
Abstract
Background:
Instrumented anorectal biofeedback (BF) improves symptoms and quality of life in patients with faecal incontinence and defecation disorder-associated chronic constipation. However, demand for BF greatly outweighs availability, so refinement of the BF protocol, in terms of the time and resources required, is of importance. Our aim was to evaluate the outcomes of an abbreviated BF protocol in patients with defecation disorder-associated chronic constipation and/or faecal incontinence compared to standard BF.
Methods:
Data were collected from consecutive patients (n = 31; age 54 ± 15; 29 females; 61% functional constipation) undergoing an intentionally abbreviated BF protocol, and compared in a 1:2 ratio with 62 age, gender and functional anorectal disorder-matched control patients undergoing a standard BF. Outcomes included change in symptoms, physiology, patient satisfaction and quality of life.
Results:
On intention to treat, patients in both protocols showed significant improvement in symptom scores and the magnitude did not differ between groups. Impact on quality of life, satisfaction and control over bowel movements improved in both protocols, but satisfaction improved to a greater extent in the standard BF protocol (p = 0.009). Physiological parameters were unchanged after BF apart from improvement in rectal sensation in the standard BF group compared to abbreviated BF (p ⩽ 0.002).
Conclusions:
Abbreviated anorectal BF offered to patients travelling from far away was not different to a standard BF in providing substantial, at least short term, improvements in symptoms of constipation and faecal incontinence, quality of life and feeling of control over bowel movements. Refinement of the standard BF protocol according to individual patient phenotypes and desired outcomes warrants further study in order to maximize efficacy and improve access for patients.
Introduction
Constipation and faecal incontinence (FI) are disorders with a high prevalence in the general community and are associated with a significantly impaired quality of life.1,2 In turn, these conditions also contribute significantly to health care utilization, direct and indirect economic costs to society and time off work. 3 Conservative management options for these patients are sometimes suboptimal, and many patients continue to be troubled by symptoms. Instrumented anorectal biofeedback (BF) is an important component of the management algorithm and improves symptoms and quality of life in both patients with faecal incontinence and patients with defecation disorder-associated constipation.4,5 Other options for management, such as surgery or sacral nerve stimulation for FI, are much more expensive, invasive and have significantly higher complication rates.
Anorectal BF has been recommended by several consensus groups6,7 as the first-line therapy for patients with defecation disorder-associated constipation or FI who have failed conservative measures. Response rates are in the order of 80% for constipation 8 and 70% for FI. 9 Importantly, it is the instrumentation, and the concomitant process of educating patients about their anorectal physiology in relation to normal anorectal physiology that has been shown to contribute to the efficacy of BF protocols, rather than protocols utilizing Kegel exercises and education alone. 8 The comprehensive protocol proposed by the American Neurogastroenterology and Motility Society and European Society of Neurogastroenterology and Motility (ANMS-ESNM) 7 involves 6-weekly hour-long instrumented sessions for FI and 4–6 sessions for constipation.
Despite expert consensus recommendations and good response rates for BF, many patients with constipation or FI are not offered BF due to lack of access to the service. The reasons for this are complex and varied around the world, but a universal issue is that BF is usually performed in selected and specialized major centres, and those centres are limited in the number of patients they can treat at any one time due to the time-consuming nature of the therapy. In addition, some patients are limited in their ability to travel significant distances for repeated sessions.
Thus the logical next step is to develop an abbreviated ANMS-ESNM BF protocol and to determine whether a reduced number of instrumented sessions can maintain efficacy. In this study, we report the outcomes of such an abbreviated ANMS-ESNM style protocol, utilizing three patient visits (all with instrumented BF), for treating patients with functional constipation and/or FI, and compare these outcomes to those of a standard ANMS-ESNM protocol.
Materials and methods
Patient selection
A matched-cohort study was performed in a neurogastroenterology unit in a major tertiary referral centre. Data were collected prospectively in consecutive patients undergoing an intentionally abbreviated BF protocol. The abbreviated protocol was offered to patients attending from interstate, or from country areas where excess travel time or costs prohibited them from participating in the standard protocol. This abbreviated protocol involved fewer patient visits and instrumented sessions, but featured supplementary telephone calls. Patients were compared in a 1:2 ratio with age, gender and functional anorectal disorder-matched control patients undergoing standard BF protocol within the same time frame. This study was approved by the Royal North Shore Hospital Human Research Ethics Committee (LNR/14/HAWKE/372) and the committee did not require or suggest further consent over and above the informed consent already in place for our anorectal manometry and BF treatment.
Clinical assessment
On initial evaluation, all patients completed the Rome Integrative Questionnaire 10 and the Hospital Anxiety and Depression (HAD) scale. 11 Medication use, past surgery, concurrent medical conditions and bowel pattern were recorded using a structured questionnaire. Patients completed a 7-day stool diary and a modified SF-36 quality of life questionnaire, 12 and underwent assessment by a physician. Stool diaries were maintained throughout the BF programme. A further assessment by a physician was performed at the end of treatment, documenting major, moderate or minor improvement; no improvement; or worsening of bowel dysfunction.
For FI, the Faecal Incontinence Severity Index (FISI) 13 was calculated before and after BF treatment, and for patients with constipation the Knowles Constipation Questionnaire 14 was calculated before and after BF treatment. A 10 cm visual analogue scale (VAS) was also used before and after treatment for (1) impact of bowel dysfunction on quality of life (score anchors: 0 = no impact; 10 = most impact); (2) satisfaction with bowel movement (score anchors: 0 = very dissatisfied; 10 = very satisfied); and (3) feeling of control over bowel function (score anchors: 0 = no control; 10 = complete control). The main outcome measure for FI was change in FISI, while the main outcome measure for constipation was change in the constipation score. Secondary outcome measures for both constipation and FI included change in the patient-rated VAS for bowel satisfaction; control over bowel function; and effect of bowel function on quality of life, as well as the physician-assessed change in bowel dysfunction.
Anorectal physiology testing
After clinical assessment, all patients underwent comprehensive anorectal function studies, as previously described in detail. 15 Complete physical examination including rectal examination was performed in all patients. Anorectal manometry (ARM) was performed using a 7-lumen water-perfused manometry catheter with 0.5 cm spaced side holes and a compliant balloon (Dentsleeve International, Ontario, Canada). The catheter was connected to calibrated pressure transducers and data from the pressure transducers were displayed in digital form (Neomedix, Sydney, Australia). Each study assessed the following parameters: (1) resting anal sphincter pressure; (2) maximum anal sphincter squeeze pressure and duration of maximum anal squeeze pressure (sustained squeeze); (3) rectal pressure on strain and concomitant anal relaxation or paradoxical contraction; (4) anal pressure on cough; (5) rectal sensory thresholds for first sensation, urge and maximum tolerated volumes; and (6) balloon expulsion recorded as time taken to expel from the rectum, a party balloon tied at the end of a section of intravenous tubing and inflated with 50 ml of warm water, while seated on a private toilet.
Anorectal biofeedback treatment
Patients were referred to BF after failing conservative treatment including diet, bulking therapy, laxatives and anti-diarrheal agents where appropriate. The standard BF protocol consisted of six 30–60 min weekly sessions, four instrumented, with a gastroenterologist-supervised nurse specialist. For the abbreviated BF protocol training there were three visits for instrumented BF lasting 60 min each and two scheduled supplementary phone calls (see Figure 1). Total face-to-face time in the abbreviated BF was 180 min compared to 315 min in the standard BF protocol.
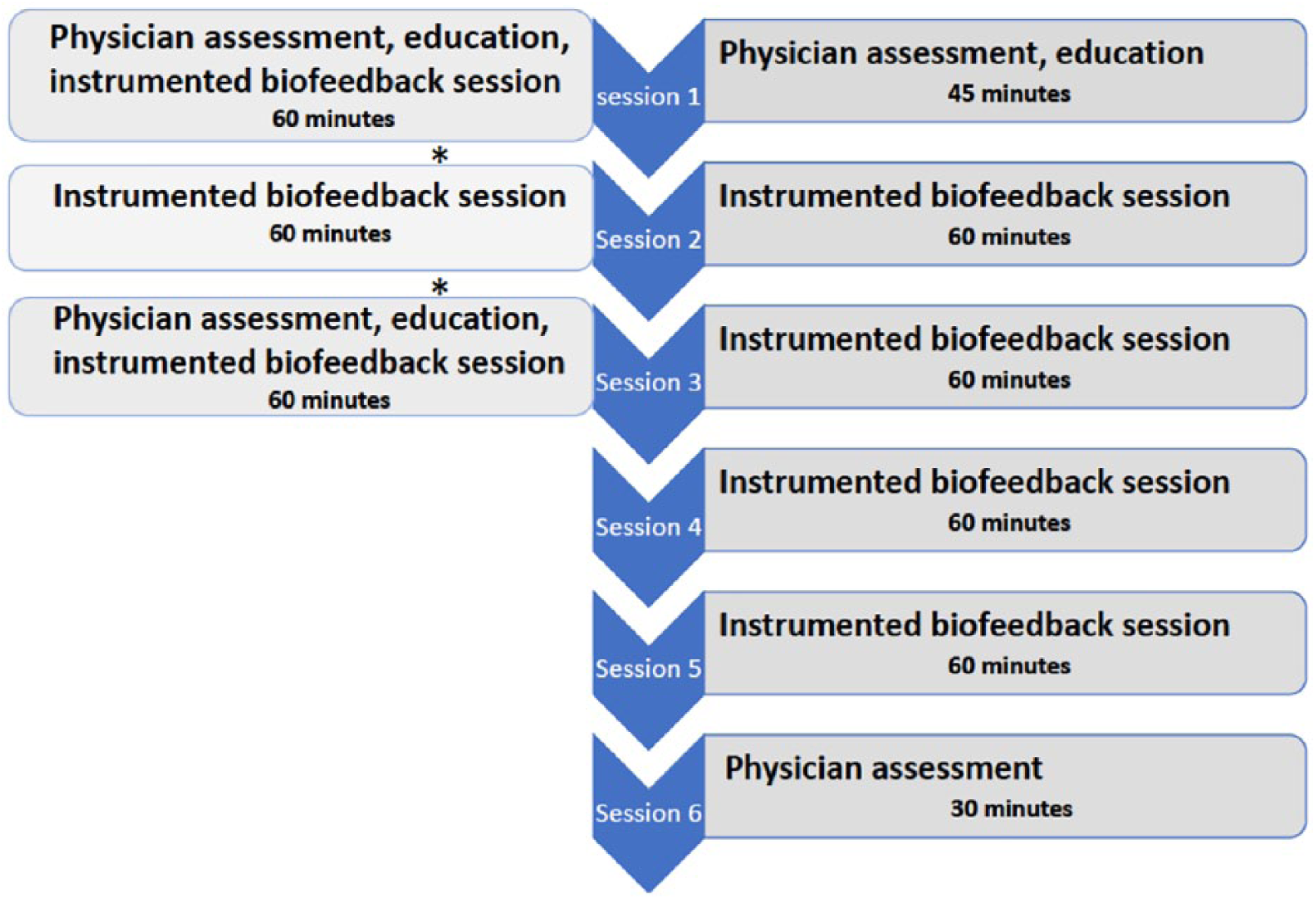
Diagram showing the differences between the standard biofeedback protocol and the abbreviated protocol.
In both instances the protocol consisted of (1) education regarding the anatomy of normal defecation; (2) advice on correct toilet positioning; (3) diaphragmatic breathing with manometric feedback aiming to achieve normalization of rectal pressure on strain, and use of diaphragmatic breathing for urge resistance training; 7 (4) manometric and surface electromyography (EMG) (Neomedix, Sydney, Australia) based BF for quick, sustained and half-maximum anal squeezes aimed to improve amplitude and duration of anal squeeze pressure; (5) manometric-based BF aiming to improve rectoanal coordination with synchronous rise in rectal pressure with anal sphincter relaxation; (6) rectal sensory training; and (7) balloon expulsion training where appropriate.
Statistical analysis
Quantitative measures are reported as mean and standard deviation (SD), while qualitative measures are reported as percentage and count. Patients who underwent the abbreviated treatment protocol were matched 1:2 with patients who underwent the standard protocol on age, gender and type of functional anorectal disorder. Within-group changes in quantitative parameters were evaluated using the Wilcoxon signed-rank test due to the non-normal distribution of some outcomes. For comparison of the BF treatment protocols, due to matching, contrasts between standard and abbreviated protocols were based on linear regression which employed the linearization method 16 to estimate within-pair correlation and adjust standard errors accordingly. Due to the non-normal distribution of some outcome variables, formal statistical inference employed the non-parametric bootstrap.
The available sample provided statistical power of 0.8 and calculated that for the standardized effect size Cohen’s d of 0.55, a total of 31 pairs matched 1:1 would be required based on the power function for the paired t test to provide statistical power of 0.8 at the 0.05 level of statistical significance (two-tailed). Given the 1:2 matching used in this study, statistical power therefore exceeds 0.8 and is adequate for clinically useful purposes. Statistical analyses were performed using Stata Statistical Software (Release 14; StataCorp LP, College Station, TX). A two-sided p value of less than 0.05 was considered to be statistically significant.
Results
Patients
A total of 31 consecutive patients (61% functional constipation, mean age 53 ± 15 years, 29 female) who prospectively underwent the intentionally abbreviated BF protocol were included. These patients were compared with 62 age, gender and functional anorectal disorder-matched patients who underwent the standard BF protocol over the same time period.
Baseline characteristics
The percentage of each group undergoing treatment predominantly for constipation rather than FI was 61% in the abbreviated group and 60% in the standard BF group. The two groups were well matched for demographics and baseline characteristics, as shown in Table 1. VAS for effect of bowel dysfunction on quality of life was higher (p = 0.02) and the SF36 sub-score for physical role was lower (p = 0.04) in the abbreviated BF group, both indicating worse severity. Baseline physiology is shown in Table 2 and was not different between the groups, other than thresholds for first and urge sensations being higher in the standard BF protocol, although both means were within our unit’s normal range. 17
Baseline demographics, clinical and psychological features of patients undergoing abbreviated versus standard biofeedback (BF) protocol.

Using standard BF as reference; **n = 39; ***n = 60; ****Using visual analogue scale (0–10).
HAD, Hospital Anxiety and Depression scale.
Baseline physiology of patients with constipation and faecal incontinence undergoing the abbreviated versus standard biofeedback (BF) protocol.

Using standard BF as reference.
In the subgroup of patients with constipation, VAS for impact of bowel dysfunction on quality of life was again higher and first-sensation thresholds were lower in patients in the abbreviated BF programme compared to standard BF (Supplementary Tables 1a and 2a). The subgroups with FI showed more marked differences, with patients in the abbreviated BF programme having higher FISI scores, reporting less satisfaction with and less control over bowel movements and scoring lower on the physical function and physical role components of the SF-36 (Supplementary Table 1b). Nevertheless, the only difference in pre-BF physiology was in sensation thresholds, being again lower in the abbreviated BF group of FI patients compared to standard BF (Supplementary Table 2b).
All constipated patients in both groups had abnormal defecatory symptoms (straining, incomplete emptying, sensation of blockage or digitation). On physiology testing, 67% and 56% of constipated patients in the abbreviated and standard anorectal BF groups, respectively, had inadequate rectal pressure on strain (defined as below 45 mmHg), 83% and 94% respectively were unable to relax their anal sphincter on strain, and 44% and 42% respectively were unable to expel the rectal balloon (in under 60 s) (Supplementary Table 2a). Defecatory dynamics did not differ between patients in the two protocols.
Abbreviated versus standard biofeedback protocols
The completion rate of abbreviated BF was 28/31 (90%) compared to 61/62 (98%) in the standard BF group (p = NS for difference). The actual number of visits in the abbreviated BF protocol was 3.5 ± 0.6 compared to 5.8 ± 0.4 in the standard BF protocol (2.3 fewer visits, 95% CI −2.6 to −2.1, p < 0.0001). No telephone calls were made in the standard BF protocol, while 1.4 ± 0.7 calls were made in the abbreviated BF protocol.
As shown in Table 3, there were minimal differences in the change in anorectal physiology between groups following BF, although first and urge sensation thresholds improved more in the standard BF group compared to the abbreviated BF group (p < 0.002), and duration of squeeze improved marginally more in the abbreviated group (p = 0.02). On intention to treat, patients in both protocols showed significant improvement in symptom scores and the magnitude did not differ between groups (Table 4). Impact of bowel dysfunction on quality of life, satisfaction with bowel motions and control over bowel movements improved in both protocols. Patient satisfaction, however, improved to a greater extent in the standard BF protocol and physician assessment classified more patients as moderate or great improvement in the standard BF protocol compared to the abbreviated BF protocol. Data for subgroups of constipated (Supplementary Tables 3a and 4a) and FI patients (Supplementary Tables 3b and 4b) were in general consistent with those of the whole cohort, although these should be interpreted with caution due to a smaller sample size. Costs for catheters and nursing time per patient were $AUD463.18 for the standard protocol and $AUD264.30 for the abbreviated protocol.
Changes in anorectal physiology of patients undergoing abbreviated biofeedback (BF) compared to patients undergoing standard BF protocol.

Change in outcome measures at the end of biofeedback (BF) compared to before BF: abbreviated BF versus standard BF protocol.

Using visual analogue scale (0–10).
Discussion
Constipation and FI are common problems in the community, associated with significant morbidity, economic and social costs and impairment in quality of life. 2 Specialized instrumented anorectal BF is a well-established and successful treatment for these conditions, yet has limited availability due to the considerable expertise and costly equipment required, and the time-consuming nature of current protocols. 7 We have shown that an abbreviated course of BF was not different in most major endpoints when compared to a standard BF protocol. Thus, an abbreviated protocol could be invaluable in improving access to this effective therapy, especially for patients living outside one of the few major centres around the world offering instrumented anorectal BF.
Small advantages were seen, however, in improvement in patient satisfaction with bowel movements and the physician-assessed response with the standard BF course when compared to the abbreviated BF course. These two outcomes are more global measures of overall improvement. It is possible that a shorter protocol might be sufficient to improve specific symptoms of FI or constipation (as evident by similar improvement of symptom scores); however, a longer protocol may be required to improve other gastrointestinal accompanying symptoms, the patient’s overall well-being or their coping strategies. Alternatively, increased face-to-face interactions with nurse therapists in the standard protocol may afford greater communication and psychological support, thus contributing to satisfaction. Another conclusion is that patients who suffer predominantly from poor satisfaction with bowel movements may be more suited to having a greater number of BF sessions or, put another way, any reduction in sessions beyond three or four is likely to lead to significantly reduced efficacy. As suggested by others, this work also highlights the importance of patients’ satisfaction and global measures like physician assessment as endpoints in functional bowel disease research. 18
Previous studies have shown a relative lack of improvement in physiology during anorectal BF compared to general outcome measures, especially for FI. 19 Although we did not show many changes in physiology, there was a notably greater improvement in rectal sensation in the standard BF protocol compared to the abbreviated protocol. In the future, in patients with FI or constipation undergoing anorectal BF, if hyposensitivity is thought to be a significant pathophysiological factor, then it may be preferable to perform more sessions if customizing a BF course for an individual patient.
