
Abstract
Background:
Standard treatment for patients with erosive esophagitis (EE) is proton-pump inhibitors (PPIs), but some patients are resistant to PPIs. We aimed to evaluate the acid-inhibitory effects and efficacy of a novel potassium-competitive acid blocker (vonoprazan) in patients with PPI-resistant EE.
Methods
This randomized, double-blind, multicenter study of vonoprazan evaluated gastric and esophageal pH over a 24-hour period as the primary endpoint and EE healing rate as the secondary endpoint. Following a 7 to 14-day run-in period (lansoprazole 30 mg treatment), patients with endoscopically confirmed PPI-resistant EE received vonoprazan 20 mg or 40 mg for 8 weeks.
Results
Patients were randomized to receive vonoprazan 20 mg (n = 9) or 40 mg (n = 10). Over a 24-hour period; both groups showed a significant increase from baseline in the percentage of time gastric pH ≥ 4, referred to as pH 4 holding time ratio (HTR): an increase from 73.21% to 96.46% in the 20 mg group, and from 69.97% to 100.00% in the 40 mg group. Increases from baseline in esophageal pH 4 HTRs were not significant. The 40 mg group showed greater increases in gastric and esophageal pH 4 HTRs compared with the 20 mg group, but differences between groups were not significant. After 8 weeks’ treatment, the healing rate in subjects with baseline EE grades A–D was 60.0% (3/5 patients) in the 20 mg group and 71.4% (5/7 patients) in the 40 mg group. Vonoprazan was generally well tolerated. One patient (40 mg group) experienced four treatment-emergent adverse events (TEAEs) (unrelated to study drug), leading to study discontinuation.
Conclusions
Vonoprazan 20 mg and 40 mg effectively inhibited gastric acid secretion over a 24-hour period with significantly increased gastric pH 4 HTR, and resulted in an EE healing rate > 60.0% in this study. Vonoprazan treatment may be valuable for patients with PPI-resistant EE
Keywords
Introduction
Gastroesophageal reflux disease (GERD) is estimated to affect 10–20% of the adult population in the western world and 2.5–7.8% of the population in East Asia [Dent et al. 2005; Maradey-Romero and Fass, 2014]. Symptoms of GERD include heartburn and acid regurgitation, which can severely reduce quality of life in patients. The prevalence and chronic nature of the disease also constitute a significant burden on the healthcare systems and economies of affected countries. GERD can be classified into two broad categories: nonerosive reflux disease (NERD) and erosive esophagitis (EE). EE is characterized by injury to the esophageal mucosa, which results from exposure to refluxate [Altomare et al. 2013].
The severity of the mucosal injury can be graded according to criteria outlined in the Los Angeles (LA) Classification system using endoscopic examination [Lundell et al. 1999].
Proton-pump inhibitors (PPIs) are currently the standard treatment for EE, owing to their high efficacy for EE healing [Cicala et al. 2013]. Despite the effectiveness of PPIs, a significant proportion of patients with EE have been shown to be resistant to PPI treatment. Approximately 10–15% of patients do not achieve complete healing following 8 weeks of treatment with PPIs [Maradey-Romero and Fass, 2014]. Despite continued treatment with PPIs, 15–23% of EE patients with LA grades A and B and 24–41% of EE patients with LA grades C and D experience a relapse within 6 months [Maradey-Romero and Fass, 2014]. It has been suggested that insufficient acid inhibition is a major reason for the lack of EE healing observed in some patients. Of note, some PPIs are able to provide effective acid inhibition during the day, but have been found to be less effective overnight [Morelli et al. 2011].
Vonoprazan (TAK-438) is a novel, potassium-competitive acid blocker developed by Takeda Pharmaceutical Company Limited. Vonoprazan has a different mechanism of action and a number of advantages compared with PPIs; it does not require an acidic environment for activation, it is acid stable, and it has been shown to rapidly exert an acid-inhibitory effect (PPIs require 3–5 days for maximal effect). Preclinical studies demonstrated that the acid inhibition achieved by vonoprazan was more potent and longer lasting than that with PPIs [Hori et al. 2010, 2011; Matsukawa et al. 2011]. Importantly, recent clinical trials have also shown vonoprazan to be noninferior to the PPI lansoprazole in terms of EE healing [Ashida et al. 2015, 2016]. Furthermore, Ashida and coworkers showed that at doses of 20 mg and 40 mg, vonoprazan was more effective than lansoprazole in some patients with severe EE (LA grades C/D) [Ashida et al. 2015]. This suggests that vonoprazan may be useful for treating patients with EE who have not completely responded to standard doses of PPIs.
The objectives of this study were to evaluate the acid-inhibitory effects and the efficacy of vonoprazan at two different doses (20 mg and 40 mg) in patients with PPI-resistant EE.
Materials and methods
Study design
This was a randomized, double-blind, multicenter study to evaluate the acid-inhibitory effects and the efficacy of vonoprazan (20 mg and 40 mg) in patients with PPI-resistant EE. The study consisted of a run-in period (7–14 days) followed by an 8-week treatment period (Figure 1). This study was conducted between 10 August 2012 and 17 September 2013 at eight sites in Japan. Approval for this study was obtained from the institutional review board at each study site and the study was conducted in accordance with the World Medical Association Declaration of Helsinki, the International Conference on Harmonization Harmonized Tripartite Guideline for Good Clinical Practice, and applicable Japanese regulatory requirements. All patients were required to provide written consent in order to participate in the study. This study was registered at ClinicalTrials.gov with the identifier NCT01630746.

