
Abstract
Tofacitinib is an oral small molecule directed against the JAK/STAT pathway, blocking the inflammatory cascade. Oral formulation of tofacitinib has recently been approved for the treatment of patients with moderate–severe ulcerative colitis. Its efficacy and safety have been demonstrated in three phase III clinical trials and confirmed by promising real-life data. The purpose of this review is to summarize the available evidence on the efficacy and safety of tofacitinib and to define its role and position in the treatment algorithms for patients with ulcerative colitis.
Introduction
Ulcerative colitis (UC) is a chronic inflammatory disease of the colon with a relapsing–remitting pattern that can affect individuals of all ages.1,2 The precise aetiology of UC is unknown, and curative medical therapy is not yet available. The aim of current pharmacological treatment is to reduce the mucosal inflammation and maintain symptom remission, though these goals are not achieved in all patients. 3 The therapeutic options now available include 5-aminosalicylates, sulfasalazine, systemic or topical steroids, immunosuppressants (azathioprine, mercaptopurine and cyclosporine), as well as biological drugs such as antitumor necrosis factor (anti-TNF) agents (infliximab, adalimumab and golimumab) and antiadhesion molecules (vedolizumab). 4 Nevertheless, up to 30% of patients do not respond to biologics (primary nonresponders), and about 10–20% per year lose response after an initial improvement (secondary nonresponders), therefore requiring a dose escalation or being switched to another drug class.
In up to 15% of patients, total proctocolectomy is needed because of refractoriness to medical therapy, development of colonic high-grade dysplasia/cancer, or complications. 5 However, surgery requires a disabling intervention for patients and can carry both early (⩽30 days postoperatively) and late (>30 days postoperatively) complications. 6 For these reasons, expanding therapeutic opportunities with new treatments is greatly needed.
Janus kinases (JAKs) are a group of four intracellular tyrosine kinases mediating the signal transduction of multiple cytokines implicated in several functions including the activation of inflammation.7,8 Their pivotal role in sustaining chronic inflammation, by stimulating the activity of T and B cells, and the production of mucus and antibodies, makes them an interesting pathway to target for the development of new molecules. Several anti-JAK agents (selective or nonselective) have been developed. Tofacitinib is the first JAK inhibitor approved for UC, although it is already licensed in the US for rheumatoid arthritis 9 since 2012. Unlike other biologics, that are mainly selective on a single cytokine or integrin, tofacitinib acts on a multitude of cytokines at the same time by inhibiting the JAK/STAT pathway, resulting in a wider effect on the gastrointestinal inflammation. Tofacitinib blocks the JAK-1 and JAK-3, and, at high concentrations, tyrosine kinase 2 (TYK2) and JAK-2 pathways as well. Interestingly, tofacitinib is rapidly absorbed after oral intake with a time to peak concentration of ½ h, thus allowing a more comfortable route of administration for the patient and a quicker effect than the majority of other drugs used in inflammatory bowel disease. On the other hand, the short half-life of about 3 h requires twice-a-day intake which could reduce patient compliance. Finally, because it is not a monoclonal antibody, it is not antigenic.10,11
The purpose of this review is to summarize the available data on the efficacy and safety of tofacitinib, both in clinical trials and from real-world experiences.
Methods
We searched the PubMed database using the following keywords ‘JAK inhibitors’, ‘JAK/STAT’, ‘small molecules’, and ‘tofacitinib’ individually or in combination with ‘IBD’, ‘Inflammatory Bowel Disease’, ‘Ulcerative Colitis’, ‘UC’, or ‘OCTAVE’. Only articles in English were included regardless of their date of publication, abstracts reporting relevant data were considered as well.
Ethics approval and informed consent were not required for this review.
