
Abstract
Background:
The aim of the study was to compare the prognostic value of histological and endoscopic activity in patients with ulcerative colitis (UC).
Methods:
Patients in clinical remission for 1 year under treatment with mesalazine underwent a planned colonoscopy with biopsies. Histological activity was scored using the histological activity index (HAI). Endoscopic activity was scored using the Mayo endoscopic subscore (MES). The clinical course was evaluated measuring relapses needing steroids during a follow up of 3 years.
Results:
A total of 52 patients were enrolled into the study and followed up for 3 years. At baseline 29 patients (55.77%) had no endoscopic lesions, and 17 patients (32.69%) showed no histological alteration. At 3 years of follow up, overall, 26 patients (50%) were still in steroid-free remission. Using univariate logistic regression analysis, both histological (HAI ⩾ 1) and endoscopic activity (MES ⩾ 1) were significantly associated with outcome, showing, respectively, a relapse risk (odds ratio [OR]) 16.4 times higher than histological remission (HAI 0) (96% confidence interval [CI]: 3.2–84.3) and 6.3 times higher with respect to endoscopic remission (MES 0) (96% CI: 1.9–21.3). After multivariate logistic regression analysis, histological activity was the only factor significantly associated with outcome (OR 10.2; 95% CI: 1.7–59.4).
Conclusions:
Histological activity has the most powerful prognostic value in predicting the need for steroids in patients with UC in stable clinical remission on mesalazine. It could be considered as a target of therapy in UC.
Keywords
Introduction
Ulcerative colitis (UC) still has no definitive cure and its treatment mainly consists of hindering the immuno-inflammatory pathways responsible for intestinal inflammation. 1 The natural course of UC usually presents the clinician with two main therapeutic scenarios: to defeat the acute, active disease, and to prevent recurrences, maintaining remission for as long as possible.2,3 These two clinical conditions variously alternate, with a prevalence of clinical remission status during the course of this lifelong disease.4,5 Since prolonged remission reduces the cost of health care and improves the patient’s quality of life, 6 increasing attention has been paid to assessing the best condition that would guarantee a lower risk of recurrence. 7
To date, the best prognostic factor of long-term remission is so-called mucosal healing (MH), which is evaluated by endoscopy. MH is associated with less need for steroids, avoidance of colectomy and long-term patient wellness.8,9 This finding is easily understandable since endoscopy directly describes lesions while clinical evaluation refers only to signs and symptoms of intestinal inflammation.
On the basis of the observation that microscopic inflammation can underlie even macroscopically normal mucosa, 10 histological healing has become the focus of growing attention as a more powerful prognostic factor.11–14 The term ‘complete remission’, coined for this condition, has been indicated as a possible new therapeutic target in UC.13–16
Among the drugs able to reduce the risk of recurrence of UC, mesalazine is by far the most frequently used, 5 on the strength of unequivocal demonstrations of its efficacy in maintaining clinical remission. 3 A meta-analysis showed that about 50% of patients with UC with mild-to-moderate active disease treated with mesalazine achieved endoscopic MH, 17 and other observations indicate that, in this condition, a proportion of patients (10–30%) can also achieve histological remission. 11 However, the prognostic relevance of these different depths of remission status, endoscopic and histological, has not been completely clarified.
The present study was conducted to evaluate the prognostic value of histological remission in patients with UC in stable clinical remission on mesalazine, and to compare it with the prognostic value of endoscopic remission.
Materials and method
Study population
This was a single centre cohort study. The study population consisted of consecutive patients with UC under high-dose mesalazine treatment in stable clinical remission, i.e. remission lasting 1 year after a first or second course of steroids. None of the patients had ever used immunosuppressants or biological drugs, and none had changed therapy in the previous year. The high-dose mesalazine regimen consisted of ⩾ 3.6 g/day orally plus 1–4 g/day topically for the first 6 months after steroid withdrawal, and subsequent reduction of the frequency of administration of the topical therapy to 3 times/week. The diagnosis of UC was based on standard clinical, endoscopic and histological criteria. Clinical remission was defined as a partial Mayo endoscopic subscore (MES) < 2. 18 The baseline characteristics, including demographic (age, gender) and clinical (disease duration, extent, clinical course, prior and current medications, smoking habits) data, of each enrolled patient, were recorded.
