
Abstract
Background:
The objective of this study was to analyse the prevalence of metabolic bone disease (MBD) in a cohort of Southern European patients with inflammatory bowel disease (IBD) and to identify associated risk factors in this population.
Methods:
We conducted a retrospective, both cross-sectional and longitudinal study of MBD, assessed by dual energy X-ray absorptiometry (DXA), among patients diagnosed with IBD and previously recognized risk factors for this complication from two referral Spanish institutions.
Results:
A total of 612 patients (58.6% diagnosed with Crohn’s disease) were included. Mean (SD) age was 44.9 (14.7) years; 71.7% of patients received at least one tapered dosage of corticosteroids before first DXA. MBD and osteoporosis were diagnosed in 66.4% and 21.4% of patients, respectively. At baseline, male gender, menopause and ulcerative colitis were found as independent risks factors for osteoporosis, whereas age, more than three IBD-related hospitalizations and previous steroid treatment were found as independent risks factors for MBD. A total of 261 patients had at least a second DXA and were included in the longitudinal study; median follow up was 56.4 months. Logistic regression model identified menopause, ulcerative colitis and baseline lumbar DXA T-score value, but not steroid treatment, as risk factors for worsening ⩾1 SD in follow-up DXA T-score. According to guidelines, all patients under treatment with corticosteroids received calcium and vitamin D supplements.
Conclusion:
MBD is a frequent complication in south-European IBD patients. Routine evaluation of bone density when risk factors are present, as well as calcium plus D vitamin prophylaxis in patients under corticosteroid treatment should be recommended.
Keywords
Introduction
Osteoporosis is a systemic skeletal disease characterized by diminished density and architectural disturbance of bone tissue, as a result of an imbalance between bone resorption and formation, and with a consequent increase in fracture risk. 1 Several factors may affect this balance, being involved in osteoporosis pathogenesis: female sex, advanced age, endocrine and nutritional disturbances, certain drugs such as corticosteroids, immobilization and comorbidities such as chronic inflammatory disorders. Bone mineral density, assessed noninvasively in sites such as spine and hip by dual energy X-ray absorptiometry (DXA), is the best predictor of bone fracture risk, especially if periodic measures are performed. Individual bone density values are most commonly expressed in standard deviation (SD) units, in relation to a reference young, healthy population (T-score); according to this, World Health Organization classifies bone mineralization in three categories: normal (⩾−1 SD), osteopenia (−1.01 to −2.49 SD) and osteoporosis (⩽−2.5 SD). 1
Osteoporosis is a well-known complication of inflammatory bowel disease (IBD). Indeed, the overall relative risk of bone fractures among IBD patients is significantly higher than in general population. 2 Osteoporosis is present in 13–42% of patients, 3 but osteopenia has been reported in up to 77% of patients with IBD. 4 Variations in these percentages may be found depending on geographical area; 5 in addition, some specific IBD-related factors might also be involved in metabolic bone disease (MBD) in this scenario: the type of IBD, the presence of persistent inflammatory activity periods, the development of flares requiring hospitalization and corticosteroids and previous history of intestinal resections leading to calcium and/or vitamin D malabsorption.6,7 Several studies have been conducted with the purpose of identifying risk factors, in order to establish therapeutic and preventive strategies and, overall, it seems that corticosteroid treatment is the most strongly associated variable with osteoporosis among IBD patients.
In 2000, British Society of Gastroenterology published the first guidelines on the management of osteoporosis in coeliac disease and IBD, 8 recommending bone mineral density measurement as an osteoporosis screening strategy in at-risk patients such as postmenopausal women, patients older than 60 years old and those who have received systemic corticosteroid therapy. These guidelines also recommended, for the first time in this clinical scenario, the prevention of bone loss while on corticosteroid treatment by ensuring an adequate daily intake of calcium (1500 mg) and vitamin D (800 units). Three years later, the American Gastroenterological Association published its own guidelines on osteoporosis in gastrointestinal diseases, including IBD, 9 and similar recommendations were suggested.
There are scarce data of MBD in large cohorts from Southern European countries; moreover, the effect of physician’s adherence to published guidelines in the development of osteoporosis among IBD patients has not been estimated. Thus, the objective of our study is to evaluate bone mineral density in a cohort of Southern European IBD patients from two tertiary hospitals and identify factors related to the development of MBD.