Results
Efficacy data
The first data on tofacitinib efficacy in UC came from a phase II, dose-defining, double-blind, randomized, placebo-controlled trial, in which 194 adults with moderate–severe disease were randomized to receive twice-daily placebo or different doses of tofacitinib (0.5 mg, 3 mg, 10 mg, or 15 mg) for 8 weeks. 12 The primary endpoint, defined as a ⩾3 points’ reduction in Mayo activity score, was reached by 61% (p = 0.10) and 78% (p < 0.001) of patients in the 10 mg and 15 mg groups, respectively, compared with 42% of placebo. Clinical remission (Mayo score ⩽ 2, with no subscore > 1) at 8 weeks occurred in 48% (p < 0.001) and 41% (p < 0.001) of the higher doses of tofacitinib as compared with 10% of patients receiving placebo. Finally, endoscopic response was higher among patients in the 10 mg and 15 mg dose groups compared with those receiving placebo or lower doses of tofacitinib.
More robust efficacy data were reported by three different phase III, randomized, double-blind, placebo-controlled trials; two assessing tofacitinib for induction therapy (OCTAVE Induction 1 and 2), and one for maintenance therapy (OCTAVE Sustain) in patients with moderate–severe disease activity. 13
In both OCTAVE Induction 1 and 2 trials, patients in the active treatment arm reached the primary endpoint, remission at 8 weeks, more frequently than in the placebo group, 18.2% versus 8.2% (p = 0.007) and 16.6% versus 3.6% (p < 0.001), respectively. Mucosal healing, a key secondary endpoint, was greater in the tofacitinib 10 mg arm compared with placebo for both OCTAVE Induction 1 and 2, 31.3% versus 15.6% and 28.4% versus 11.6% (p < 0.001 for both comparisons). Sixteen and six patients were originally randomized to receive high doses of tofacitinib (15 mg) in the OCTAVE 1 and 2 trials, respectively. Among these patients, clinical remission at 8 weeks was achieved in seven (43.8%) and three (50%), respectively. Further evaluation of such dose was interrupted by the drug manufacturer for reasons unrelated to either efficacy or safety, and patients were rerandomized 1:1:1 in the other groups. Despite the lack of a comprehensive assessment of such dosage, 15 mg tofacitinib could be an option worth investigating for induction therapy. No significant difference among patients previously treated with TNF-α inhibitors compared with naïve to biologics patients was found, both for primary and secondary outcomes.
Moreover, the effect of tofacitinib appears to be rapid. According to a recent subanalysis of data from OCTAVE Induction 1 and 2, improvements in Mayo stool frequency and rectal bleeding subscores were shown already at day 3, and were significantly greater for tofacitinib-treated patients than for placebo-treated ones: 9.2% versus 2.3% (p < 0.01) and 14.4% and 8.2% (p < 0.05), respectively. This effect was consistent among all subgroups. 14
The OCTAVE Sustained trial demonstrated higher remission rates at 52 weeks in the groups treated with 5 mg twice daily (n = 198) and 10 mg twice daily (n = 197) tofacitinib rather than placebo (n = 198), 34.3% and 40.6% (p < 0.001) versus 11.1% (p < 0.001), respectively. 11 Such results are summarized in Table 1.
Efficacy data on tofacitinib in patients with ulcerative colitis.

TFB, tofacitinib; PBO, placebo; b.i.d., twice daily; pts, patients.
The efficacy of tofacitinib is also clear on patient-reported outcomes. One study 15 investigated the perceived benefits of treatment of OCTAVE Induction and maintenance phase III clinical trials through a disease-specific questionnaire (IBDQ) and the general Short Form-36v2® Health Survey (SF-36v2). Results showed a statistically significant improvement in quality of life in the group treated with 10 mg tofacitinib in OCTAVE Induction 1 and 2 compared with placebo (40.7 and 44.6 versus 21.0 and 25.0, respectively, p < 0.0001). Mean changes from baseline to week 8 SF-36v2 Physical and Mental Component Summaries (PCS/MCS) were also significantly greater in the 10 mg twice daily (b.i.d.) tofacitinib arm compared with placebo. Similarly, in the OCTAVE Sustain population, changes at week 52 of IBDQ and SF-36v2 PCS/MCS were maintained in the active treatment arm 5 mg (+3.7 and 0.0, −1.0) and 10 mg (4.8 and 0.3, 0.1) b.i.d., unlike in the placebo group (−26.5, −5.2 and −6.7). Subanalyses of health-related quality of life showed a consistent benefit of tofacitinib therapy regardless of corticosteroid use at baseline, sex and previous anti-TNF treatment.