Baseline assessment
All patients underwent a planned colonoscopy with biopsies after 1 year of stable remission, according to the follow-up procedure adopted at our institution for UC. All patients gave a written consent to the anonymous processing of their data. Ethics approval was waived by the Internal Review Board of the University of L’Aquila since no procedures outside clinical practice were planned. Each patient was given an MES, based on the overall appearance of the colonic mucosa; 18 MES = 0 corresponded to endoscopic remission. Two biopsies were taken from different portions of the colon (i.e. the cecum, ascending colon, transverse colon, descending colon, sigmoid colon and rectum) targeting the areas where the colitis was endoscopically most active. Haematoxylin and eosin-stained slides for pathological examination were retrieved from all the endoscopy biopsies in all the patients. Two pathologists, unaware of the clinical and endoscopic scores, reviewed the biopsies together and jointly scored the histological activity using the histological activity index (HAI) 19 : a score of 0 (inactive colitis) was given to tissue with no epithelial infiltration by neutrophils; a score of 1 (mildly active colitis) was given to tissue with neutrophil infiltration in < 50% of sampled crypts or cross sections, without ulcers or erosions; a score of 2 (moderately active colitis) was given to tissue with neutrophil infiltration in > 50% of crypts, no ulcers or erosions; a score of 3 (severely active colitis) was given to tissue with erosions or ulcerations, irrespective of other features. By convention, the specimen with the worst degree of inflammation was considered to categorize patients, according to the HAI, into four groups, one for each HAI score (0: remission, 1: mild activity, 2: moderate activity, 3: severe activity). HAI, also called the Harpaz index or Gupta index,13,14,19 is a relatively simple index developed and used at Mount Sinai Hospital with high levels of intra-observer and inter-observer agreement with kappa values of approximately 0.9 regardless of the level of training. 20 We decided to use the HAI score as it is mainly based on the presence of neutrophil infiltration, which defines inflammatory activity. 13 Furthermore, HAI score calculation is easy and fast, with apparently few sources of bias.
Inter-rater agreement between histology and endoscopy was analysed by comparing MES and HAI scores since both are indexed from 0 (absence of inflammation) to 3 (the worst inflammatory activity).
Outcomes and follow up
The clinical course was evaluated on the basis of relapses needing steroids, immunomodulators and/or biological drugs, over the course of a 3-year follow up. Patients were seen for clinical assessment every 6 months; otherwise, they were contacted by phone/internet. Clinical evaluation was brought forward if patients reported a relapse of symptoms before the scheduled follow up. Steroids were deemed necessary in the presence of an established UC relapse, with or without endoscopic confirmation, according to the MES. 18 The main objective of this study was to compare clinical course between the groups of patients stratified on the basis of histological score. The clinical course was also compared between patients stratified on the basis of endoscopic score. Finally, the subgroup of patients with endoscopic MH was stratified on the basis of their histological activity, and the clinical course of patients with both endoscopic and histological remission (MES 0 and HAI 0) was compared with the clinical course of those in whom MH was not associated with histological remission (MES 0 and HAI ⩾ 1). A model was also created to evaluate the clinical course according to the definition of remission, i.e. clinical, endoscopic or histological.
Statistical analysis
The chi-square test was used to estimate the association between the categorical variables and outcome. The cumulative proportion of relapse-free survival was estimated by the Kaplan–Meier life-table method on the intention-to-treat principle. In this analysis, we considered the months between baseline and the diagnosis of relapse. The log-rank test was used for the between-groups comparisons.