Patients and methods
Patients and study design
We conducted an observational, retrospective, both cross-sectional and longitudinal study to estimate the prevalence and risk factors of MBD (osteoporosis and osteopenia), based on first DXA performed after IBD diagnosis between 2002 and 2016, among high-risk (see below) IBD patients from two referral, tertiary centres in Madrid (HGUGM) and Ciudad Real (HGUCR), Spain. The aforementioned guidelines recommend evaluation of bone density using DXA in IBD patients with previously recognized risk factors for this complication: poor response to treatment or hospitalization due to IBD activity, extensive disease including upper gastrointestinal tract involvement in CD patients, short bowel syndrome, prolonged treatment with corticosteroids, menopause or male older than 55 years or previously diagnosed with hypogonadism. Both institutions follow these recommendations; nevertheless, owing to retrospective nature of the study and missing data we cannot assure full compliance of referral to DXA screening. Electronic clinical charts of IBD patients registered in our databases were reviewed, and clinical, endoscopic and radiologic information was included. Prescription data, including doses and duration of therapies, were confirmed from electronical clinical charts. Adherence has not been confirmed by objective methods, except for the case of biological therapies. Inclusion criteria were diagnosis of IBD (based on the usual clinical, radiological, endoscopic and histological criteria); age over 18 years at the time of the baseline densitometry; and at least one spine or hip DXA performed after IBD diagnosis. Exclusion criteria were bone mineral density expression only by Z-score; bone mineral density measurement in different location to lumbar spine or hip; time between baseline DXA and control DXA less than 2 years (for the longitudinal study); neoplasms that lead to withdraw immunosuppressive IBD treatment or chemotherapy; and pregnancy.
Cross-sectional study
Epidemiological and clinical data were collected (including smoking habits, history of fractures and usual medication that may act as confusion variables such as proton pump inhibitors, low molecular weight heparin, contraception pills and cancer chemotherapy) as well as specific data of IBD [type of IBD, Montreal classification for Crohn’s disease (CD) and extension for ulcerative colitis (UC), years from diagnosis, medical treatment and previous surgery] as potential independent factors for the worsening of the course of bone mineral density. Corticosteroid treatment was recorded as cumulative dose of prednisone, each tapered treatment was annotated and when methylprednisolone was used an equivalency 0.8 mg methylprednisolone = 1 mg prednisone was used to standardize dosing. Dosing used in both institutions was 1 mg/kg of weight/day (maximum 60 mg/day) of prednisone during 1 or 2 weeks, and a decrease of 10 mg/day each week until 20 mg per day, after this dose the decrease falls to 5 mg/day each week until suppression. Chronic treatment with calcium and vitamin D was also recorded. When this treatment was administered as cotreatment during steroids tapering therapy it was not annotated as chronic calcium and vitamin D treatment. Blood chemistry variables (25-hydroxy-vitamin D, calcium, albumin, parathyroid hormone, reactive C protein and fibrinogen) were also collected at the DXA date (±2 weeks).
Follow-up cohort assessment
The following parameters were retrieved: initiation or not of specific treatment for bone mineral disease after baseline DXA and type (calcium plus D vitamin, bisphosphonates or others), change or not in the specific treatment of IBD after baseline DXA and type [immunomodulators (IMM), anti-tumour necrosis factor (TNF)α agents, IMM plus anti-TNFα agents, surgery or others], need or not of intensification in the specific treatment of IBD, need or not of corticosteroids treatment and cumulative dose, and history of fractures. The blood chemistry variables collected were the same as for the baseline assessment.
Bone density measurements
DXA was performed using a Hologic densitometer, Discovery QDR series, and APEX 3.3.0.1 software. MBD was defined according to the World Health Organization 10 criteria, which bases the categorization of abnormality in an individual according to the number of SDs below the mean value for a young adult reference population (T-score): normal when the T-score is ⩾−1 SD; osteopenia if the lowest T-score (hip or spine) is between −1 and −2.49 SD, and osteoporosis if the lowest T-score (hip or spine) is ⩽−2.5 SD. The lumbar spine or hip T-score were used for the interpretation of bone mineral density data. In the follow-up cohort, those patients who had more than two DXA, the most recent DXA was chosen as control DXA.
Ethical considerations
The study was approved by the Institutional Ethics Committee (39/14, 24 March 2014). Data analysis was performed according to the Declaration of Helsinki. As the study utilized existing health data, a waiver of informed consent was granted by the Ethics Committee.