Study design and treatment periods.
Study population
In order to be eligible for the study, patients had to be male or female, aged 20 years or older, and should have been receiving regular doses (or higher) of PPIs (lansoprazole 30 mg, omeprazole 20 mg, rabeprazole 10 or 20 mg, or esomeprazole 20 mg) for treatment of EE for at least 8 weeks until the start of the run-in period. At 2 days before the end of the run-in period, patients had to have endoscopically confirmed EE with an LA grade between A and D, despite previous treatment with regular (or higher) doses of PPIs and treatment with 30 mg of lansoprazole (compliance level ≥ 80%) during the run-in period. The main exclusion criteria were: esophageal complications other than Schatzki’s ring and Barrett’s esophagus; history of surgery or treatment affecting gastroesophageal reflux; upper gastrointestinal bleeding, or gastric or duodenal ulcer (characterized by a defective mucosa with white coating) at the start of the run-in period; currently or previously affected by Zollinger-Ellison syndrome; history of hypersensitivity or allergies to vonoprazan (including formulatory components) or PPIs; requiring treatment with excluded medications (medications for the gastrointestinal tract or for Helicobacter pylori eradication, strong CYP3A4 inhibitors, and other medications for which concomitant use with lansoprazole was contraindicated); serious neurological, cardiovascular, pulmonary, hepatic, renal, metabolic, gastrointestinal, urologic, endocrinologic, or hematologic disorders; presence of acquired immunodeficiency syndrome or hepatitis, or a positive test for the hepatitis B surface antigen or the hepatitis C virus antibody.
Randomization and treatment
During the run-in period, patients received 30 mg of lansoprazole orally once daily for at least 7 days and up to a maximum of 14 days. Randomization of the patients occurred at the end of the run-in period, following confirmation of EE (by endoscopy) by the study investigator, the day before the treatment period was due to begin. Patients were randomly assigned to receive 20 mg of vonoprazan or 40 mg of vonoprazan in a 1:1 ratio, according to a prespecified randomization schedule generated by randomization personnel designated by the sponsor. During the treatment period, patients received the designated dose of vonoprazan orally once daily for 8 weeks.
Outcome measures
Acid-inhibitory effect (pharmacodynamics)
The primary pharmacodynamic endpoints were the time course of both gastric and esophageal pH changes over 24 hours at steady state during the treatment period. These changes were measured as the percentage of time the pH was ≥4, referred to as the pH 4 holding time ratio (HTR). Gastroesophageal pH monitoring of patients (over a 24-hour period) was carried out twice; once on the day before the end of the run-in period (following at least 6 days of receiving lansoprazole), constituting the baseline and once 2 weeks after the start of the treatment period (following at least 7 days of vonoprazan treatment). Gastroesophageal pH was measured for at least 24 hours using a glass pH electrode (CM-200W; Chemical Instruments, Tokyo, Japan) and a pH monitor (PH-101ZG; Chemical Instruments, Tokyo, Japan). The catheter-guided pH electrode was calibrated using standard pH 4 and pH 7 solutions before being inserted transnasally into the patient’s stomach; correct positioning of the probe was confirmed by X-ray.
Evaluation of efficacy
The secondary endpoint of the study was the EE healing rate after 8 weeks of treatment with vonoprazan. Healing was defined as having no endoscopically confirmed mucosal breaks. The EE healing rate was defined as the percentage of patients with endoscopically confirmed EE healing, as decided by the investigator. Photographs of each patient’s esophagus under fasting conditions was examined by the investigator, who graded the severity of the EE according to the LA classification system. In this study, no mucosal break was classified as grade 0. Patients were enrolled in the study based on the assessment of the severity of their EE at baseline by the investigator. A central adjudication committee (CAC) also assessed and graded the severity of EE in patients at baseline, according to the LA classification system. The analysis of healing rate excluded patients for whom baseline EE was classified as grade 0 by the CAC. However, the originally planned healing rate analysis was to have been conducted using the investigator-determined classifications of EE grade.
Safety and tolerability
Safety variables assessed included treatment-emergent adverse events (TEAEs), serious adverse events (SAEs), clinical laboratory test values, electrocardiogram (ECG) findings, vital signs, and levels of serum gastrin and pepsinogen I/II.
Statistical analysis
A sample size of 10 patients per group (20 in total) was planned for evaluation of the primary endpoint; the sample size for this study was based on what was considered feasible and was not statistically derived. The full analysis set and the safety analysis set were defined as all patients who were randomized and received at least one dose of vonoprazan. For the primary endpoint, the gastric and esophageal pH 4 HTRs and their changes from baseline were described using descriptive statistics and two-sided 95% confidence intervals (CIs) for each group. The point estimate of the difference in change from baseline between groups (40 mg group–20 mg group) was calculated for gastric and esophageal pH 4 HTRs with 95% CIs using an analysis of variance with treatment group as a fixed effect. The analyses of gastric and esophageal pH 4 HTRs over the 24-hour period were also repeated for the same measurements made during the two 12-hour periods. For the secondary endpoint, the point estimate and two-sided 95% CI of the healing rate were calculated. The point estimate and the two-sided 95% CI of the difference in EE healing rates between the groups were also calculated. Data analyses were performed using SAS release 9.2 (SAS Institute Inc., Cary, NC, USA).