A logistic regression analysis 21 allowed us to estimate the predictive ability of variables for clinical relapse in univariate models, where the dependent variable was the relapse and the independent variable was, for each model, histological activity, endoscopic activity and the baseline characteristics. Logistic regression estimates the probability of relapse for each patient at the value of the independent variables. For logistic analysis histological activity and endoscopic activity were dichotomized (respectively, HAI/MES 0 versus ⩾ 1), age and disease duration were logarithmically transformed, while gender, clinical course, extent and smoking habits were considered categorical variables. The significance of the independent variable in each model was tested with G-test statistics, that, under the hypothesis that b1 is equal to 0, follow a chi-square distribution. 21 On the basis of results of univariate analyses, a multivariate regression analysis was performed. 22 Logistic regression analysis was performed by the LOGISTIC procedure of the SAS statistical software. This provides an approximation that allows the reduction of the bias to obtain the estimated probability of postoperative failure by replacing the logistic regression variables derived from the same set of data. Discrimination between individuals with and without relapse was evaluated by receiver operating characteristic (ROC) analysis. The area under the ROC curve indicates the probability of concordance between the predicted probability of relapse and the actual state, and it has been described as the best ‘index of detectability’. 23 The area ranges from 0.5 for chance performance to 1 for a perfect prediction. Every area referring to a predictive model (and its confidence interval [CI]) was estimated and compared with one another using the method proposed by Hanley and McNeil. 24 The correlation between histological and endoscopic scores was analysed by Spearman’s rank correlation coefficient (p). All statistical analyses were performed using the SAS 9.4 statistics software package.
Results
Study population and baseline assessment
A total of 52 patients with UC were enrolled in the study. The baseline demographic, clinical, endoscopic and histological characteristics of all the patients are shown in Table 1. In particular, all the patients had been in clinical remission for 1 year under treatment with mesalazine, about half (29 patients; 55.77%) had no endoscopic lesions (MES = 0) and one third (17 patients; 32.69%) showed no histological alteration (HAI = 0).
Baseline demographic and clinical characteristics of the cohort of patients with ulcerative colitis in clinical remission. Relapses were categorized as frequent (⩾ 2 relapses/year) or infrequent (⩽ 1 /year). 2

SD, standard deviation.
Table 2 shows the correlation between HAI and MES scores. Spearman’s p was: 0.610 (p < 0.0001), indicating a good correlation.
Correlation between the histological activity index and Mayo endoscopic subscore.
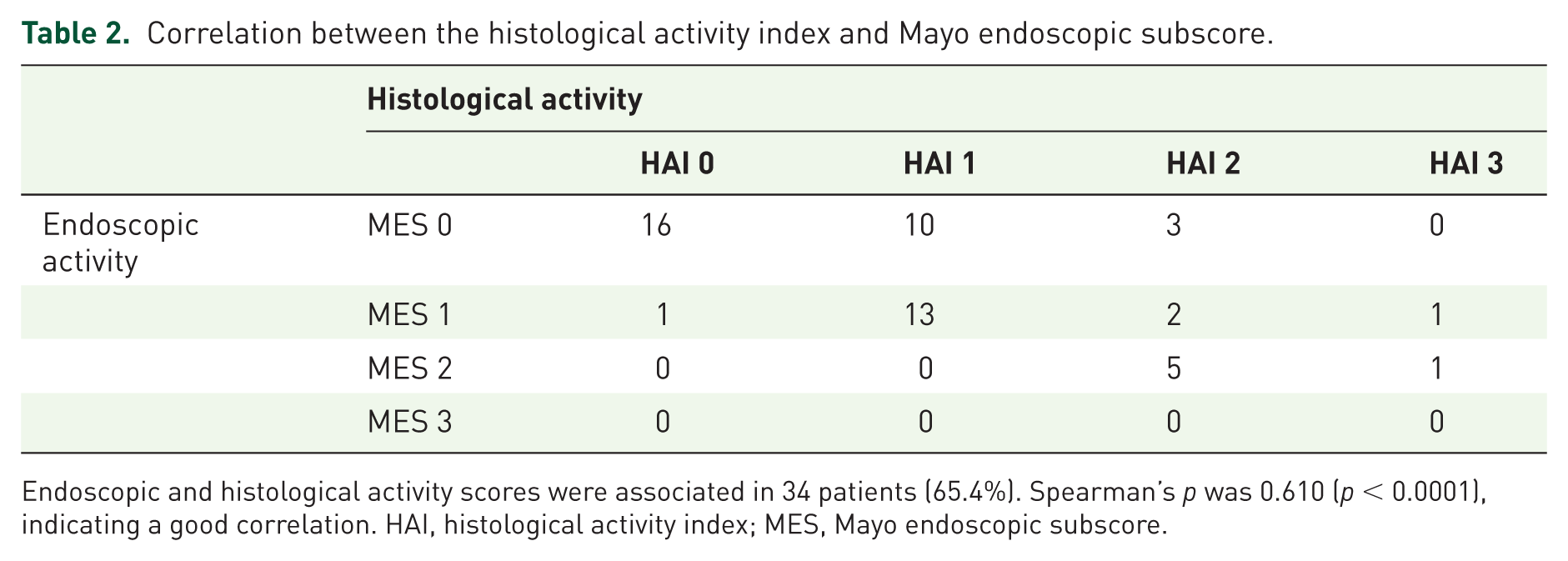