Statistical analysis
Results of continuous variables are expressed as mean and SD, in the case of a normal distribution, or as median and interquartile range (25th percentile; 75th percentile) if not. Analysis of the normal distribution was performed with Kolmogorov–Smirnov test. For categorical variables, results are expressed as frequencies and percentages. To evaluate mean differences between two or more groups, parametric [Student’s t test or analysis of variance (ANOVA)] or nonparametric (Mann–Whitney or Kruskal–Wallis) were used depending on the normal distribution or total number of patients in each group. Association between categorical variables were analysed by means of chi-squared or Fisher tests; to measure the strength of the associations, odds ratios (ORs) with their confidence intervals (CIs) were calculated. Association between quantitative variables were assessed with Pearson or Spearman correlation coefficients. A logistic regression multivariate analysis was performed to assess independent predictive factors of MBD and osteoporosis (dependent variables) in IBD patients. All statistically significant variables (p < 0.1 for this purpose) in univariate analysis and those that although not significant are clinically or physiologically relevant were included in the multivariate analysis; those with very low incident cases were not included. The final model was obtained following a backwards stepwise selection using maximum likelihood estimation, in which variables are removed based on likelihood ratio test; final statistically significant variables are presented. Statistical analysis was performed with IBM SPSS Statistics package for Windows (Version 21.0. Armonk, NY: IBM Corp.). p values < 0.05 were considered statistically significant.
Results
Cross-sectional study
Baseline clinical characteristics
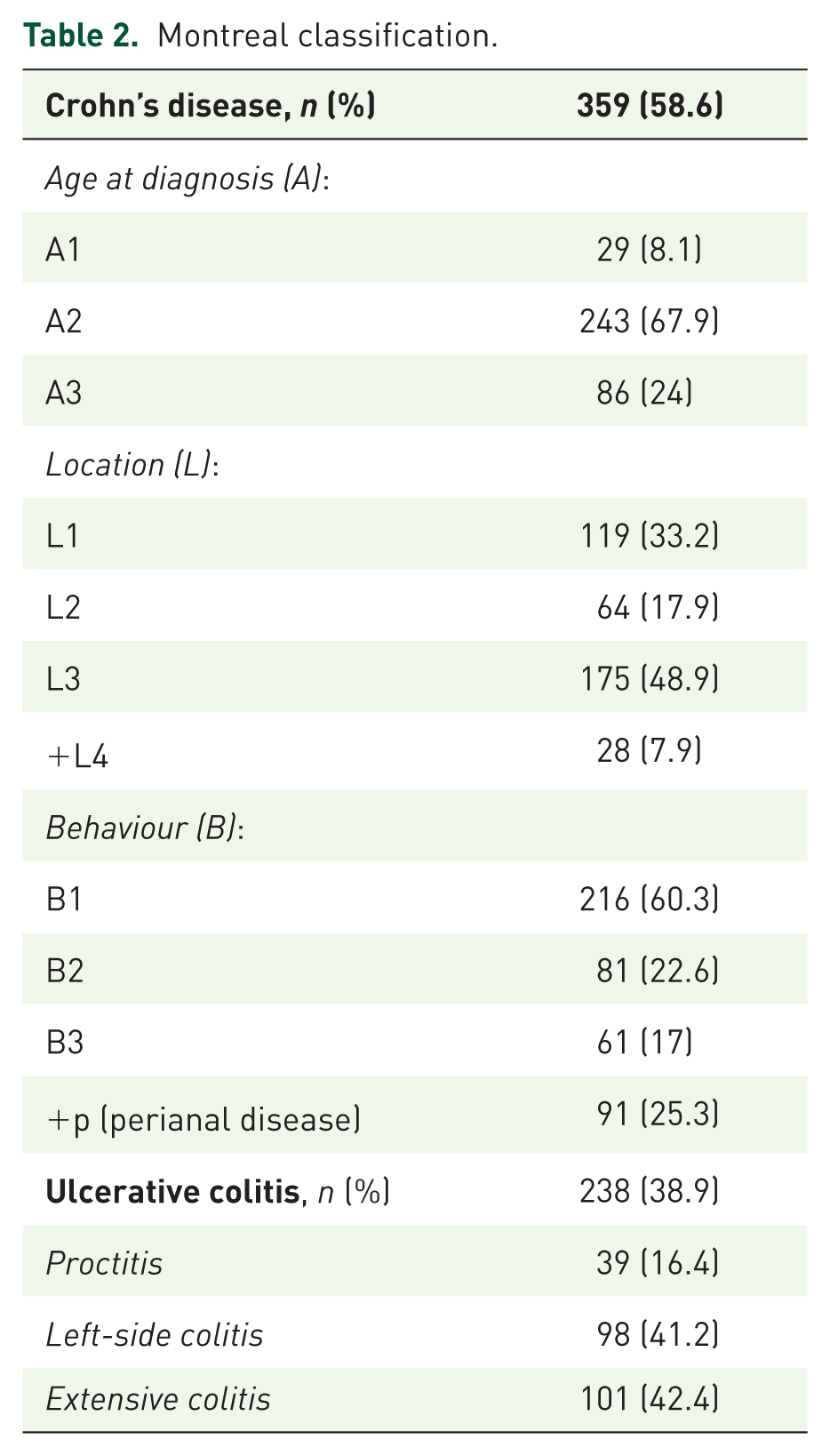
A total of 1619 [1152 from Hospital General Universitario Gregorio Marañón (HGUGM) and 467 from Hospital General Universitario de Ciudad Real (HGUCR)] consecutive IBD patients attended between 2002 and 2014, were evaluated; 612 eligible patients with risk factors for MBD and at least one DXA were finally included in the study (Figure 1): 43.1% of patients were male; mean (SD) age was 44.9 (14.7) years. CD was diagnosed in 359 (58.6%) patients, UC in 238 (38.9%), and indeterminate colitis (IC) in 15 (2.4%). Mean evolution time from diagnosis was 9.7 years. Clinical characteristics, and previous and active treatments of patients at the moment of basal DXA are summarized in Tables 1 and 2. Patients diagnosed with CD were significantly younger [42.1 (13.9) versus 48.6 (15), p < 0.001] and had a significantly