplemental material, MARS_supplementary_table_and_figures for Meta-analysis of individual patient data of albumin dialysis in acute-on-chronic liver failure: focus on treatment intensity by Rafael Bañares, Luis Ibáñez-Samaniego, Josep María Torner, Marco Pavesi, Carmen Olmedo, María Vega Catalina, Agustín Albillos, Fin Stolze Larsen, Frederik Nevens, Tarek Hassanein, Harmuth Schmidt, Uwe Heeman, Rajiv Jalan, Richard Moreau and Vicente Arroyo in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
Rafael Bañares and Luis Ibáñez-Samaniego contributed equally to this work.
The EASL CLIF Consortium is supported by an unrestricted grant from Grifols.
Author contributions
RB and LI participated in the design and performance of the research, analysis of the data, and writing of the article. JT and CO participated in the performance of the research. MP provided statistical support. VC, AA, FL, FN, TH, HS, UH, RJ, and RM participated in the data acquisition and writing of the article. VA participated in the design and writing of the article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study has been partially funded by Baxter and a grant by Fondo de Investigación en Salud PI18/01901.
Conflict of interest statement
The authors declare that there are no conflicts of interest.
The statistical analysis has been performed by the Data Management Center of the European Foundation for the Study of Chronic Liver Failure.
Availability of data and material
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics approval and consent to participate
Each of the included studies in this meta-analysis obtained approval of a local ethics committee in accordance with local legislation. Patients or their next of kin signed informed consent forms. With regard to its retrospective design, the need for additional ethic committee approval was waived according to local legislation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.