A post hoc efficacy analysis on Eastern Asian patients included in OCTAVE Induction 1 and 2 and OCTAVE Sustain trials showed greater efficacy of tofacitinib versus placebo in this subgroup when compared with the global population for both induction (18.9% versus 17.6%) and maintenance therapy (47.6% versus 40.6%). The safety profile did not vary significantly, instead. 16
Safety data
The incidence of tofacitinib-related adverse events (AEs) in UC treatment appears to be similar to that of patients treated with tofacitinib for rheumatoid arthritis. No particular safety concerns were raised from the UC trials and the overall safety profile can be considered in line with monoclonal antibodies. 17
In the phase II trial on 194 patients, the most commonly reported AEs were influenza (n = 6), nasopharyngitis (n = 6) and an increase in low-density lipoprotein (LDL), high-density lipoprotein (HDL), and total cholesterol levels proportional to the dose of tofacitinib administered, which subsided after treatment discontinuation. Serious AEs were only two (1%); one postoperative abscess and one anal abscess. 10
In the 8-week-long OCTAVE Induction 1 trial (n = 614), patients treated with 10 mg of tofacitinib reported a 56.5% rate of AEs compared with 59.8% in the placebo, and the proportion of patients suffering at least one serious AE was 3.4% and 4.1%, respectively. Similarly, the rate of AEs reported in the OCTAVE Induction 2 (n = 547) was 54.1% in the active treatment arm and 52.7% in the placebo arm; the rate of serious AEs 4.2% and 8.0%, respectively. In the OCTAVE Sustain trial (593 patients who previously responded to the induction phase and were treated for 52 weeks), 72.2% of those in the 5 mg group reported at least one AE, while there was 79.6% in the 10 mg group and 75.3% in the placebo one. Serious AEs were 5.1% for the low dose, 5.6% for the high dose and 6.6% for placebo. 11 Such findings are summarized in Table 2.
Safety data on tofacitinib in patients with ulcerative colitis.

AEs, adverse events; SAEs, severe adverse events; PBO, placebo; TFB, tofacitinib; b.i.d., twice daily; Pts, patients.
Nasopharyngitis, arthralgia, and headache were the most commonly reported AEs. They occurred more frequently among tofacitinib-treated patients than in placebo controls. Nasopharyngitis occurred in 7.1% and 4.9% of patients in the two induction trials and in 9.6% and 13.8% of patients treated with 5 and 10 mg tofacitinib in the maintenance trial, compared with 7.4%, 3.6% and 5.6% in the respective placebo groups. Arthralgia incidence rate was 2.9% and 2.6% in the OCTAVE 1 and 2 trials and 8.6% and 8.7% in the Sustain trial compared with 4.9%, 5.4% and 9.6% in the corresponding placebo groups. Finally, headache was observed in 7.8% and 7.7% of patients in the induction trials and in 8.6% and 3.1% in the Sustain trial versus 6.6%, 8.0% and 6.1% of patients in the respective placebo groups. In the induction trials, serious AEs occurred in 3.4% and 4.2% of patients in the 10 mg tofacitinib group and in 4.1% and 8.0% in the placebo group. In the OCTAVE Sustain trial, serious AEs resulted in 5.1% of the patients in the 5 mg tofacitinib group, 5.6% in the 10 mg tofacitinib group, and 6.6% in the placebo group. Serious AEs were mainly nonopportunistic serious infections, defined as infections requiring hospitalization or e.v. antibiotic treatment.
A post hoc analysis pooling all patients (n = 1157) receiving any dose of tofacitinib both for induction or maintenance, showed that 33 (2.9%) subjects suffered at least one serious infection compared with two (1.0%) of the placebo controls (n = 198). Such events included pneumonia, herpes zoster (HZ), anal abscess, and Clostridium difficile infection.