Endoscopic and histological activity scores were associated in 34 patients (65.4%). Spearman’s p was 0.610 (p < 0.0001), indicating a good correlation. HAI, histological activity index; MES, Mayo endoscopic subscore.
Outcome
At 3 years of follow up, overall, 26 patients (50%) were still in steroid-free remission. In patients with HAI scores at baseline of 0, 1, 2 and 3, clinical remission rates were 88.24%, 47.83%, 0% and 0%, respectively. For subsequent evaluations, patients with moderate and severe histological activity (HAI 2 and 3), due to their small numbers, were considered as a single group for statistical analysis. The remission rates of patients with MES scores of 0, 1 and 2 (none had a score of 3), were 68.97%, 35.29% and 0%, respectively.
Histology
The cumulative proportion of relapse-free survival at 36 months of follow up differed significantly (p < 0.0001) between the three groups of patients (HAI 0 versus 1 versus ⩾ 2). A better relapse-free survival was predicted by histological remission (Figure 1). The patients with mild histological activity (HAI 1) and those with moderate-to-severe activity (HAI 2 and 3) showed a relapse risk that was 5.62 (95% CI: 2.48–12.72) and 22.68 (95% CI: 6.28–81.84) times higher, respectively, than that of the patients in histological remission (HAI 0).

Kaplan–Meier life-table curves of survival free of relapse needing steroids. Patients were stratified on the basis of histological activity into three groups: histological activity index (HAI) 0, HAI 1 and HAI ⩾ 2. The numbers of patients in each group are reported.
Endoscopy
The cumulative proportion of relapse-free survival at 36 months of follow up differed significantly (p < 0.0001) between the three groups of patients (MES 0 versus 1 versus 2). A better relapse-free survival was predicted by endoscopic remission (Figure 2). Patients with mild endoscopic activity (MES 1) and those with moderate activity (MES 2) showed a relapse risk that was 2.86 (95% CI: 1.22–6.71) and 15.74 (95% CI: 1.56–158.90) times higher, respectively, than those in endoscopic remission (MES 0).

Kaplan–Meier life-table curves of survival free of relapse needing steroids. Patients were stratified on the basis of endoscopic activity into three groups: Mayo endoscopic subscore (MES) 0, MES 1 and MES 2. The numbers of patients in each group are reported. Time is expressed in months.
Comparison between histological, endoscopic and clinical remission
A total of 29 patients showed MH (MES 0) at baseline. Of these, 16 had both normal endoscopy and normal histology (MES 0 and HAI 0), while the remaining 13 presented histological activity (MES 0 and HAI ⩾ 1). The cumulative proportion of relapse-free survival at 36 months of follow up was significantly better in patients showing histological remission (p < 0.01) than in those with microscopic inflammation of any grade of activity (Figure 3). Patients with histological activity showed a relapse risk 5.52 (95% CI: 1.44–21.11) times higher than those with histological remission.
