
Abstract
Background:
The objective of this study was to report a case series on the efficacy and safety of capecitabine 7/7 schedule combined with erlotinib (CAP-ERL) in patients with advanced pancreatic cancer (APC) who have failed prior therapies.
Methods:
We retrospectively evaluated 13 patients with locally advanced or metastatic pancreatic cancer previously treated with gemcitabine or oxaliplatin–irinotecan-based first-line regimens. Treatment consisted of capecitabine (Xeloda) at a flat dose of 1000 mg orally twice daily on days 1–7 out of 14 days (7/7 schedule) and erlotinib (Tarceva) 100 mg orally once daily until unacceptable toxicity or disease progression. Tumor assessments were repeated every two cycles (8 weeks) and serum tumor markers were measured every 4 weeks.
Results:
All patients (median age: 63 years; 7 female/3 male) had various previous lines of treatments of chemotherapies. Median number of cycles with CAP-ERL was 4 (range 2–12). The overall response rate was 20%. CA19-9 was reduced more than 25% in 40% patients. The median overall survival and progression-free survival from the start of CAP-ERL were 4.5 months (range 3–7.5) and 2 months (range 1.5–4), respectively. The most common grade 3 toxicities included hand–foot syndrome, nausea, vomiting, diarrhea, rash, and fatigue.
Conclusions:
Our result suggests that the combination of a fixed low dose of CAP-ERL 7/7 schedule was tolerated with manageable toxicity and showed encouraging activity as salvage treatment in patients with refractory APC with ECOG performance status 0–2. Further prospective studies are warranted to evaluate this combination.
Introduction
Pancreatic adenocarcinoma is one of the most lethal cancers with mortality accounting for 6% of all cancer-related deaths, listed just after lung, prostate, breast, and colorectal cancer (CRC) [Saif, 2014]. Most pancreatic cancers are diagnosed in the latter stages with local invasion or metastasis. These cancers are not surgically removable and have to be treated with chemotherapy or radiotherapy. However, the treatment outcomes are not satisfactory due to drug resistance; either inherent or acquired drug resistance. There is growing evidence that supports the benefit of chemotherapy after gemcitabine failure in selected patients with good performance status [Kang and Saif, 2008].
To date, the US Food and Drug Administration (FDA) has approved nonstandard regimen for salvage chemotherapy after gemcitabine failure in patients with advanced pancreatic cancer (APC). However, data exists for OFF (oxaliplatin, folinic acid, 5-FU) in these patients and many other small phase II studies have shown activity of single as well as combined regimens [Kang and Saif, 2008; Oettle et al. 2005]. Capecitabine has been investigated prospectively by Boeck and colleagues in 37 patients with APC who already had received at least one previous treatment regimen containing full-dose gemcitabine either as single or combination chemotherapy or sequentially within a radiochemotherapy with capecitabine [Boeck et al. 2007]. Capecitabine was administrated orally at a daily dose of 2 × 1250 mg/m2 for 14 consecutive days followed by 7 days of rest and dose reduction in patients >65 years to 1000 mg/m2/day. They reported stable disease (SD) in 37% of patients and a decrease in CA19-9 of more than 20% in 16% of patients. Median time to tumor progression (TTP) was 2.2 months and median overall survival (OS) was 7.5 months. Most common grade ⩾2 toxicities included hand–foot syndrome (HFS) in 30%, anemia in 24%, diarrhea in 14%, nausea/vomiting in 11%, and leukopenia in 11%. On the other hand, erlotinib, an oral epidermal growth factor receptor (EGFR) tyrosine kinase inhibitor (TKI) was approved in combination with gemcitabine for use in first-line treatment of APC in 2005 [Moore et al. 2007]. This study showed a mild benefit in survival, approximately 12–14 days of gain with erlotinib therapy. Investigators also evaluated erlotinib in the second line in APC as a single agent at a dose of 150 mg per day orally in 13 patients with APC [Epelbaum et al. 2007]. Median TTP was only 1 month and five patients achieved clinical improvement with either SD or decrease in CA19-9.