HZ infection deserves a special mention, as it was previously reported among the most common serious infections in rheumatoid arthritis patients treated with tofacitinib.18,19 Winthrop and colleagues 20 reported that 5.6% (n = 65) of patients treated with any dose of tofacitinib in all the OCTAVE trials developed a HZ infection. Of these, 11 (16.9%) had a multidermatomal involvement (2 nonadjacent or 3–6 adjacent dermatomes), and 1 (1.5%) developed encephalitis (that resolved with standard treatment). Overall, five (7.7%) events led to treatment discontinuation. The incidence rate of HZ infection over a mean of 509.1 days (range 1–1606) was 4.07 [confidence interval (CI) 3.14–5.19]. Previous studies in rheumatoid arthritis, showed that HZ incidence rates were higher among older individuals, Asians, those who had previously failed anti-TNF treatments, those using 10 mg b.i.d. doses of tofacitinib, and those with corticosteroid use at baseline.21–23 Winthrop’s analysis of UC patients treated with tofacitinib confirmed that age [for each 10 years, hazard ratio (HR) 1.58; 95% CI 1.34–1.87; p < 0.0001], prior TNF-inhibitor failure (HR 1.92; 95% CI 1.15–3.21; p = 0.0122) and Asian ethnicity correlated with an increased risk of HZ infection, although the latter did not reach significance (HR 1.76; 95% CI 0.97–3.19; p = 0.0612). 20 Older age is known to be associated with a decrease in immunity and thus with a greater risk of infections, including HZ, also among otherwise healthy individuals. It remains unclear why Asians could have a higher risk of HZ infection; part of that difference could be explained by two single-nucleotide polymorphisms, present within a minority of Japanese and Korean populations, that confer an increased risk. Similarly, no clear explanation is available on why previous anti-TNF failure is linked to increased HZ infections.
Vaccination against varicella zoster virus (VZV) remains the most suitable preventive measure for these patients, but since it is a live vaccine, it should be started 3–4 weeks before commencing tofacitinib. Recently, a new inactivated recombinant vaccine (Shingrix®, GlaxoSmithKline) which is not contraindicated in immunocompromised patients has been approved by the US Food and Drug Administration (FDA) in 2017 24 and could prevent VZV infection or reactivation during the treatment.
However, the risk of serious or opportunistic infections seems to be similar to the other molecules approved for moderate–severe UC, as shown by a recent systematic review and meta-analysis comparing all biologics approved for UC and tofacitinib. 25
Two cases of gastrointestinal perforation were reported in the OCTAVE trials; one in the 10 mg group of OCTAVE Induction 1 and the second in the placebo arm of the same study. There have been reports of such events in patients treated with tofacitinib for rheumatoid arthritis and psoriasis, though a clear correlation to the drug has not been proven.26–28
Across all three OCTAVE trials and the open-label long-extension study (total n = 1157), tofacitinib-treated patients were diagnosed with 11 nonmelanoma skin cancers; however, all had previously received azathioprine and 8 had received anti-TNF. Another 11 malignancies were diagnosed in actively treated groups with no particular pattern; one case of each of the following was reported: cervical cancer, hepatic angiosarcoma, cholangiocarcinoma, cutaneous leiomyosarcoma, Epstein–Barr-virus-associated lymphoma, renal cell carcinoma, essential thrombocythemia, acute myeloid leukemia, adenocarcinoma of colon, lung cancer, and breast cancer.
The increase of serum lipid levels is a known side effect of tofacitinib. 12 This effect was also confirmed in the phase III trials among tofacitinib-treated patients, but it was apparently not accompanied by an increase in major adverse cardiovascular events. Only four patients who received tofacitinib in the phase II A3921063 [ClinicalTrials.gov identifier: NCT00787202], OCTAVE Induction 1 and 2, or OCTAVE Sustain trials had cardiovascular events apparently unrelated to drug administration.