higher rate of active smoking (34.3% versus 15.6%, p < 0.001), IMM (49.7% versus 37.8% p = 0.011) and biologic treatment (27.9% versus 14.7%, p < 0.001), hospital admissions (51.4% versus 38.6%, p = 0.026) and previous surgery (42.1% versus 9.7%, p < 0.001) than those diagnosed with UC. A higher proportion of menopausal women was found among UC compared with CD patients (24.6% versus 16%, p = 0.004). A total of 439 patients (71.7%) received at least one tapered dosage of corticosteroids before DXA, with a mean (SD) cumulative dose of 4021.5 (2979) mg of prednisone or equivalent; 143 patients received calcium and vitamin D treatment at least 3 months before first DXA, and 19 patients received bisphosphonates.

Flowchart.
Clinical characteristics of the cohort (CD, 359 patients; UC, 238 patients; IC, 15 patients).

CD, Crohn’s disease; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; IC, indeterminate colitis; IBD, inflammatory bowel disease; PPI, proton pump inhibitor; UC, ulcerative colitis.
Montreal classification.
Prevalence of MBD
Following the above-mentioned criteria, MBD (both osteopenia and osteoporosis) was diagnosed in 406 (66.4%) of patients; osteoporosis was diagnosed in 131 (21.4%) patients. Mean (SD) spine T-score was −1.53 (1.16), whereas mean (SD) hip T-score was −1.32 (0.9). Osteoporosis prevalence was higher among UC than CD patients (27.7 versus 17%, p = 0.02). Previous nontraumatic bone fracture occurred in 2.6% of the cohort. When cohorts from both institutions were compared, no statistically significant differences in MBD prevalence were found (data not shown).
Univariate analysis of risk factors for MBD in patients with IBD
Raw data of patients’ characteristics included in all three categories of MBD, normal, osteopenia and osteoporosis, are listed in Supplemental Table 1. Univariate analysis based on the categorization of alteration of bone mineral density (normal, osteopenia or osteoporosis) was carried out (Supplemental Table 1), and showed that age (p = 0.001), menopause (p < 0.001), previous fracture (p = 0.014) and age of onset (p = 0.023) were statistically significant risk factors for worse categorization of bone mineral density. No previous fractures were observed among patients with normal bone mineral density. Biochemical parameters and other variables of the Montreal classification were not significantly associated with the presence of bone mineral disease. Treatment with proton pump inhibitors (PPIs) was significantly associated (p = 0.019) with worse categorization of bone mineral density. However, previous steroid treatment was not significantly associated with a worse bone mineral density (p = 0.476).