Results
Demographic and baseline clinical characteristics
A total of 25 patients provided informed consent and of these, six patients were not randomized; one patient did not meet the inclusion criteria and five patients were excluded for ‘other’ reasons (Figure 2). Of the 19 patients randomized, nine were allocated to the vonoprazan 20 mg group and 10 to the vonoprazan 40 mg group. All 19 patients enrolled received at least one dose of the study drug and 18 patients completed the 8-week study. One patient in the 40 mg group discontinued study treatment prematurely due to TEAEs (Figure 2).

Patient disposition (CONSORT flow chart).
No clinically meaningful differences were observed between groups at baseline, with the exception of the classification of EE (Table 1). As assessed by the investigator, both groups had similar numbers of patients classified as having Grade A/B EE (six patients in the 20 mg group and seven patients in 40 mg group) or Grade C/D EE (three patients in each group). However, the CAC assessed four patients in the 20 mg group and two patients in the 40 mg group as having Grade 0 EE (no mucosal breaks).
Patient characteristics at baseline.
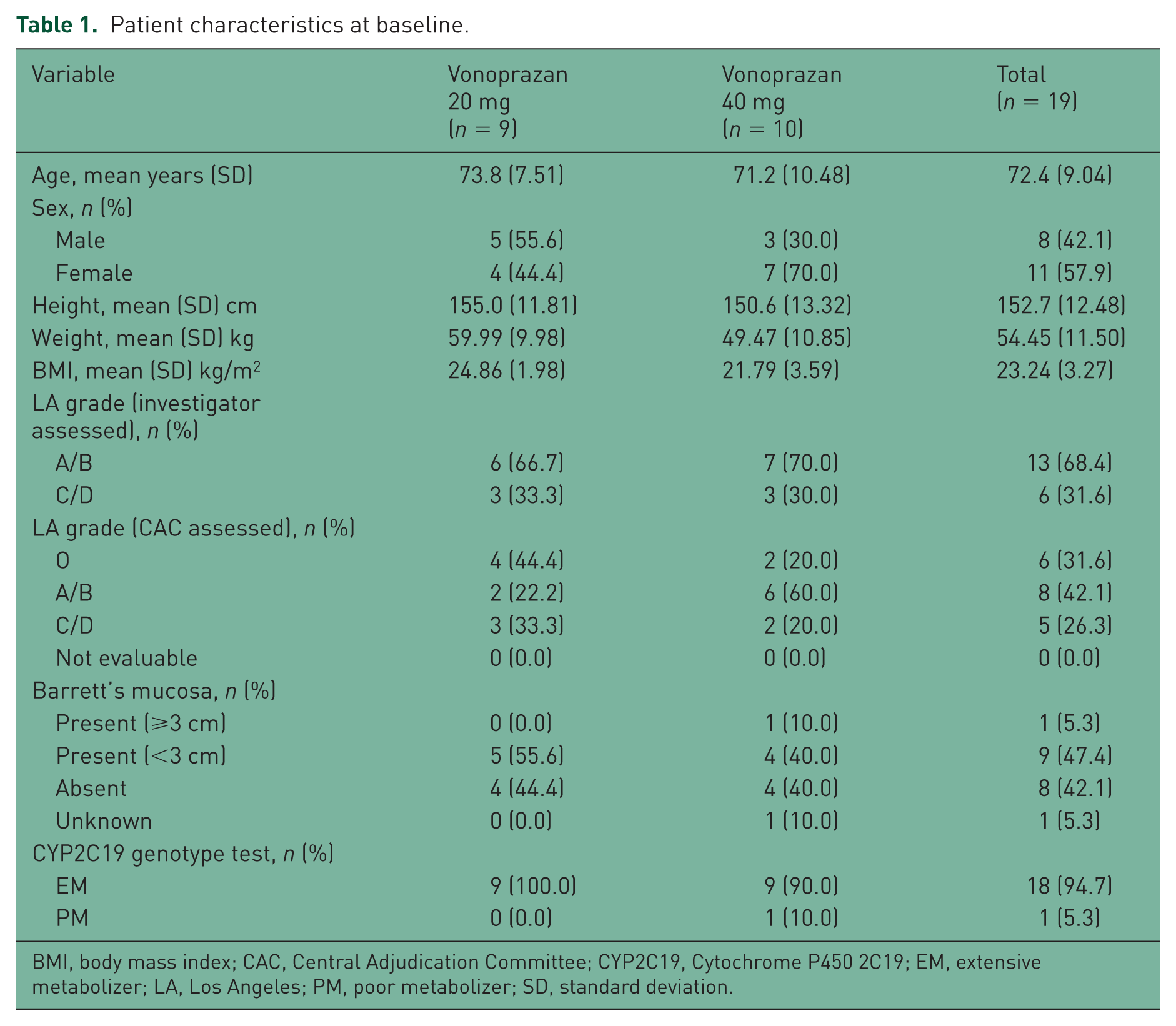
BMI, body mass index; CAC, Central Adjudication Committee; CYP2C19, Cytochrome P450 2C19; EM, extensive metabolizer; LA, Los Angeles; PM, poor metabolizer; SD, standard deviation.