Tofacitinib can cross the placental barrier. Preclinical studies in rats and rabbits showed that the drug exposure can cause fetal malformations (cardiovascular and bone malformations) when given at much higher doses (100 mg/kg/day) than the therapeutic doses in humans. 29 Data on pregnant women derived from a rheumatologic cohort of 9815 patients showed that 47 pregnancies resulted in 25 healthy newborns, 7 spontaneous abortions, 8 medical terminations, 1 congenital malformation (pulmonary valve stenosis), and 6 cases pending or lost to follow up. According to these data, tofacitinib does not appear to increase the risk of fetal malformation or death. 30 New data from the 1157 patients actively treated in the phase II and III trials in UC reported 11 cases of maternal exposure to tofacitinib resulted in 4 healthy newborns, 2 medical terminations, 2 spontaneous abortions and 3 pending or lost to follow up. 31 Nevertheless, these studies are retrospective and the number of pregnancies reported is relatively small. Currently, tofacitinib is not approved for the treatment of pregnant or breastfeeding women. Routine pharmacovigilance and other studies are needed to evaluate the safety in this particular setting.
Real-life experience
Recent data from a small real-world study including 58 patients (53 UC, 4 Crohn’s disease, and 1 pouchitis) who completed 8 weeks of treatment with tofacitinib were consistent with OCTAVE’s preliminary results. 32 A total of 21 participants (36%) had a clinical response and 19 (33%) achieved clinical remission, of which 14 (24%) were also steroid free. A total of 26 patients completed 52 weeks of follow up, 5 of which (19%) were clinically responsive to the drug, and 7 (27%) were in clinical steroid-free remission at that time. Interestingly, patients’ demographic characteristics, disease extent, previous medical therapy, and steroid exposure were not predictive of clinical response during both induction or maintenance treatment.
Infections were reported in 12 patients (20.1%) treated with tofacitinib, though 6 were concomitantly on corticosteroids, 1 was on vedolizumab and 1 was on tacrolimus. The reported AEs were C. difficile colitis (four cases), upper respiratory tract infections (one), H. Zoster infection (one), aspergillus sinusitis (one), Epstein–Barr-virus infection (one), parainfluenza (one), cellulitis (one), Escherichia coli gastroenteritis (one) and group B streptococcus sepsis (one). Treatment was halted in nine patients, and subsequently resumed in four. Three patients had a modest increase in LDL levels, but no major cardiovascular events were reported. No patient required dyslipidemia treatment or tofacitinib discontinuation.
Discussion
Tofacitinib represents a significant advance in the management of patients with UC. The blockade of the JAK/STAT cascade implicates an efficient blockade of the chronic inflammatory cascade at different levels, with marginal side effects. An oral formulation should be more acceptable to patients, eliminating discomfort and possible AEs related to infusion therapies or subcutaneous injections. The very short half-life and high intestinal bioavailability allows the fast, effective action of tofacitinib. This is also an advantage in case of need to withdraw the drug for AEs or before interventions with high risk of infection (such as major surgery or live vaccination), since the drug is rapidly cleared from the body. Moreover, since it is a small molecule and not an antibody, it does not generate antidrug antibody. One main limitation, as previously shown with oral drugs such as 5-ASA compounds, can be a reduced compliance, especially in the long term. 33
Several clinical trials showed the efficacy of the drug in determining clinical remission of patients with moderate–severe UC, both in the induction and in the maintenance phase. The efficacy of tofacitinib was also confirmed by the high rate of mucosal healing and by the significant improvement in quality of life, as demonstrated by the reduction in the IBDQ score.
The drug had a good safety profile and the main AEs are comparable with those observed for other drugs used in the same patient setting (moderate–severe UC patients refractory to conventional therapies). The increase in LDL and HDL cholesterol levels, already reported in trials performed on rheumatologic diseases, was confirmed but not related to a greater incidence of cardiovascular events. A considerable risk for developing HZV infections was highlighted among the expected AEs of relevance, but the incidence was very low and did not usually result in permanent treatment discontinuation. Furthermore, such risk of HZV infections could be prevented by the HZV vaccination. There is no clear increase in risk of malignancies, although data on US patients are scarce and most of the evidence comes from studies in rheumatoid arthritis, which itself could be a confounder in the development of some cancers.