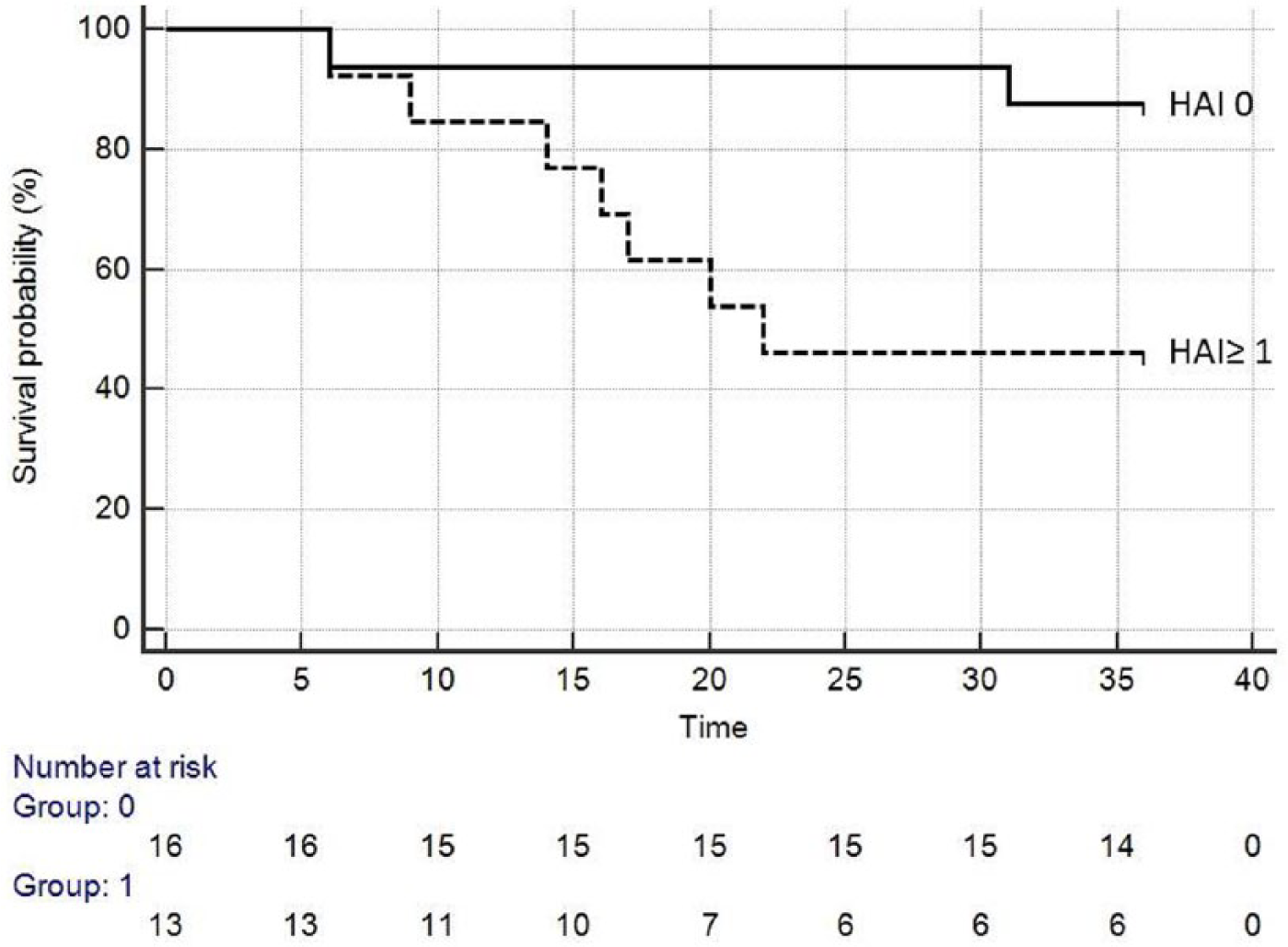
Kaplan–Meier life-table curves of survival free of relapse needing steroids in the subgroup of patients with endoscopic remission (Mayo endoscopic subscore 0). Patients were substratified on the basis of histological activity; histological activity index (HAI) 0 versus HAI ⩾ 1). The numbers of patients in each group are reported. Time is expressed in months.