There were also differences in the number of patients in each group classified by the CAC as having Grade A/B EE (two in the 20 mg group and six in the 40 mg group, versus six and seven respectively, as assessed by the investigator). As was the case when assessed by the investigator, similar numbers of patients from each group were classified by the CAC as having Grade C/D EE (three in the 20 mg group and two in the 40 mg group).
Pharmacodynamics
Gastric holding time ratio
Following 2 weeks of vonoprazan treatment, patients treated with either 20 mg or 40 mg of vonoprazan showed an increase in the percentage of total time during which their gastric and esophageal pH readings were equal to or above 4 (pH 4 HTRs) compared with baseline (Table 2). The 24-hour gastric pH 4 HTR increased from 73.21% (at baseline) to 96.46% in the 20 mg group and from 69.97% (at baseline) to 100.00% in the 40 mg group. These increases were significant, as indicated by the fact that the lower limits of the 95% CIs of the mean changes from baseline (of the 24-hour gastric pH 4 HTR) were greater than 0 in both groups. A significant increase in the gastric pH 4 HTRs was observed in both groups during both daytime (0–12 hours; 9 am–9 pm) and night-time (12–24 hours; 9 pm–9 am), although the increase was larger during the night-time period for both groups.
pH 4 holding time ratios.

Daytime (9 am–9 pm); $night-time (9 pm–9 am).
CI, confidence interval; h, hours; HTR, holding time ratio.
Esophageal holding time ratio
The 24-hour esophageal pH 4 HTRs increased from 96.51% (at baseline) to 98.41% in the 20 mg group and from 94.27% (at baseline) to 99.86% in the 40 mg group. These increases in the esophageal pH 4 HTRs were not significant in either group. Patients treated with 40 mg of vonoprazan showed greater increases in both gastric and esophageal pH 4 HTRs compared with patients treated with 20 mg of vonoprazan, but these differences were not statistically significant.
Efficacy
Following 8 weeks of treatment with vonoprazan, endoscopic assessment (excluding patients for whom baseline EE was classified as grade 0 by the CAC, which was not originally planned) showed that 3/5 patients in the 20 mg group and 5/7 patients in the 40 mg group had confirmed EE healing, resulting in EE healing rates of 60.0% and 71.4%, respectively (Table 3). The highest healing rate was observed for patients with EE graded as A/B at baseline (as assessed by the CAC) who were treated with 40 mg of vonoprazan; this group had a healing rate of 80% (4/5 patients). Patients with EE graded as A/B (as assessed by the CAC) treated with 20 mg of vonoprazan and all patients with EE graded as C/D (as assessed by the CAC) had similar healing rates (50.0–66.7%), irrespective of dose (Table 3).