Tofacitinib has recently been approved for the treatment of moderate–severe UC by the FDA 29 and the European Medicines Agency. 34 To date, however, no head-to-head clinical trials have been conducted to clearly recommend the right positioning of this drug in the therapeutic algorithm for treatment of patients with UC.
A recent systematic review and network meta-analysis evaluated 19 randomized placebo-controlled trials to compare the efficacy and the safety of tofacitinib, anti-TNF (infliximab, adalimumab, golimumab) and anti-integrin (vedolizumab) as induction or maintenance therapy for patients with moderate–severe UC naïve to anti-TNF; all drugs were superior to placebo in determining clinical response, clinical remission and mucosal healing, both in the induction and in the maintenance phase. Indirect evidence suggested that tofacitinib performance is similar to biologic therapies. 17 Tofacitinib was equally safe to other drugs and demonstrated a stronger safety profile than infliximab.
Another systematic review and network meta-analysis (analyzing 14 phase II and III studies), comparing available first-line treatments in patients with moderate–severe UC showed that tofacitinib resulted in the highest rate of clinical remission in the maintenance phase, with a similar profile to vedolizumab. 22
The pharmacokinetics and pharmacodynamics of tofacitinib need a special mention. Since it is meta-bolized by cytochrome CYP3A4, interactions with other medications that inhibit or induce CYP3A4 are likely. Tofacitinib exposure is increased when co-administered with potent inhibitors of CYP3A4 (e.g. ketoconazole) or when administration of one or more concomitant medicinal products results in both moderate inhibition of CYP3A4 and potent inhibition of CYP2C19 (e.g. fluconazole). Like most other drugs, tofacitinib requires adjustment, in case of renal and hepatic impairment, and in the event of neutropenia, lymphocytopenia or anemia. Specific drug adjustments provided by the manufacturer are summarized in Table 3 and Table 4. 35
Tofacitinib dose adjustments in special conditions.

Hb, Hemoglobin; Cr., creatinine.
Tofacitinib dose adjustments in case of drug co-administration.
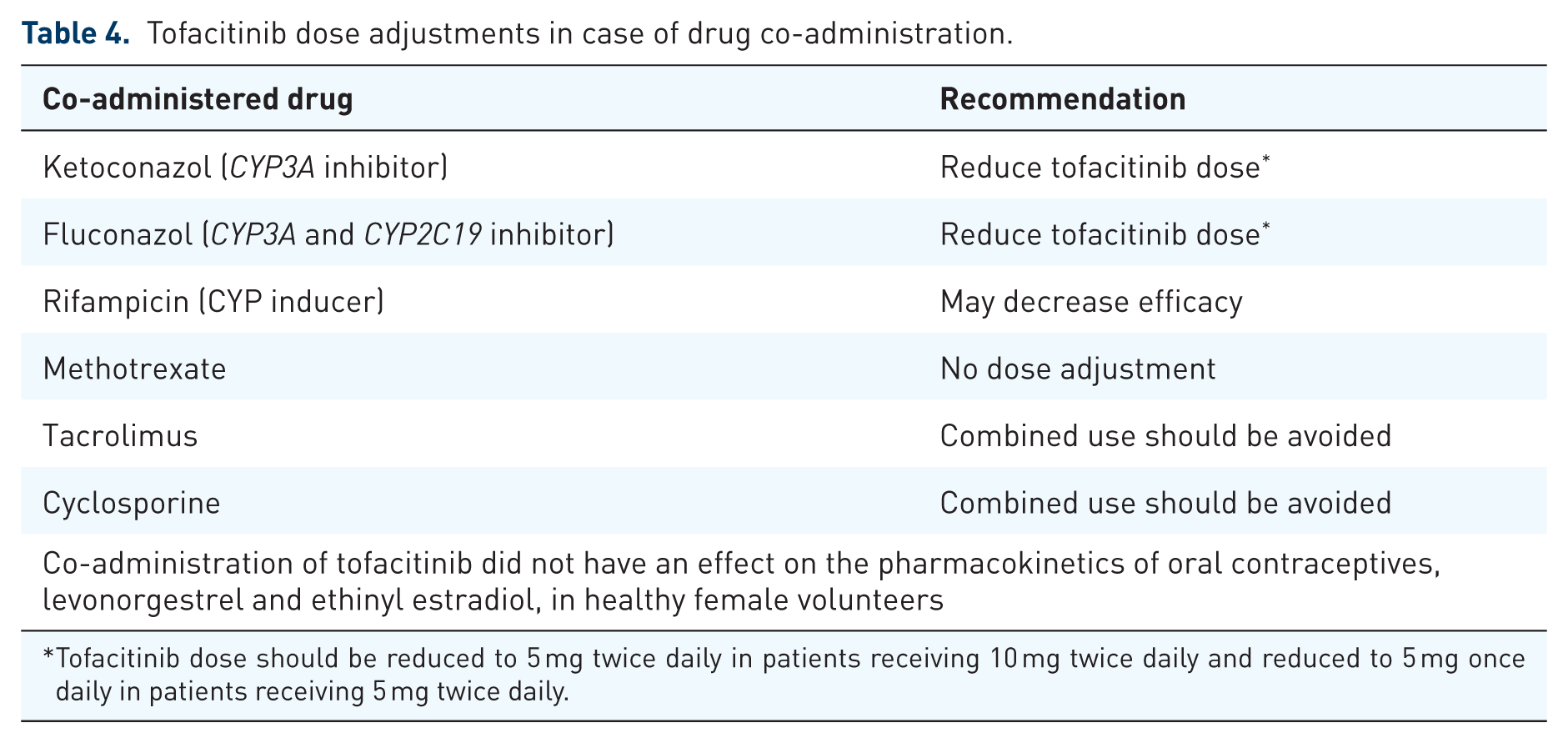