Finally, the probability of avoiding steroids over the 3-year follow up in patients with clinical, endoscopic and histological remission, considered separately, was 50.0%, 69.0% and 88.2%, respectively (Figure 4). Histological remission, when compared with clinical and endoscopic remission, was associated with a significantly better outcome (p < 0.008).

Evaluation of the clinical course according to the definition of remission at baseline, i.e. clinical, endoscopic or histological. Time is expressed in months.
Regression logistic analysis
The results of the univariate logistic regression analysis (Table 3) showed a significant relationship between the risk of relapse and both histological activity (G statistics: 16.198, p = 0.0001; odds ratio [OR]: 16.364; 95% CI: 3.178–84.270) and endoscopic activity (G statistics: 9.761, p: 0.0018; OR: 6.296; 95% CI: 1.861–21.299). There were no significant relationships bet-ween the risk of relapse and other baseline characteristics.
Comparison of the results of the univariate and multivariate logistic regression analysis for the prediction of relapse.
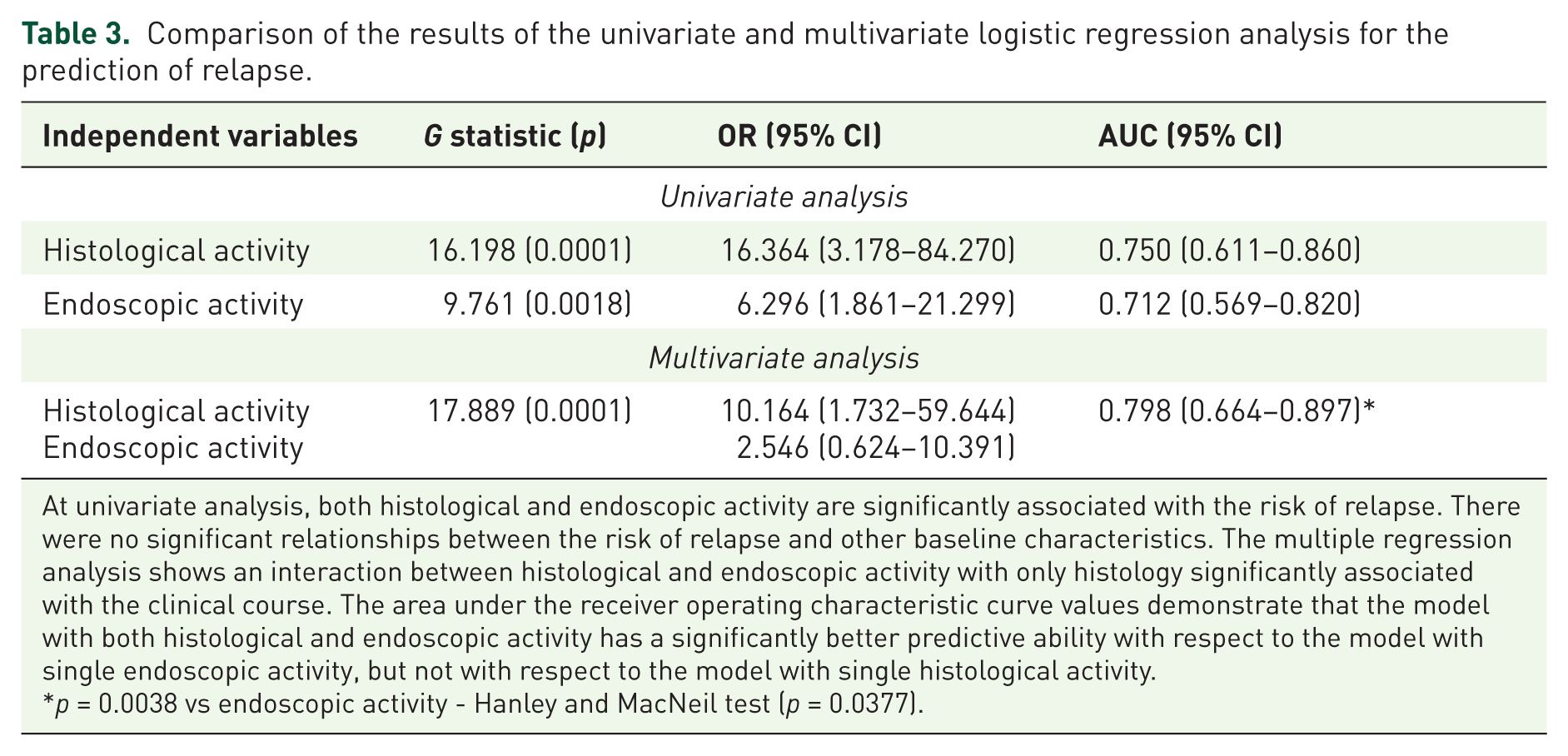
At univariate analysis, both histological and endoscopic activity are significantly associated with the risk of relapse. There were no significant relationships between the risk of relapse and other baseline characteristics. The multiple regression analysis shows an interaction between histological and endoscopic activity with only histology significantly associated with the clinical course. The area under the receiver operating characteristic curve values demonstrate that the model with both histological and endoscopic activity has a significantly better predictive ability with respect to the model with single endoscopic activity, but not with respect to the model with single histological activity.
p = 0.0038 vs endoscopic activity - Hanley and MacNeil test (p = 0.0377).
Multiple logistic regression analysis revealed an interaction between histological and endoscopic activity and only histology continued to be significantly associated with the clinical course (OR: 10.164; 95% CI: 1.732–59.644; OR: 2.546; 95% CI: 0.624–10.391, respectively). No other variable determined significant interactions with respect to histological activity in the prediction of relapse. The model with both histological and endoscopic activity had a significantly better predictive ability with respect to the model with single endoscopic activity, but not with respect to the model with single histological activity as demonstrated by the area under the ROC curve values (Table 3).
Discussion