Summary of erosive esophagitis healing rate after 8-week treatment period (as assessed by investigator).

Graded by the CAC; **totals do not include patients for whom baseline EE was classified as grade 0 (vonoprazan 20 mg, n = 4; vonoprazan 40 mg, n = 2) by the CAC.
LA, Los Angeles.
Gastric and esophageal pH profiles of nonhealed patients
Vonoprazan treatment appeared to increase gastric pH in patients for whom baseline EE was classified as Grades A–D by the CAC but did not have confirmed EE healing (Figure 3). For all four of these patients, gastric pH was generally higher and less variable (reflected by fewer periods of lower pH) at week 2 compared with baseline. In contrast, esophageal pH levels were similar at week 2 compared with baseline for all four of these patients, although they were less variable (reflected by fewer periods of lower pH) at week 2 than at baseline for two of these patients. The pattern of pH response was very similar for healed and nonhealed patients (Figure 4).

Gastric and esophageal pH profiles of nonhealed patients, according to baseline and week 8 erosive esophagitis grades: (a) nonhealed patient one, LA grade B at baseline, LA grade B at week 8; (b) nonhealed patient two, LA grade D at baseline, LA grade D at week 8; (c) nonhealed patient three, LA grade B at baseline, LA grade B at week 8; (d) nonhealed patient four, LA grade D at baseline, LA grade D at week 8.*
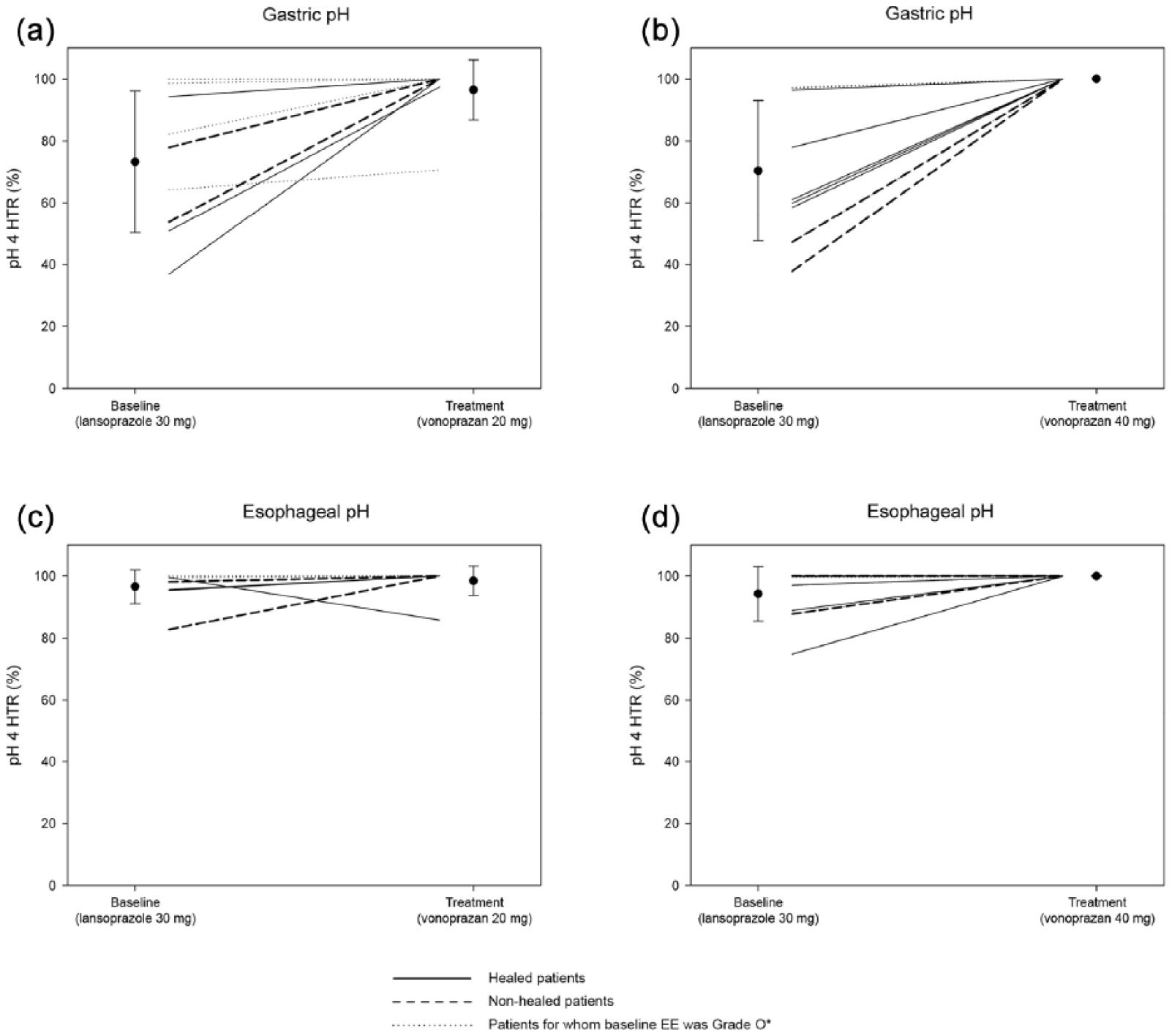
Patterns of gastric and esophageal pH for healed patients, nonhealed patients, and patients for whom baseline erosive esophagitis was classified as grade 0 by the central adjudication committee: (a) gastric pH, 20 mg vonoprazan group; (b) gastric pH, 40 mg vonoprazan group; (c) esophageal pH, 20 mg vonoprazan group; (d) esophageal pH, 40 mg vonoprazan group.
Safety and tolerability measures
TEAEs were reported by 4/9 (44.4%) patients in the 20 mg group and by 6/10 (60.0%) patients in the 40 mg group (Table 4). Drug-related TEAEs were reported by 1/9 (11.1%) patients in the 20 mg group and by 1/10 (10.0%) patients in the 40 mg group (Table 4). The drug-related TEAEs reported were psoriasis in the 20 mg group and gastric mucosal lesion in the 40 mg group (Table 5). All TEAEs reported were mild or moderate in intensity; no severe TEAEs or SAEs were reported in either group during the study. There was no obvious increase in the incidence of TEAEs by preferred term in either group during the treatment period. One patient in the 40 mg group experienced four TEAEs (pyrexia, fall, and two instances of muscular weakness), which were unrelated to the study drug. These TEAEs resulted in the patient being discontinued from the study.
Summary of treatment-emergent adverse events.

TEAE, treatment-emergent adverse event.
Treatment-emergent adverse events by preferred term.
