
Abstract
Background:
Proton-pump inhibitors (PPIs) are commonly used in clinical practice for gastric acid suppression. However, these agents have also been associated with certain negative clinical outcomes. We evaluated the real-world effects of incident PPI use on clinical outcomes in patients with Staphylococcus aureus bacteremia.
Methods:
This retrospective cohort study included patients admitted to Veterans Affairs hospitals with positive S. aureus blood cultures collected between 2002 and 2013 that received appropriate antibiotics within 48 hours of culture collection. Clinical outcomes among three PPI exposure groups, each compared to nonusers, were assessed with propensity-score-matched Cox proportional-hazard regression models: pretreated PPI users initiating therapy in the 30 days prior to culture and either (a) continuing PPI therapy after culture, or (b) not continuing after culture, and (c) de novo users initiating at culture.
Results:
Clinical outcomes, including inpatient mortality, intensive care discharge, 30-day mortality, 30-day readmission, and 30-day Clostridium difficile infection (CDI) were similar among PPI users and nonusers. Though length of stay was longer in pretreated, continuing PPI users [time-to-discharge hazard ratio (HR) 0.78, 95% confidence interval (CI) 0.65–0.93], 14-day mortality was significantly lower than in nonusers (HR 0.66, 95% CI 0.50–0.87).
Conclusions:
In our large national cohort study, PPIs were not associated with an increased risk of negative clinical outcomes, including mortality and CDI, in patients with S. aureus bacteremia.
Introduction
Proton-pump inhibitors (PPIs) are commonly used in clinical practice for gastric-acid suppression, particularly for the prevention of stress ulcers in critically ill patients. However, an increased risk of some negative clinical outcomes has been reported, including kidney disease, hypomagnesemia, bone fractures, pneumonia, and Clostridium difficile infections (CDIs).1,2 A recent study raised alarm by suggesting that initiating PPIs during hospital admission could increase the risk of inpatient mortality by about 90%. 3 While older data have suggested that acid suppression allows for increased intestinal bacteria, some analyses found this overgrowth occurred less with histamine antagonists, conceivably related to less potent gastric-acid suppression from histamine antagonists when compared with PPIs. 4 Moreover, PPIs have been associated with decreased leukocyte antimicrobial activity in vitro, as well as attenuated innate immune responses in vivo that may be beneficial in clearance of bacterial infection. 5 We thought it would be important to examine if these reported immunomodulatory effects described for PPIs translated into any clinical outcome differences in patients with invasive infection. Among the most common of invasive bacterial infection in humans, Staphylococcus aureus affects broad patient populations exhibiting high diversity in baseline host innate immune status. This study sought to evaluate the real-world effects of incident PPI use on clinical outcomes in patients with S. aureus bacteremia.
Methods
Data source
We utilized national Veterans Affairs (VA) databases, which contain health and administrative data captured from electronic medical records. The databases used included diagnoses and procedures from outpatient and inpatient care, laboratory and microbiology results, vital signs and vital status, and pharmacy data, including inpatient and outpatient administration and dispensing, and medications prescribed by non-VA providers or purchased by patients at non-VA pharmacies.
Study population
This retrospective cohort study included adult patients (age ⩾ 18 years) admitted to VA hospitals with positive blood cultures for S. aureus between 1 January 2002 and 1 December 2013. Initial antibiotic regimens within 48 hours of culture collection were reviewed and only those with appropriate regimens were selected for inclusion: intravenous β-lactam therapy (ampicillin-sulbactam, nafcillin, oxacillin, piperacillin–tazobactam, cefazolin, cefotetan, cefoxitin, ceftazidime, ceftriaxone, ceftaroline, ertapenem, doripenem, imipenem–cilastatin, or meropenem) or vancomycin for methicillin-susceptible S. aureus (MSSA) and vancomycin or ceftaroline for methicillin-resistant S. aureus (MRSA). If patients were discharged within 1 day of culture or died in that same timeframe, they were excluded. Once these criteria were applied, the first admission was selected for analysis.
This study was approved by the Institutional Review Board and Research and Development Committee of the Providence Veterans Affairs Medical Center.
As this study utilized existing health data, a waiver of informed consent was granted by the Institutional Review Board of the Providence Veterans Affairs Medical Center.