Multivariate (logistic) regression analysis of risk factors for MBD
To identify the risk factors that influenced in the baseline DXA, two multivariate analysis were performed for two dependent variables, osteoporosis (Table 3) and MBD (both osteoporosis and osteopenia; Table 4), as follows: first, each independent variable was tested in the univariate analysis, and those statistically significant (p < 0.1 for this purpose) or those clinically or physiologically relevant were included in multivariate analysis. We used a backwards strategy and after deleting the variable less significant in each step the variables finally selected and their OR, CI and p value are shown. Female sex (OR 0.430, 95% CI = 0.213–0.867; p = 0.018) and albumin (OR 0.474, 95% CI = 0.251–0.898; p = 0.022) were identified as protective factors for osteoporosis; on the other hand, menopause (OR 2.165, 95% CI = 0.997–4.7; p = 0.051), ulcerative colitis diagnosis (OR 2.619; 95% CI = 1.438–4.77; p = 0.002) and treatment with calcium and vitamin D (OR 2.123; 95% CI = 1.129–3.99; p = 0.019) were found as risk factors for osteoporosis. Treatment with calcium and vitamin D is interpreted as a collinear variable, as risk patients are more likely to receive this treatment. Furthermore, we performed the same analysis with MBD (i.e. osteopenia and osteoporosis) as a dependent variable (Table 4). IMM therapy was identified as a potential protective factor for MBD (OR 0.609; 95% CI = 0.372–0.997; p = 0.049) whereas age (per year, OR 1.031; 95% CI = 1.031–1.049; p = 0.000), more than three IBD-related hospitalizations (OR 3.217; 95% CI = 1.23–8.415; p = 0.017), corticosteroids (OR 1.948; 95% CI = 1.147–3.309; p = 0.014) and treatment with calcium and vitamin D (OR 2.073; 95% CI = 1.13–3.804; p = 0.019) were identified as risk factors.
Univariate and multivariate (logistic) regression analysis of risk factors for metabolic bone disease. Dependent variable: osteoporosis. All statistically significant (p < 0.1 for this purpose) variables in univariate analysis and those clinically or physiologically relevant were included in the multivariate analysis (highlighted in bold in the univariate column). A backwards strategy was used, and final statistically significant variables and their OR, CI and p value are presented.

CI, confidence interval; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; IMM, immunomodulator; OR, odds ratio; PPI, proton pump inhibitor; PTH, parathyroid hormone.
Univariate and multivariate (logistic) regression analysis of risk factors for metabolic bone disease. Dependent variable: metabolic bone disease (osteopenia and osteoporosis). All statistically significant (p < 0.1 for this purpose) variables in univariate analysis and those clinically or physiologically relevant were included in the multivariate analysis (highlighted in bold in the univariate column). A backwards strategy was used, and final statistically significant variables and their OR, CI and p value are presented.

CI, confidence interval; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; IMM, immunomodulator; OR, odds ratio; PPI, proton pump inhibitor; PTH, parathyroid hormone.
Longitudinal study
Baseline characteristics of the cohort
A total of 261 (42.6%) of the 611 patients, had at least a second DXA throughout follow up (Figure 1). Median (range) follow up between first and last DXA was 56.4 months. A total of 41.6% of patients required IBD treatment intensification (adding an immunomodulator, an anti-TNF or increasing biologic dose) during follow up. Rate of intensification and need for steroids were higher among CD than UC patients (51.8% versus 31%, p < 0.001; and 29.4% versus 23%, p = 0.035, respectively). A total of 72.3% of patients were treated with calcium plus vitamin D supplements, and 22.2% with bisphosphonates during the follow up.
Analysis of patients lost in follow up
The following variables of the 351 (57.4%) patients not included in the longitudinal study due to lack of control DXA were analysed: age, sex, T-score in column and hip at baseline, categorization of bone mineral disease according to WHO (normal, osteopenia and osteoporosis) at baseline, menopause, treatment with corticosteroids and history of pathological fractures. T-score of the spine or hip in the baseline DXA (p < 0.001), number of patients with a normal baseline DXA (p = 0.004) and proportion of males (p < 0.001) were significantly higher in those patients who do not have a control DXA than in those who are included in the longitudinal study.