The need to combat inflammation in UC became apparent more than a century ago when it was reported that the inflammatory process involving the colonic mucosa is responsible for the disease’s signs, symptoms and complications, including colorectal cancer.25–27 Since then, numerous studies have attempted to identify the best outcome we can expect from an anti-inflammatory drug. Clinical response and maintenance of remission have traditionally been considered the best result of therapy in UC.1,28,29 In the last few years, however, the bar has been raised: the outcome now pursued is MH, as this condition, compared with clinical remission, is associated with a lower risk of recurrence and complications.8,9,30–32 Although the clearest demonstration has been obtained with biological drugs, even traditional medications have been shown to achieve MH.8,9,17 As a result, it is now claimed that MH should be the main outcome of future controlled clinical trials.12–14 The still debated role of histological inflammation in predicting recurrence has recently been studied in two cohorts of patients with different clinical course and treatment.15,16 The first study included 91 patients with UC (37 in clinical remission) submitted to different therapies (i.e. mesalazine, azathioprine, anti-tumour necrosis factor [TNF]-α and no treatment at all), followed up for a median of 72 months. Histological remission (Truelove and Richards’ index) was shown to be of more value than endoscopic remission (Baron score) in predicting the requirement for corticosteroids or hospitalization. 15 Another study investigated a cohort of 179 patients with UC, all in clinical remission, treated with different therapies (i.e. mesalazine, thiopurines, anti-TNF-α), and followed up for 12 months. Histological remission at baseline (Geboes score) was the only independent factor associated with clinical relapse. 16 In spite of these results, an international steering committee on therapeutic targets in inflammatory bowel disease stated that the level of evidence is insufficient to recommend histological remission as a target in UC in clinical practice. 33
To provide further data on this topic, the present investigation was conducted to evaluate the prognostic value of histology in a homogeneous cohort of patients with a similar clinical course and same therapeutic regimen (mesalazine), representing patients in the early phases of a step-up therapeutic approach. Mesalazine was given at doses usually considered high but, at the same time, able to assure a higher drug therapeutic concentration at the site of inflammation. In this setting, results showed that, although there was a good correlation between histological and endoscopic scores, at multivariate analysis only histology significantly predicts the outcome.