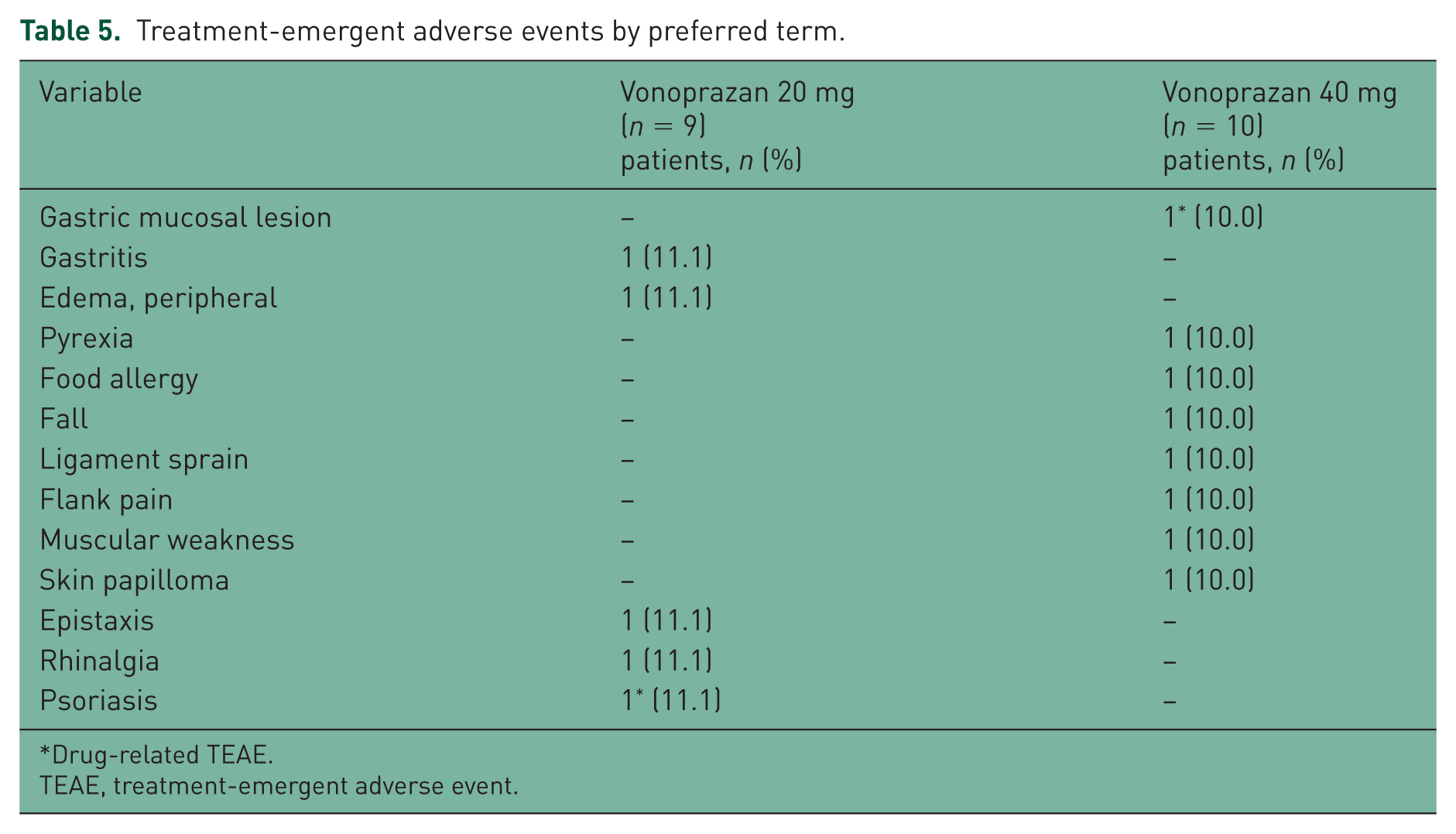
Drug-related TEAE.
TEAE, treatment-emergent adverse event.
There were no clinically significant changes in clinical laboratory test values, vital signs, or ECG findings observed during the study. Increases were observed in the mean levels of serum gastrin, pepsinogen I, and pepsinogen II in both groups after the start of treatment. The increase in serum gastrin levels was greater in the 40 mg group throughout the study, except at week 4. The greatest increases in the levels of pepsinogen I and II were observed at week 2 in both groups (Figure 5).
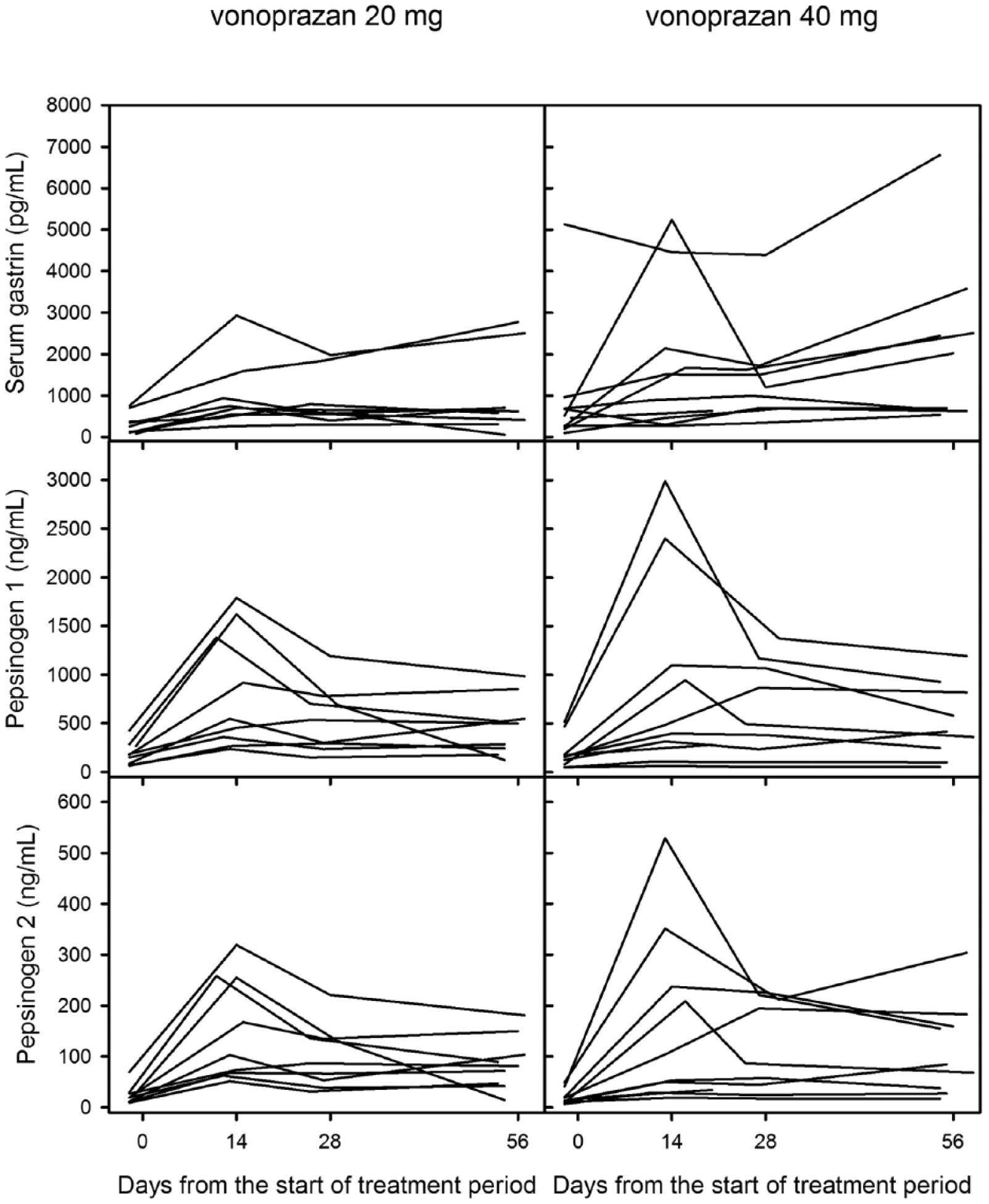
Time courses of serum gastrin, pepsinogen I and pepsinogen II.
Discussion
This is the first randomized, controlled trial to evaluate the acid-inhibitory effect and efficacy of vonoprazan in patients with PPI-resistant EE. This study demonstrated that vonoprazan at doses of 20 mg and 40 mg can effectively inhibit gastric acid secretion over 24 hours. Indication of the efficacy of vonoprazan was suggested by EE healing rates of 44.4% (4/9 patients) and 55.6% (5/9 patients) in the 20 mg and 40 mg groups, respectively. Vonoprazan was found to have a favorable safety and tolerability profile, with all TEAEs being mild or moderate in severity. Together, these results indicate that vonoprazan could be an effective and well tolerated treatment for patients with EE that is resistant to PPIs.
The strengths of this study include the fact that it was a randomized, double-blind, multicenter trial, and the fact that the presence of PPI-resistant EE in each patient was confirmed by endoscopy. Furthermore, data on both efficacy (healing rate) and gastroesophageal pH levels were recorded for each patient, allowing a closer examination of the association between acid inhibition and healing of PPI-resistant EE. This study was limited by the small sample size and the lack of a placebo or active