Tofacitinib dose should be reduced to 5 mg twice daily in patients receiving 10 mg twice daily and reduced to 5 mg once daily in patients receiving 5 mg twice daily.
Data from clinical studies suggest that tofacitinib could be a valid first-line treatment in patients with moderate–severe UC not responsive to steroids and mesalazine, or as second-line therapy in patients previously treated with an anti-TNF or an anti-integrin. Theoretically, no additional contraindications should be considered for tofacitinib, as compared with the other approved medications. Some caution and adjustment should be adopted in patients with concomitant therapies.
Tofacitinib could also be economically viable in comparison with other biologics due to its lower production cost. Such estimates much depend on individual countries and are perhaps premature given its only recent approval. 36
Conclusion
In conclusion, the introduction of tofacitinib for the treatment of UC adds a new therapeutic strategy and increases the possibility of curing UC patients. In the absence of head-to-head clinical trials demonstrating a clear superiority of one drug versus others, treatment choice should depend on patients’ preferences and characteristics, cost, and local regulations. The benefits of tofacitinib over other therapies, however, should be considered in the positioning of tofacitinib in the treatment algorithms.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
Gionata Fiorino served as a consultant and a member of Advisory Boards for MSD, Takeda Pharmaceuticals, AbbVie, Pfizer, Celltrion, Amgen, Sandoz, Samsung, and Janssen Pharmaceuticals. Laurent Peyrin-Biroulet received consulting fees from Merck, Abbvie, Janssen, Genentech, Mitsubishi, Ferring, Norgine, Tillots, Vifor, Pharmacosmos, BMS, UCB-pharma, Hospira, Celltrion, Takeda, Biogaran, Boerhinger-Ingelheim, Lilly, Pfizer, HAC-Pharma, Index Pharmaceuticals, Amgen, Sandoz, Forward Pharma GmbH, Celgene, Biogen, Lycera, Samsung Bioepis, and lecture fees from Merck, Abbvie, Takeda, Janssen, Ferring, Norgine, Tillots, Vifor, Mitsubishi, and HAC-pharma. Silvio Danese has served as a speaker, a consultant and an advisory board member for Abbvie, Ferring, Hospira, Johnson & Johnson, Merck, Millennium Takeda, Mundipharma, Pfizer, Tigenix, UCB Pharma, and Vifor. The other authors declare no conflicts of interest.