Long-term evolution of bone mineral density in IBD patients
Bone mineral density at lumbar spine slightly but significantly improved during the follow up (T-score from −1.53 ± 1.16 to −1.36 ± 1.18, p = 0.001); improvement in density at hip did not reach statistical significance (−1.32 ± 0.96 to −1.28 ± 1.05, p= 0.418). The course of bone mineral density in the hip for CD showed a statistically significant improvement (p = 0.003). Furthermore, we carried out two multivariate (logistic) regression models in order to identify factors that influenced these changes: first, an assessment as the worsening in the bone mineral disease classification (from normal to osteopenia or osteoporosis, and from osteopenia to osteoporosis) (Table 5); and second, as a decrease ⩾ 1 SD in hip or lumbar T-score (Table 6). Thirty-four (5.6%) of the 183 patients included in the follow up who presented normal values or osteopenia in baseline DXA presented a worsening in the control DXA. Supplemental Table 2 shows the univariate analysis of the longitudinal study comparing the group of patients who experienced worsening of MBD category and the group who did not. The ‘worsening of category’ group has a greater proportion of patients diagnosed with UC (p = 0.015), and lower proportion of patients under corticosteroid (p = 0.047) and biologic treatment (p = 0.025) previously to first DXA. Following the same approach as in the cross-sectional study, we performed a multivariate logistic analysis (dependent variable: worsening of MBD category) menopause (OR 18.072; 95% CI = 3.924–83.240; p = 0.000) and baseline lumbar DXA T-score value (OR 7.434; 95% CI = 2.697–20.491; p = 0.000) were identified as risk factors of worsening of MBD category (Table 5). On the other hand, 30 (11.5%) of the 261 patients included in the follow-up analysis presented a decreased in ⩾1 SD in hip or lumbar T-score in the control DXA. The multivariate (logistic) regression model identified menopause (OR 9.467; 95% CI = 2.411–37.169; p = 0.001), UC (OR 6.813; 95% CI = 1.82–25.503; p = 0.004) and baseline lumbar DXA T-score value (OR 2.981; 95% CI = 1.427–6.228; p= 0.004) as risk factors for worsening ⩾1 SD in follow-up DXA T-score. According to guidelines, all patients under treatment with corticosteroids received prophylaxis with calcium and vitamin D.
Univariate and multivariate (logistic) regression analysis of risk factors associated with worsening of metabolic bone disease category (n = 34). All variables that are statistically significant (p < 0.1 for this purpose) in univariate analysis and those that although not significant they are clinically or physiologically relevant were included in the multivariate analysis, and are highlighted in bold in the univariate column. A backwards strategy was used, and final statistically significant variables and their OR, CI and p value are presented in the multivariate column.

CI, confidence interval; CKD, chronic kidney disease; DXA, dual energy X-ray absorptiometry; COPD, chronic obstructive pulmonary disease; IMM, immunomodulator; OR, odds ratio; PPI: proton pump inhibitor; PTH, parathyroid hormone.
Univariate (left) and multivariate (right) analysis (logistic) regression analysis of risk factors associated with decrease ⩾1 SD in hip or lumbar T-score (n = 30). All variables that are statistically significant (p < 0.1 for this purpose) in univariate analysis and those that although not significant are clinically or physiologically relevant were included in the multivariate analysis, and are highlighted in bold in the univariate column. A backwards strategy was used, and final statistically significant variables and their OR, CI and p value are presented.

CI, confidence interval; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; DXA, dual energy X-ray absorptiometry; IMM, immunomodulator; OR, odds ratio; PPI, proton pump inhibitor; PTH, parathyroid hormone.
Influence of IBD and concomitant treatments in the course of bone mineral density
We further investigated the course of bone mineral density of IBD patients with osteopenia who were under calcium (1000 mg) plus cholecalciferol (800 UI) supplements at least 3 months before baseline DXA and continued during the follow up, showing that mean (SD) hip T-score significantly improved [0.219 (0.597) versus −0.033 (0.734), p < 0.005]. A tendency to lumbar spine improvement [0.296 (0.861) versus 0.115 (0.760), p > 0.05] was also shown, but without statistical significance.
We also analysed the evolution of bone mineral density of IBD patients with osteoporosis who were under bisphosphonate treatment during the follow up. Compared with nontreated patients, mean hip T-score improved during the follow up (0.324 (0.247) versus 0.030 (0.719) points, p = 0.039). No significant improvement in lumbar T-score (0.407 (0.884) versus 0.115 (0.2792) points, p = 0.42) was found. The course of bone mineral density of nine patients who started bisphosphonate after osteoporosis diagnosed in baseline DXA was also analysed and we found an improvement in the hip and the lumbar T-scores, but did not reach statistical significance (−2.162 versus −1.875 and −2.812 versus −2.262 respectively; p > 0.05).