The finding that patients who are better are more likely to get better in the future may seem obvious. However, it is not clear why patients in clinical remission following the same therapeutic regimen have different degrees of microscopic inflammation. A hypothesis is that patients with lower histological activity suffer from less aggressive disease. Different clinical courses have been recognized in patients with UC,4,5 but relevant prognostic factors able to predict which patients are most likely to suffer from more aggressive disease are lacking. The treatment of UC is based on standardized therapeutic indications derived from clinical trials. 3 Patients in clinical remission are strictly monitored in order to intervene promptly when a clinical recurrence ensues. 2 However, since symptoms occur when mucosal inflammation has already flared up, our therapeutic intervention is always late. Thus, the availability of a parameter that could identify which patients are most likely to undergo recurrence would be useful in planning tailored follow up and therapies. The results of the present study show that the risk of recurrence in patients with any grade of histological inflammation is significantly higher than in patients with histological remission. Moreover, the greater the severity of inflammation, the worse the prognosis was over a 3-year follow up. Even endoscopy seems able to predict recurrence better than clinical status, but the only independent prognostic variable is histological inflammation.
Several definitions of histological remission in UC have been proposed, but the most appropriate has yet to be established. 33 Out of the numerous scores that, starting from 1956 (Truelove and Richards index), have been developed to measure histological activity, none has been fully validated.12–14 Currently, the most widely used histological indices of disease activity in UC are the Riley index (1991) and the Geboes index (2000). These two scores have many similarities as they grade features of both acute and chronic inflammation. 34 Many other indices evaluate only features of acute inflammation,14,34,35 in particular neutrophils, as they are considered to play the leading role in acute inflammation. 13 Experts agree that neutrophils are a key component for diagnosing the presence of active disease or MH. 36 Assessment of neutrophils has a higher reproducibility with respect to other items of acute inflammation, and could easily generate agreement between pathologists more than other features associated with disease activity.36,37 In the present study, we used the partially validated HAI that is based just on the evaluation of neutrophils. It is a stepwise grading system, easy and fast to calculate, with high levels of intra-observer and inter-observer agreement (kappa values of approximately 0.9), and therefore suitable for clinical practice.19,20 It has been observed that evaluation of HAI has a good agreement regardless of the level of pathologist training. 20 Therefore, this score could allow a precise measure of histological remission in the real clinical practice even when obtained by nondedicated pathologists. The HAI score has a good correlation with the need for colectomy and development of colorectal cancer in UC.19,38 By means of the HAI score, we further confirmed the prognostic value of histology already described in other series using different indices.15,16 Therefore, a regular endoscopic and histological follow up in patients with UC should be employed, not only to detect dysplasia, but also to establish more precisely the patient’s remission status in order to modulate therapy, a strategy that has recently been successfully adopted in Crohn’s disease. 39 Thus, in our opinion, in patients showing microscopic inflammation in spite of clinical and endoscopic remission, a risk–benefit ratio should be considered in order to decide the opportuneness of a step up of treatment to obtain MH.
In conclusion, the present study demonstrates that in patients treated with high doses of mesalazine in clinical remission for 1 year, the absence of histological inflammation carries a lower risk of recurrence than the presence of inflammatory infiltration of any severity. Another result is that endoscopic appearance is less effective than histology in predicting the outcome, while the worst prognostic factor is clinical remission, the factor that both patients and physicians currently consider the main target when treating this disease. It remains to be clarified whether these observations might drive the decision to step up therapy before clinical recurrence ensues.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest.