
Abstract
Inflammatory bowel disease (IBD) is increasingly prevalent within western societies. Its complex and chronic facets in addition to its increasing prevalence place a great economic burden on our healthcare systems. Our aim was to estimate the national prevalence of IBD through predictive models. We used prevalence data which spans the years 2003–2007 to estimate prevalence until 2030 by means of four forecasting methods. Prevalence rates are estimated to be 4–6-times higher in 2030 when compared with 2003 with an average annual percent change of 5%. IBD is poised to have a substantial impact on healthcare systems in the near future, given its rapidly increasing prevalence. Forecasting methods will allow for a proactive stance on the development of health policies that will be needed to provide high quality and cost-effective care to these patients, while ensuring the economic viability of healthcare systems.
Introduction
Inflammatory Bowel Disease (IBD) is a chronic immunologically mediated disorder of unknown etiology comprising Crohn’s disease (CD) and ulcerative colitis (UC). It is estimated to affect up to 0.8% of the general population of western nations, 1 with accelerating incidence in newly industrialized countries whose societies have become more westernized due to rapid socioeconomic development. 2 Moreover, given its chronic nature, early onset, and low mortality, IBD prevalence has been increasing at a higher rate than incidence. This phenomenon is called compounding prevalence.3–5
In addition, IBD is associated with a considerable economic burden, 6 mostly due to the use of biologic therapy as well as the clinical and surgical hospitalizations that stem from the unpredictable relapsing and remitting course of the disease. 7 Consequently, healthcare systems and society will be progressively burdened by the increasing prevalence of IBD.2,5
Prediction modeling will allow for a proactive stance on the development of health policies that will be needed to tackle the impact of the increasing prevalence of IBD and the consequent challenges faced by healthcare systems.
In this short report, we follow up on the work of Azevedo and colleagues 8 in order to assess the evolution of IBD prevalence in Portugal by means of several forecasting methods.
Short report (methods + results)
Methods
For our dataset, we used the IBD prevalence estimates of Azevedo and colleagues 8 which span from 2003 to 2007. Prevalence data were then predicted from 2008 to 2030 by using four methods:



α and

These naïve forecasting methods (DM, ETSM and TM) were chosen due to the size and quality of our dataset and implemented using the forecast package in R.11,12 Accuracy tests were performed in order to evaluate the fitting of the data for all methods apart from the MA method which is a simple moving average calculation (Supplementary Table 1).
Prediction intervals (PIs; 80% and 95%) were used in the visual display of the DM, ETSM and TM methods. Confidence intervals (CIs; 80% and 95%) were used for the visual display of the MAM.
Results
Prediction methods
The four prediction methods yielded similar prevalence results throughout the forecasted period with the exception of the TM method, which provided more conservative estimates (Table 1).
Predicted prevalence rates between 2003 and 2030 through four forecasting methods.

CI, confidence interval; DM, drift method; ETSM, ETS method; MA, moving average method; PI, prediction interval; TM, theta method.
To evaluate the fitting of the forecasts, we performed accuracy tests. The DM presented the smallest error values regardless of which accuracy measure was used (Supplementary Table 1), and therefore may be considered the most accurate of those implemented and the most similar to the simple MAM.
Forecasted IBD prevalence in Portugal
In 2019, the calculated prevalence of IBD in Portugal is: MAM: 319 per 100,000 (95% CI: 286–351); DM: 326 per 100,000 (95% PI: 241–411); ETSM: 302 per 100,000 (95% PI: 254–350); and TM: 325 per 100,000 people (95% PI: 145–334). In 2030, the forecasted prevalence ranges from 325 per 100,000 (TM 95% PI: 194–456) to 491 per 100,000 people (DM: 95% PI: 332–650).
When comparing data from 2003 to the forecasted prevalence of 2030, we obtained prevalence estimates 4–6-fold higher (Table 1). In addition, the average annual percent change of the forecasted prevalence rate was approximately 4–6%, regardless of the methods implemented. This meaning that the prevalence of IBD is forecasted to climb 4–6% per year in Portugal (Table 1).
Figure 1 presents the annual forecasted prevalence of IBD for each method, with associated 80% and 95% PI or CI.
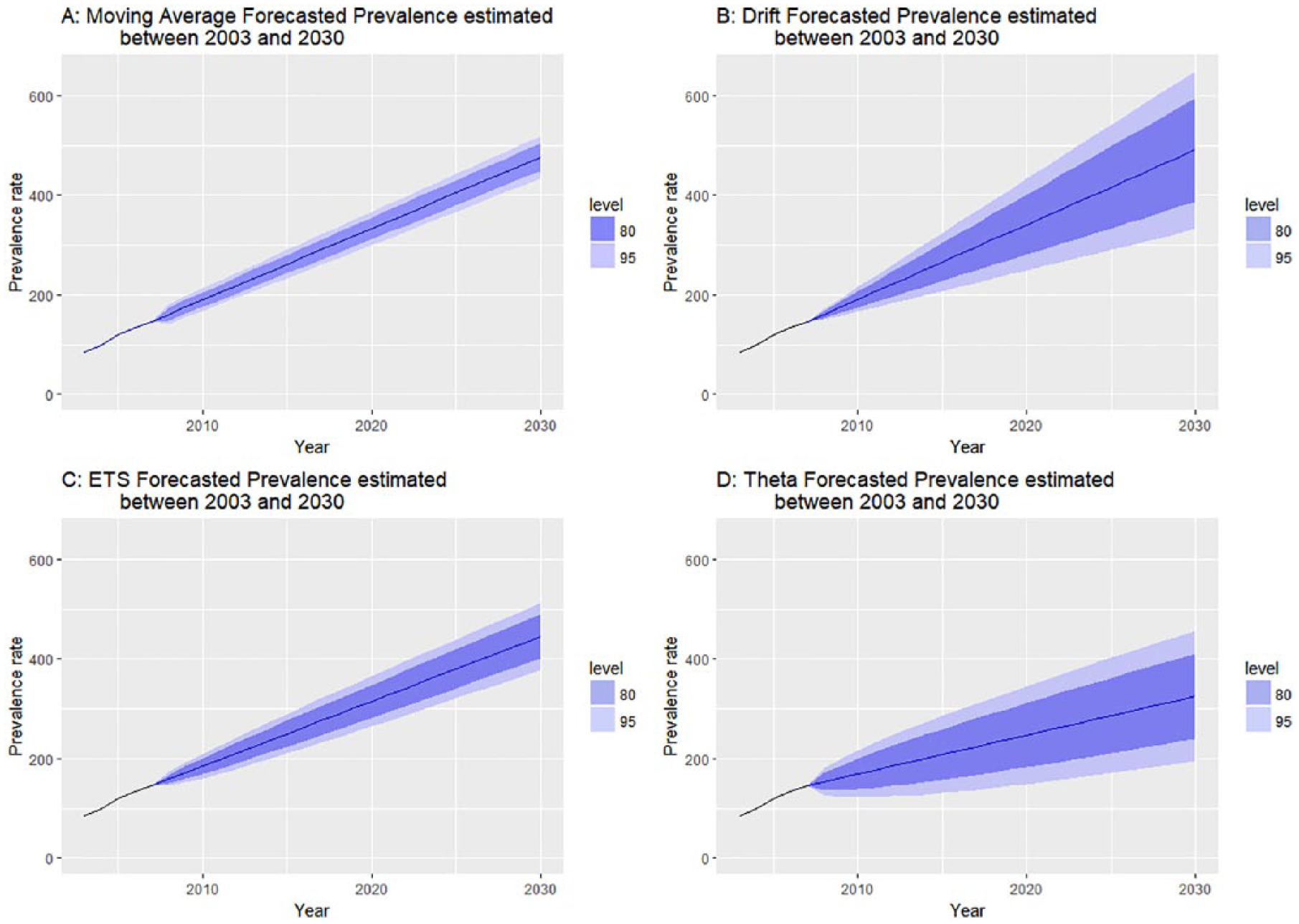
Forecasted prevalence rates of IBD between the years 2003 and 2030. Shaded areas are either confidence intervals (a) or prediction intervals (b, c, d).
Discussion
Our analysis, based on the application of four simple forecasting methods pertaining to previously published data, allowed the estimation of past, present and future prevalence of IBD in a southern European country.
In 2003, approximately 0.1% of the Portuguese population was diagnosed with IBD. According to our estimations, this figure is forecasted to rise to 0.22–0.33% in the past year of 2016, reaching 0.24–0.33% in 2019 and 0.32–0.49% in 2030. Consequently, Portugal may be considered part of the group of European countries with the highest IBD prevalence estimates. Since in Europe, the highest reported prevalence values correspondent to the period of 1990 to 2016, were 505 per 100,000 people for UC and 322 per 100,000 people for CD. 2
As previously mentioned, the prevalence of IBD is estimated to climb approximately 4–6% per year in Portugal. This is due to the imbalance between the incidence and mortality of IBD as a chronic and incurable disorder. 13
Moreover, these estimations are higher than what was predicted by Coward and colleagues 14 for Canada (2.86%), which may be explained by the different methodologies applied to each study. Whereas Coward and colleagues 14 study analyzed larger datasets presenting a more robust implementation of forecasting methods, our work has a more comparative nature due to the limited available data.
Since the increase in IBD prevalence appears to be inevitable, it is of major importance for health policies to be developed and healthcare systems adapted to the growing burden of IBD and the resulting economic impact.5,6,15
Additionally, more studies are needed in order to reach a better understanding of the actual prevalence of IBD in Portugal, since Azevedo and colleagues 8 used a pharmaco-epidemiological approach based of the use of intestinal anti-inflammatory drugs to reach the original prevalence estimates.
Regarding the forecasting analysis, our estimations were based on the prevalence estimates reported by Azevedo and colleagues 8 which comprise only a 5-year period. Although accuracy tests were performed, these results must be taken with caution as we must acknowledge the severe limitations of conducting forecast estimations on a small dataset. This was the rationale for the implementation of several simple forecasting methods, in order to allow comparisons among the results obtained.
The DM, which has shown better accuracy, estimates the slope of the original sample, draws a line and extrapolates it into the future. The MAM only considers a predetermined number of past data points, four in our case. These two methods yielded the most comparable results due to the similarity between the size of our sample and the number of data points considered for the calculation of MAM. As for the ETSM, it presents two smoothing parameters, alpha and beta with values ranging from 0 to 1. The first when close to 1 means estimates are based on recent observations while a small beta value, which represents the slope of the time series, implies a slightly unchanging trend. 16 This is representative of our forecasted scenario regarding the results by the ETSM. Hence, the smaller estimates and respective PIs (Table 1). As previously mentioned, the TM can be described as a special case of SES with drift that is equal to half the slope of a straight line fitted to the data. 9 Therefore, presenting the more conservative prevalence prediction (Table 1).
Additionally, we tested the aforementioned models on a dataset of the prevalence of CD from the study of Yao and colleagues. 17 This was a nationwide study which covered the period of 1986–1998. We compared the results of the forecasting methods to the work of Asakura and colleagues, to our knowledge the most recent nationwide prevalence study of IBD in Japan. Asakura and colleagues reported a CD prevalence of 21.2 per 100,000 persons in the year 2005. 18
As seen in Supplementary Figure 1, our CD prevalence forecasts for the year 2005 were similar to what was estimated by Asakura and colleagues. Moreover, according to the accuracy tests performed, the model showing the lowest error values was the ETSM which presents the closest estimation of that of Asakura and colleagues. 18
Overall, these results show the importance of performing future prevalence and forecasting studies and to act on the impending burden of IBD, given the escalation of IBD prevalence on such a likely high rate, as estimated here.
Supplemental Material
Supplementary_Figure_1 – Supplemental material for What forecasting the prevalence of inflammatory bowel disease may tell us about its evolution on a national scale
Supplemental material, Supplementary_Figure_1 for What forecasting the prevalence of inflammatory bowel disease may tell us about its evolution on a national scale by Mafalda Santiago, Fernando Magro, Luís Correia, Francisco Portela, Paula Ministro, Paula Lago and Cláudia Camila Dias in Therapeutic Advances in Gastroenterology
Supplemental Material
Supplementary_Table_1 – Supplemental material for What forecasting the prevalence of inflammatory bowel disease may tell us about its evolution on a national scale
Supplemental material, Supplementary_Table_1 for What forecasting the prevalence of inflammatory bowel disease may tell us about its evolution on a national scale by Mafalda Santiago, Fernando Magro, Luís Correia, Francisco Portela, Paula Ministro, Paula Lago and Cláudia Camila Dias in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
The authors would like to acknowledge Tiago Campos for scientific writing assistance. The authors thank the Center for Health Technology and Services Research (CINTESIS) for providing the conditions to perform this study (reference UID/IC/4255/2019), the support given by the Project ‘NORTE-01-0145-FEDER-000016’ (NanoSTIMA), financed by the North Portugal Regional Operational Programme (NORTE 2020), under the PORTUGAL 2020 Partnership Agreement, and through the European Regional Development Fund (ERDF). MS acknowledges ‘Fundação para a Ciência e Tecnologia (FCT)’, Portugal under grant number PD/BD/142890/2018.
In terms of author contributions, MS was involved in the design of the study, data analysis, interpretation of data and writing the manuscript. FM was involved in the conception and design of the study, interpretation of data and revising the manuscript. CCD was involved in the conception and design of the study, data analysis, interpretation of data and revising the manuscript. All other authors helped in the interpretation of data, reviewed and approved the final manuscript
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
Fernando Magro received a fee for presenting from: AbbVie, Ferring, Falk, Hospira, PharmaKern, MSD, Schering, Lab. Vitoria, Vifor, OmPharma. All other authors have nothing to declare.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.