Regarding specific IBD treatments, the evolution of bone mineral density was also evaluated in 22 patients with bone mineral disease who intensified their treatment to an anti-TNF treatment after baseline DXA, but changes between both bone densities were not statistically significant. In the same way, the evolution in bone mineral density was evaluated in those 12 patients whose IBD treatment was intensified after control DXA to treatment with anti-TNF and AZA, and a statistically significant increase in the lumbar T-score was found (−1.97 versus −1.12, p = 0.002).
Discussion
Osteoporosis is an architectural disorder of the bone, characterized by reduced mass affecting both cortical and trabecular bone, and that confers a higher risk of fractures. Osteoporosis is a frequent condition in the general population: in Spain, its prevalence among women older than 45 years ranges between 9.1% and 36.5%,11,12 whereas in men older than 50 years it ranges between 1.1% and 14.9%.13,14 Nevertheless, these numbers are markedly lower in the younger population: as an example, a Spanish study that included women younger than 45 years reported a prevalence of 0.17% when mineral density was measured in the femoral neck, and of 0.34% when assessed in the lumbar spine. 15
In the present study, describing the largest European cohort of IBD patients in whom bone density is analysed, osteoporosis was diagnosed in 21.4% of patients. Therefore, the prevalence of osteoporosis in IBD seems to be significantly higher than in an age-matched general population. Such a high prevalence, considering that mean age of the cohort is 44.9 years, is similar to reports from other studies from Southern European countries.16–18 Nevertheless, it is mandatory to consider that the present and the vast majority of previous studies include selected patients from referral centres; that is, patients with risk factors for the development of MBD such as a more severe intestinal disease; this fact might explain, at least in part, the wide variability of prevalence rates reported in the literature, ranging from 13% in a population-based Dutch study 19 to 42% of IBD patients in hospital-based cohort from Israel. 20 In addition, such differences in severity and prevalence of MBD might be related, among other factors, with the severity of the underlying disease, in our study only patients with previously recognized risk factors for MBD are included, and with region of living reflecting differences in prevalence of vitamin D deficiency due to dietary intake and sun exposure. Nevertheless, studies performed in Southern European regions, or in a country next to the equator such Sri Lanka 21 found similar prevalence rates of osteoporosis among IBD patients than other reports from northern European countries.19,22,23 In contrast with the majority of previously published studies,24,25 we found a higher MBD prevalence in UC compared with CD, despite the fact that CD patients had a significantly higher rate of active smoking, IMM and biologic treatment, hospital admissions and previous surgery than those diagnosed with UC. Nevertheless mean age of UC patients and proportion of postmenopausal women in our study were significantly higher than in CD affected individuals; and, as in the present report, age has been uniformly described as a risk factor for the development of MBD in IBD patients.17–19,21,26
Lower bone mineral density in IBD patients may be the consequence of the development of the skeleton during childhood and adolescence, in the case of paediatric-onset IBD, or excessive bone loss thereafter, due to malabsorption or to an increased bone resorption rate. 4 Thus, IBD patients are at subsequent higher risk of MBD due to corticosteroid treatment, immobilization due to hospitalizations, nutritional deficiencies and systemic inflammation; in fact, we have identified the albumin level as a protective factor for osteoporosis, and more than three hospitalizations in the last 5 years as a risk factor of MBD. Several studies, especially those published before 2000, suggest that worsening of bone density is associated with corticosteroid therapy in IBD patients.20,23,25–31 In the present study, corticosteroid therapy has been identified as a risk factor for MBD (both osteopenia and osteoporosis), but not for osteoporosis, in the cross-sectional study. Nevertheless, in the longitudinal study, with a mean follow up of more than 4.6 years, corticosteroid treatment seems to be a protective factor for the decrease ⩾1 SD in hip or lumbar T-score in the univariate analysis (OR 0.246; CI 95% = 0.112–0.539, p = 0.000), although this association disappears when the elected variables are included in the model. As mentioned previously, in the year 2000 the British Society of Gastroenterology published its recommendations about osteoporosis and IBD. 8 They encouraged evaluating bone density in IBD postmenopausal women, men aged 55 or more, in patients under corticosteroid treatment and when a fragility fracture is diagnosed. General measures as advising exercise, adequate dietary calcium intake, quit smoking and diminish alcohol intake were also suggested. They also recommended prevention or treatment of bone loss while