PPI use
Incident PPI use was defined as initiation of a PPI within the 30 days prior to culture or at culture, without PPI use in the previous year. Those initiating prior to culture were further categorized as continuing after culture and not continuing after culture, to assess whether lasting effects were observed after discontinuation. Nonusers were those with no record of PPI use in the year prior to culture or during the entire admission and served as the comparison group for all three PPI user groups (pretreated with continuation, pretreated without continuation, and de novo at culture).
Outcomes
The primary outcome was mortality as assessed within 30 days of the culture collection date and the secondary outcomes included 14-day mortality, inpatient mortality, hospital discharge, intensive care unit (ICU) discharge, 30-day readmission, and 30-day CDI (International Classification of Diseases, 9th edition, 008.45). We calculated time for each endpoint from the culture collection date to the event date, and censoring was used in the assessments of discharge, readmission, and CDI for patients who died.
Statistical analysis
We developed three separate propensity-score models for each PPI exposure group that controlled for initial antibiotic treatment, treating facility, treating specialty, infection source, previous healthcare exposures, demographics, current comorbidities, medical history, and other clinical characteristics, such as MSSA/MRSA (Appendix 1 in the Supplementary Material). We confirmed goodness of fit and absence of multicollinearity in the propensity-score models. Nonusers were then matched to users on their propensity score using nearest neighbor matching within 0.005 caliper. Lastly, Cox proportional hazard regression models were used to quantify the hazard ratio (HR) and 95% confidence interval (CI) for all outcomes. Analyses were performed using SAS software version 9.2 (SAS Institute Inc., Cary, NC, USA).
Results
Our study included 653 pretreated PPI users without continuation, 642 pretreated PPI users with continuation, 900 de novo PPI users, and 11,840 nonusers, all with S. aureus bacteremia (Figure 1). Table 1 lists demographics and clinical characteristics of patients in each of these groups prior to implementation of propensity-score matching. PPI users differed considerably from nonusers, in terms of demographic characteristics, source of infection, comorbidity burden, and medical history. Due to these significant differences, these variables were included in the propensity-score models. Each model demonstrated goodness of fit, allowing strong discrimination between the groups, with high C statistics of 0.82–0.90, and due to the small caliper used for identifying matches, complete overlap in propensity-score distributions between PPI users and nonusers was obtained.

Study cohort identification.
Demographic and clinical characteristics in proton-pump inhibitor users and nonusers.
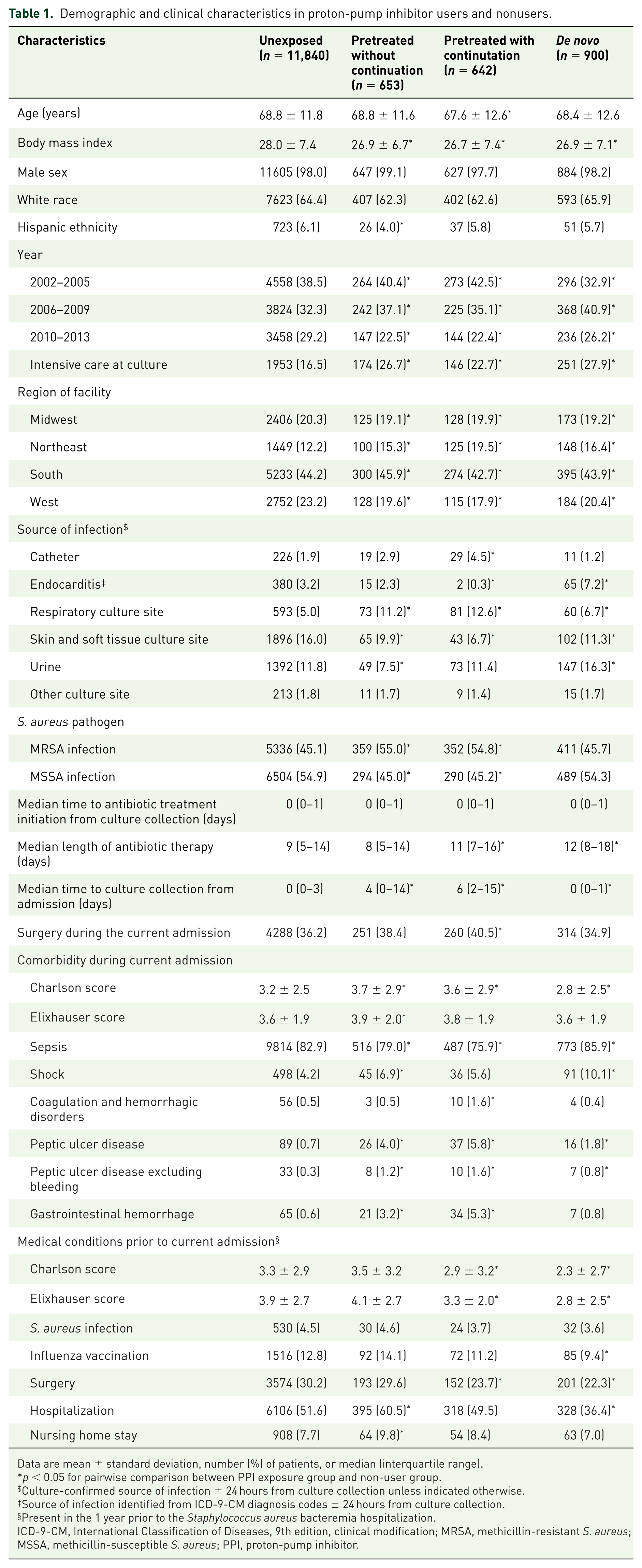
Data are mean ± standard deviation, number (%) of patients, or median (interquartile range).
p < 0.05 for pairwise comparison between PPI exposure group and non-user group.
Culture-confirmed source of infection ± 24 hours from culture collection unless indicated otherwise.
Source of infection identified from ICD-9-CM diagnosis codes ± 24 hours from culture collection.
Present in the 1 year prior to the Staphylococcus aureus bacteremia hospitalization.
ICD-9-CM, International Classification of Diseases, 9th edition, clinical modification; MRSA, methicillin-resistant S. aureus; MSSA, methicillin-susceptible S. aureus; PPI, proton-pump inhibitor.
In propensity-matched analyses of the aforementioned clinical outcomes, there were few differences observed between PPI users and nonusers (Table 2). Inpatient mortality, intensive care discharge, 30-day mortality, 30-day readmission, and 30-day CDI were similar among PPI users and nonusers. In pretreated PPI users with continuation, the 14-day mortality rate was significantly lower (HR 0.66, 95% CI 0.50–0.87) despite a lower discharge rate (HR 0.78, 0.65–0.92). This lower discharge rate, which reflected a longer length of stay, was also observed in de novo PPI users (HR 0.85, 95% CI 0.74–0.97) as compared with nonusers. Similar results were observed in sensitivity analyses that excluded patients with a C. difficile diagnosis code during the S. aureus bacteremia admission, where 14-day mortality was significantly lower (HR 0.62, 95% CI 0.42–0.92) among pretreated PPI users with continuation, despite a lower discharge rate (HR 0.74, 0.60–0.90), and a lower discharge rate was also observed for de novo PPI users (HR 0.75, 95% CI 0.64–0.87; data not presented in tables).
Clinical outcomes in propensity-matched proton-pump inhibitor users and nonusers.
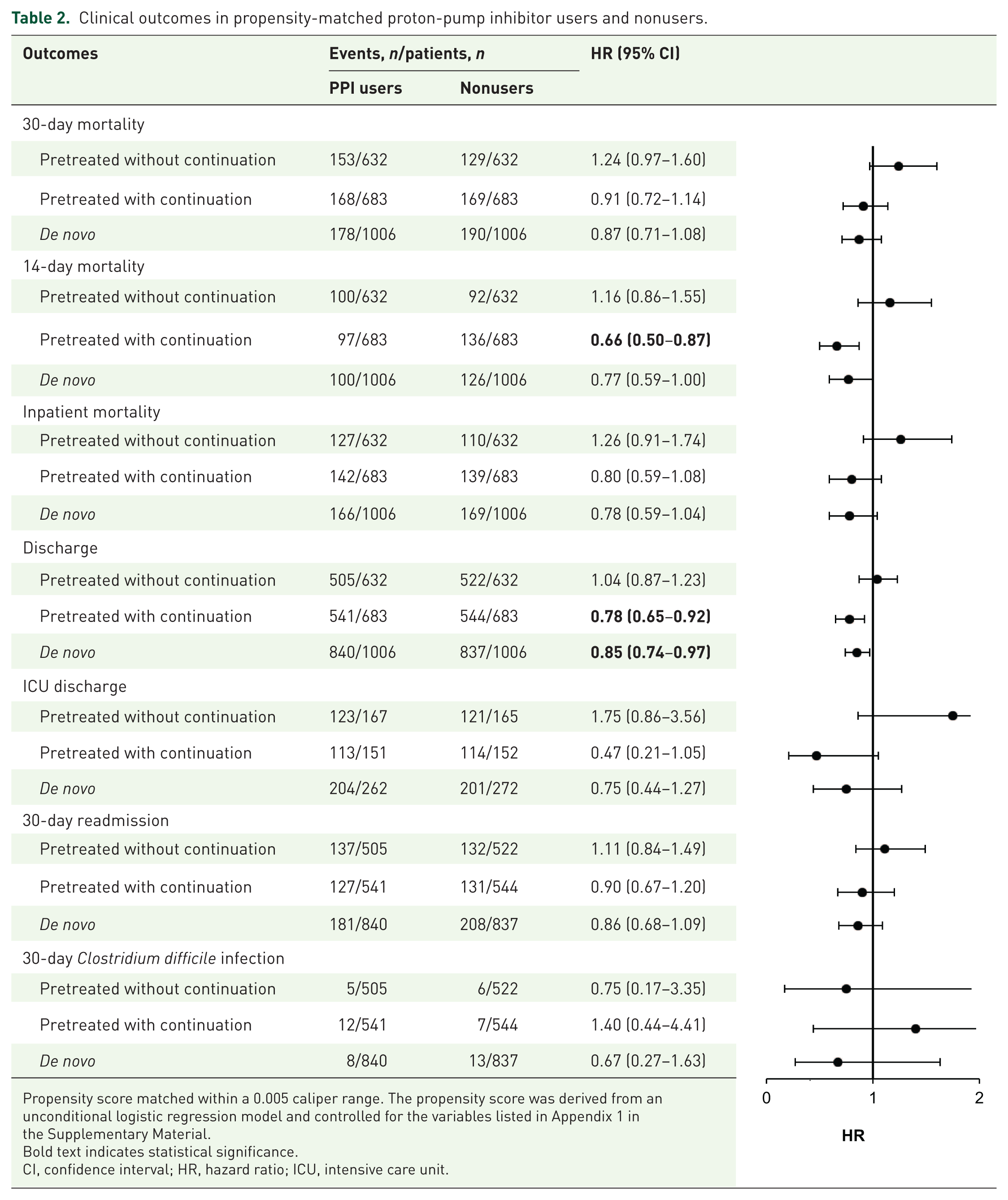
Propensity score matched within a 0.005 caliper range. The propensity score was derived from an unconditional logistic regression model and controlled for the variables listed in Appendix 1 in the Supplementary Material.
Bold text indicates statistical significance.
CI, confidence interval; HR, hazard ratio; ICU, intensive care unit.
Discussion
PPIs have been shown in various studies to inhibit neutrophil functions that are critical in bacterial clearance, including production of reactive oxidative species, chemotaxis, and phagolysozome acidification.6,7 In addition, certain PPIs are reported to reduce expression of integrins CD11b and CD18 on the neutrophil surface and expression of adhesion molecules ICAM-1 and VCAM-1 on endothelial cells, potentially compromising transcytosis of the immune cells to tissue foci of infection. 8 Consistent with such laboratory data is previous clinical evidence suggesting poorer clinical outcomes in patients treated with PPIs, including increased risk for C. difficile infections and mortality.2,3
Seeking to determine whether PPIs influence clinical outcomes in patients with S. aureus bacteremia, we found similar outcomes between PPI users with varying exposure patterns as compared with nonusers, in agreement with a recent meta-analysis of 19 randomized trials conducted among critically ill patients. 9 As the included randomized trials evaluated prophylactic PPI use, these studies most likely reflect a de novo exposure pattern, however the number of studies excluding patients with preadmission PPI use was not reported. Pneumonia, mortality, and ICU length of stay were similar among those randomzied to PPIs versus histamine-2-receptor antagonists (H2RAs), with a relative risk of 1.12 (95% CI 0.86–1.46) and 1.05 (95% CI 0.87–1.27) for pneumonia and mortality, respectively, and a mean difference in ICU length of stay of −0.38 days (95% CI −1.49 to 0.74). None of the included 19 studies reported CDIs.
While multiple meta-analyses have found an association between PPI use and CDIs, heterogeneity among studies evaluated has been consistently high (I2 > 85%) reflecting variability in the associated risk among studies, and significant limitations of existing studies have been noted.10,11 A recent study evaluating the risk of CDI among intensive care unit patients suggests some patient populations may not have the same associated risk, consistent with our results. 12 In this large multicenter study among 18,134 patients, PPI use did not lead to a significant increase in CDI [adjusted hazard ratio (aHR) 1.56; 95% CI 0.72–3.35] among patients not receiving antibiotics and was protective in those receiving antibiotics (aHR 0.64; 95% CI 0.48–0.83). Further studies should seek to determine in which patient populations PPIs may be safely used without conferring increased CDI risk.
Several limitations to our study should be noted. First, over-the-counter use of PPIs may not have been reported during clinical visits and hospitalizations. Second, we utilized diagnosis codes to operationally define certain conditions, such as CDI, which may result in misclassification. For example, presence of diagnosis codes may not always reflect active problems and may be used to reflect history of the condition, or even colonization in the case of C. difficile. Third, residual confounding may be present due to unmeasured confounders, despite our efforts to control for many confounders using propensity-score methods. Fourth, our study was conducted among patients receiving care at VA hospitals, and included mostly older males.
Conclusion
Rates of negative clinical outcomes were similar among PPI users and nonusers in our large, national, real-world cohort study. As this is one observational study from a single-study population, our results should be substantiated in other study populations. If rates of negative clinical outcomes, such as mortality and CDI, are found to be similar between PPI users and nonusers with serious infections then the clinical benefits of PPI use under appropriate indications may outweigh the potential risk of certain other adverse events that have been attributed to PPI use.
Supplemental Material
PPIs_in_SA_Bacteremia_Appendix – Supplemental material for Proton-pump inhibitors do not influence clinical outcomes in patients with Staphylococcus aureus bacteremia
Supplemental material, PPIs_in_SA_Bacteremia_Appendix for Proton-pump inhibitors do not influence clinical outcomes in patients with Staphylococcus aureus bacteremia by Aisling R. Caffrey, Tristan T. Timbrook, Syed Raza Ali, Victor Nizet and George Sakoulas in Therapeutic Advances in Gastroenterology
Supplemental Material
PPIs_in_SA_Bacteremia_Strobe – Supplemental material for Proton-pump inhibitors do not influence clinical outcomes in patients with Staphylococcus aureus bacteremia
Supplemental material, PPIs_in_SA_Bacteremia_Strobe for Proton-pump inhibitors do not influence clinical outcomes in patients with Staphylococcus aureus bacteremia by Aisling R. Caffrey, Tristan T. Timbrook, Syed Raza Ali, Victor Nizet and George Sakoulas in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
The views expressed are those of the authors and do not necessarily reflect the position or policy of the United States Department of Veterans Affairs. This work was presented, in part, at the 32nd International Conference on Pharmacoep-idemiology and Therapeutic Risk Management, 28 August 2016. This material is based upon work supported, in part, by the Office of Research and Development, Department of Veterans Affairs. George Sakoulas and Victor Nizet have research support under a National Institutes of Health grant (1U54HD090259). We appreciate the assistance of Vrishali Lopes with data preparation and analyses.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest statement
Aisling Caffrey has received research funding from Pfizer, Merck (Cubist), and The Medicines Company. Tristan Timbrook has received honoraria for speaking and/or consulting from BioFire Diagnostics, GenMark Diagnostics, and Roche Diagnostics. Syed Raza Ali has no conflicts to disclose. Victor Nizet has received research funding or acted as an advisor for InhibRx, Centauri Therapeutics, Cidara Therapeutics, and Roche Pharmaceutical Research and Early Development. George Sakoulas has received speaking honoraria from Allergan, Sunovion, and The Medicines Company, and consulting fees from Allergan.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.