control arm. Although the natural healing of reflux esophagitis after failure of PPI is possible, the acid-suppressive effects seen with vonoprazan in this study suggest that our findings are unlikely to be spurious. Another limitation is the fact that efficacy was based solely on the proportion of patients demonstrating complete healing of mucosal breaks. Moreover, the interpretation of the results was complicated by discrepancies between the investigator’s and the CAC’s endoscopic assessment of LA Grade at baseline.
It has been suggested that the persistence of EE despite PPI treatment is due to insufficient inhibition of gastric acid. At both doses, patients treated with vonoprazan in this study were able to achieve 24-hour pH 4 HTRs of 90% or greater after 2 weeks (Table 2). These results are similar to those observed in phase I studies of vonoprazan in healthy male subjects in Japan and the United Kingdom (UK), as described by Jenkins and coworkers [Jenkins et al. 2015]. At day 7, 24-hour pH > 4 HTRs of 83.4% and 100% were observed for subjects in Japan receiving 20 mg and 40 mg of vonoprazan, respectively [Jenkins et al. 2015]. For subjects in the UK, 24-hour pH > 4 HTRs of 85.2% and 93.2% were observed for subjects receiving 20 mg and 40 mg of vonoprazan, respectively [Jenkins et al. 2015].
Similar results were also observed in a cross-over study comparing vonoprazan with esomeprazole and rabeprazole in healthy male subjects in Japan, as described by Sakurai and coworkers [Sakurai et al. 2015]; vonoprazan was shown to result in 24-hour pH 4 HTRs of 85.8% or greater at day 7. Given that previous studies showing effective acid inhibition by vonoprazan (as demonstrated by pH 4 HTRs) were carried out in healthy subjects [Jenkins et al. 2015; Sakurai et al. 2015], the results of this study indicate that the acid-inhibitory effects of vonoprazan are similar in patients with PPI-resistant EE.
Vonoprazan has also been shown to inhibit gastric acid secretion throughout the night in both PPI-resistant EE patients as well as in healthy subjects [Jenkins et al. 2015; Sakurai et al. 2015]. In the present study, inhibition of gastric acid by vonoprazan was maintained throughout the night, with pH 4 HTRs of 93% or greater being observed between 12 and 24 hours (9 pm–9 am, Table 2). In the phase I study of vonoprazan by Jenkins and coworkers, pH > 4 HTRs for 20 mg of vonoprazan were between 73.0% and 75.4% throughout the night [Jenkins et al. 2015]; in the cross-over study comparing vonoprazan with esomeprazole and rabeprazole, pH 4 HTRs for 20 mg of vonoprazan were between 75.2% and 88.8% throughout the night [Sakurai et al. 2015]. The intragastric pH values of both EE patients and healthy subjects have been observed to follow a circadian pattern, with the pH decreasing during the nocturnal fasting period (the first part of the night) [Zentilin et al. 2003]. Although PPIs are able to effectively control gastric pH during the day, markedly lower pH 4 HTRs have been observed at night-time in patients treated with PPIs [Morelli et al. 2011; Sakurai et al. 2015]. Maintaining acid inhibition throughout the night is important, as this increases gastric and esophageal pH 4 HTRs, which in turn correlates with improved healing of EE [Katz et al. 2007]. An especially low intragastric pH during the night-time period may also be a good predictor of low EE healing rate [Yuan and Hunt, 2010].
Given that vonoprazan resulted in high (>80%) pH 4 HTRs in this study, as well as in previous studies [Jenkins et al. 2015; Sakurai et al. 2015], it was predicted that vonoprazan would be successful in healing the PPI-resistant EE in these patients. Previous studies in patients with EE have shown that treatment with vonoprazan, even with doses as low as 5 mg, resulted in healing rates of >92% after 4 weeks [Ashida et al. 2015]. Following 8 weeks of treatment with 20 mg of vonoprazan, the healing rate was 99% [Ashida et al. 2016]. Vonoprazan, at both 20 mg and 40 mg, was also shown to be noninferior to lansoprazole 30 mg in terms of efficacy [Ashida et al. 2015, 2016].
In this study, both doses of vonoprazan were effective in healing PPI-resistant EE, albeit at lower healing rates than observed for patients with EE. The moderate overall healing rate observed may be partly explained by the small sample size, which was reduced further by the fact that the healing analysis excluded a significant proportion (32%) of patients who were classified by the CAC as having no mucosal breaks at baseline (the investigator had classified these same patients as having Grades A–D EE at baseline). Vonoprazan did appear to increase gastric pH in nonhealed patients, so factors other than effects on pH may have contributed to lack of healing. Possible reasons for the lack of observed healing may include reflux of bile juices and atypical presentation of EE (e.g. mucosal break in the middle of the esophagus).
The results of this study demonstrate that some patients with PPI-resistant EE derive clinical benefit from treatment with vonoprazan. This is especially important given the limited treatment options for patients with PPI-resistant EE; vonoprazan may be a viable treatment for this subset of patients with EE. Further clinical trials are needed to confirm these findings.
Vonoprazan was found to have a favorable safety and tolerability profile, which has also been observed in several other studies. In previous trials, vonoprazan was well tolerated, with most TEAEs being mild or moderate in intensity [Ashida et al. 2015; Jenkins et al. 2015; Sakurai et al. 2015; Ashida et al . 2016]. Elevated levels of serum gastrin, pepsinogen I and pepsinogen II, resulting from vonoprazan treatment, have also been observed in previous studies [Ashida et al. 2015, 2016].
In conclusion, vonoprazan at doses of 20 mg and 40 mg was found to effectively inhibit gastric acid secretion over a 24-hour period, both during the daytime and night-time, and resulted in the healing of EE in some patients who had failed previous treatment with a PPI. Vonoprazan had a favorable safety and tolerability profile and may be considered a viable treatment option for patients with EE that is resistant to PPIs.
Footnotes
Acknowledgements
The authors would like to thank all study participants, as well as the following investigators: Kenji Furuta (currently at Otsu Medical Clinic, Izumo, Japan, and formerly of Shimane University Faculty of Medicine, Izumo, Japan); Takahisa Furuta (Hamamatsu University School of Medicine, Hamamatsu, Japan); Norihisa Ishimura (Shimane University Faculty of Medicine, Izumo, Japan); Ryuichi Iwakiri (Saga Medical School, Saga, Japan); Noriyuki Kawami (Department of Gastroenterology, Nippon Medical School, Graduate School of Medicine, Tokyo, Japan); Tomoyuki Koike (Tohoku University Graduate School of Medicine, Sendai, Japan); Nobutoshi Kuniyoshi (Kuniyoshi Hospital, Kochi, Japan) and Shinichi Takahashi (Kyorin University School of Medicine, Mitaka, Japan). All authors participated in the study design, interpretation of study results, and in the drafting, critical revision, and approval of the final version of the manuscript. KK and HO conducted the statistical analysis.
Funding
This study was sponsored by Takeda Pharmaceutical Company Limited, manufacturer/licensee of vonoprazan. Medical writing assistance was provided by Chu Kong Liew, PhD, and Tania Dickson, PhD, of ProScribe, part of Envision Pharma Group, and was funded by Takeda Pharmaceutical Company Limited. ProScribe’s services complied with international guidelines for Good Publication Practice (GPP3).
Conflict of interest statement
YS, MS, HO, KK, and AN are employees of Takeda Pharmaceutical Company Limited. KI, NH, EU, and KA are all paid consultants for Takeda Pharmaceutical Company Limited. Takeda Pharmaceutical Company Limited was involved in the study design, data collection, data analysis and preparation of the manuscript.