There is a substantial cost saving in performing an abbreviated BF course. In addition to savings in consumable equipment used and therapists’ time, there are savings in indirect costs such as facility costs, maintenance and cleaning, administration, travel costs and time off work for patients. At present, most insurance companies in the United States do not fund BF, and yet if costs were lower and if the considerable long-term advantages of this one-off behavioural therapy course were considered, 20 then clearly BF would appear more favourable than alternate therapies for obstructed defecation and FI, most of which are surgical. In regions like the United Kingdom, where percutaneous tibial nerve stimulation (PTNS) is often the first-line treatment for FI, an abbreviated BF programme could become practical to combine with PTNS in the common subgroup of patients with coexistent FI and dyssynergia to optimize patient outcomes. 21
Limitations of our study include a relatively small sample size, which limited our ability to perform subgroup analysis such as comparing outcomes between FI and constipation. Also, the patients selected for the abbreviated protocol were in general patients who lived a long distance away. This may explain the baseline differences we saw, such as the abbreviated group having more severe symptoms and quality of life measures, as these patients were more avidly seeking care for their problem. On the other hand, this is a strength, as it can be seen that despite those baseline differences, the response rate in major outcome measures were similar. From a practical perspective, it is the patients travelling from some distance who have a particular need for an abbreviated course, as others have found. 22 The alternative solution used by other major centres involving two weeks of inpatient care 23 is not sustainable in most health care systems due to exceptionally high costs.
Another limitation of our study is the absence of defecating proctograms, limiting our ability to fully characterize the constipated patients with a defecatory disorder, and perhaps including patients less likely to benefit from BF through the programme. Proctograms are very useful for defining anatomical abnormalities; however, they are not recommended prior to BF therapy by consensus groups such as the Rome Committee and there is no evidence that the information they provide will alter the BF therapy. Radiation exposure is an additional concern, especially as many patients were female and young and therefore more radiosensitive. Nevertheless, there were no differences in defecatory dynamics between patients in the two protocols, making a bias unlikely.
In conclusion, an abbreviated anorectal BF protocol offered to patients travelling from a long distance away provides substantial, at least short-term, improvements in constipation and FI, as well as in quality of life, satisfaction and feeling of control over bowel movements, that are not substantially different from a full protocol. Small advantages were seen for the more comprehensive protocol in terms of improvement in patient satisfaction with bowel movements and rectal sensation. Further work refining BF protocols, tailored to patient subtypes and desired outcomes, is warranted. Our study also suggests any further reduction in instrumented sessions below three or four may be detrimental. Although this study was performed in Australia, where distances to major medical facilities can be great, the same problems of access to BF services exist in more densely populated areas such as Europe and parts of the United States; hence, abbreviating the protocol while maintaining efficacy may have far-reaching ramifications.
Supplemental Material
Supplementary_Material – Supplemental material for Anorectal biofeedback: an effective therapy, but can we shorten the course to improve access to treatment?
Supplemental material, Supplementary_Material for Anorectal biofeedback: an effective therapy, but can we shorten the course to improve access to treatment? by Yoav Mazor, John E. Kellow, Gillian M. Prott, Michael P. Jones and Allison Malcolm in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
We wish to thank Alison Andrews for her assistance in data entry.
Specific author contributions
YM, AM and JEK planned the study. YM and GP collected all data, MJ and YM conducted statistical analysis and YM, MJ, AM and JEK interpreted the data and jointly drafted the manuscript. All authors reviewed and approved the final manuscript.
Funding
YM received an IPRS/APA Australian government scholarship for his studies at the University of Sydney.
Conflict of interest statement
The authors declare that there is no conflict of interest in preparing this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.