on corticosteroid treatment, keeping to a minimum duration of therapy and prescribing concurrently 800 units of vitamin D daily. Since then, cotreatment with steroids and vitamin D is a standard of practice in our units. The American Gastroenterological Association guidelines 9 also recommend vitamin D cotreatment while on corticosteroids, and in all patients with proven osteoporosis or at high risk for osteoporosis. Finally, European Crohn and Colitis Organization (ECCO) guidelines 32 recommend adding calcium and vitamin D in patients with corticosteroid treatment if the duration of therapy is likely to be more than 6 weeks (but suggested in all patients), as well as other patients at risk of bone fracture as osteoporosis and osteopenia. Therefore, the results found in our study, on which every included patient under steroid treatment received concomitant supplements of calcium plus vitamin D, support the fact that adhering clinical practice guidelines by treating physicians may reduce steroid-related bone loss. In our study, medical prescription of this cotreatment was confirmed by chart review in every patient, in contrast with other studies in which calcium and vitamin D supplementation prescription is around 53–58%. 33 However, the adherence to the therapy was not controlled by specific methods. Adherence to calcium and vitamin D supplements in postmenopausal women is around 70% in previous studies. 34
On the other hand, thiopurine treatment, both in monotherapy and in combination with anti-TNFα agents, has been previously described as a protective factor for MBD among IBD patients.35,36 Our cross-sectional study confirmed this beneficial effect of IMM, although we could not demonstrate it in the longitudinal study; this fact could be related with an insufficient sample size. Moreover, omeprazole treatment was associated with osteoporosis in our univariate analysis, but multivariate analysis failed to confirm this detrimental effect in both cross-sectional and longitudinal studies. Although PPIs have been associated with hip fractures in the general population, 37 precise mechanisms by which it develops are not clear, as there is no a defined relationship with calcium absorption and risk of osteoporosis.38,39 In all the studies, the magnitude of the association is modest and could be related to confounding factors. Our observation of diminution of hip T-score associated with omeprazole might be a consequence of an additive effect of disease activity; PPIs are drugs often used as gastroprotective cotreatment when administered simultaneously with potential gastro-lessive drugs, including steroids. Anyway, this finding deserves further investigation.
This study has several weak points to consider. It is a retrospective evaluation, from two referral centres with probable sample bias and many excluded patients due to missing data; an important confounding variable such as body mass index was not recorded in every patient and has not been included in the analysis. The retrospective evaluation of the selected high-risk population might imply selection bias as the physicians may have missed some high-risk patients due to personal interpretation of the risk factors. On the other hand, IBD activity, a key factor related to MBD development, systematically measured by standardized clinical and endoscopic scores should have been considered; the retrospective nature of our study prevented us to reliably conclude about this point, but further studies considering these scores and MBD are guaranteed. However, the quite big sample number may permit a high-confidence extrapolation. In summary, the present study confirms that MBD is a frequent complication in southern European IBD patients. Special attention must be paid to elderly and male patients, UC patients and those requiring corticosteroids or hospitalizations. Early evaluation of bone density, and calcium and vitamin D prophylaxis while on corticosteroid treatment should be carried out in every IBD patients at risk for MBD.
Supplemental Material
Supplemental_Material – Supplemental material for Metabolic bone disease in patients diagnosed with inflammatory bowel disease from Spain
Supplemental material, Supplemental_Material for Metabolic bone disease in patients diagnosed with inflammatory bowel disease from Spain by José Miranda-Bautista, Cristina Verdejo, Alicia Díaz-Redondo, Irene Bretón, José M. Bellón, María Dolores Pérez-Valderas, Aránzazu Caballero-Marcos, Marta de Dios-Lascuevas, Elena González-Río, Cristina García-Sánchez, Ignacio Marín-Jiménez, Rafael Bañares and Luis Menchén in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
José Miranda-Bautista and Cristina Verdejo contributed equally.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Spanish Ministry of Health (Instituto de Salud Carlos III -ISCIII- FIS 13/02555 and 16/02096 and CIBEREHD) to LM.
Conflict of interest statement
LM and IM-J received unrestricted grants from MSD and Abbvie, and served as advisory board members for MSD, Abbvie, Pfizer, Janssen and Takeda. The other authors have no conflicts of interest, financial or otherwise, to declare with respect to this work.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.