Preclinical data led clinical investigators to investigate the benefit of combining capecitabine and erlotinib (CAP-ERL). Kaori and colleagues administered erlotinib 100 mg/kg/day with or without capecitabine 359 or 90 mg/kg/day, by oral administration once daily for 14 days in BALB/c nu/nu mice bearing LoVo and HT-29 (colon cancer), A-431 (vulvar cancer), and KPL-4 and MAXF401 (breast cancer) human tumors [Kaori et al. 2006]. They observed that erlotinib inhibited tumor growth in a range of human tumor xenograft models, including breast cancer and CRC. CAP-ERL demonstrated at least additive activity in LoVo, KPL-4, and A-431 tumor models. The antitumor activity of the combination was greater than that of capecitabine alone at the MTD. Erlotinib treatment did affect thymidine phosphorylase (TP) in the CRC tumor models. This preclinical data was further supported by a study that treated 30 patients with gemcitabine-refractory APC with capecitabine 1000 mg/m2 twice daily for 2 weeks, followed by a 1-week break along with erlotinib 150 mg daily [Kulke et al. 2007]. This CAP-ERL regimen resulted in an overall objective radiologic response rate (RR) of 10%, median OS of 6.5 months, reduction in CA19-9 of more than 50% in 17% of the patients. Common toxicities included diarrhea, skin rash, fatigue, and HFS.
However, capecitabine is rarely tolerated at the recommended dose in the US population, especially in patients with APC [Saif et al. 2008a]. Moreover, erlotinib was planned to be escalated to 150 mg in the Moore and colleagues study but due to toxicity 100 mg was the dose approved by FDA [Moore et al. 2007]. In addition, rash has been found to be a surrogate maker for response to erlotinib and small efforts have been conducted to escalate erlotinib to cause rash to achieve response [Saif et al. 2008b; Renouf et al. 2014]. We already know from previous studies that the RR of 5-FU is directly proportional to the area under the curve (AUC) and hence increasing the dose may achieve a better outcome [Saif and von Borstel, 2006]. These rationales allowed us to treat patients with APC on a novel schedule that had previous treatment with various chemotherapeutic agents and radiotherapy.
Patients and methods
We conducted a retrospective chart review of patients with APC. We selected patients with APC who have failed the first-line and more upfront chemotherapy regimens, including gemcitabine-containing regimens during March 2009 to April 2013. A pharmacy database was created to indicate patients for who were treated with CAP-ERL during this period. A review of electronic charts was performed. The data including age, sex, diagnoses, dose of CAP-ERL, laboratory data including CA19-9 and CT scan results were collected.
Patients received capecitabine at a flat dose of 1000 mg orally twice daily on days 1–7 out of 14 days (7/7 schedule) and erlotinib (Tarceva) 100 mg PO daily. As rationalized above [Saif et al. 2008b; Renouf et al. 2014], if no rash developed, erlotinib was escalated to 150 mg and continued if no toxicity was found. If the tumor marker rose, then capecitabine was escalated to 1300 mg twice daily, 1500 mg twice daily and 2000 mg twice daily based on the data described above [Saif and von Borstel 2006]. The side effects of the combination treatment were closely monitored and the dosage of erlotinib and capecitabine were modified when the side effects reached severe as per general guidelines for both agents, including management of rash and HFS.
Imaging was performed every four cycles (8 weeks), and serum CA19-9 was measured every 4 weeks. Response to treatment was assessed using Response Evaluation Criteria in Solid Tumors (RECIST) parameters. The best response seen at either 8 weeks or 16 weeks was considered. CA19-9 response was defined as drop of at least 25% from baseline at the time of start of CAP-ERL. Toxicity was graded using the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE), version 3.0. Progression-free survival was defined as time from initiation of treatment until disease progression or death. OS was defined as time from initiation of treatment until death or last known follow up.
Results
Demographic features
A total of 13 patients were included in this retrospective review. Data from 10 patients are included in this report as one patient only received the first three doses and declined to continue and the other two patients were lost to follow up as they initially came for second opinion only. The demographic characteristics of the patients are listed in Table 1. Among these patients, seven were female and three were male. Ages ranged from 48 to 71 years (median age: 63). All patients had advanced (stage IV) stage. All patients had various previous treatments of chemotherapies (Table 1). Among them, four patients had radiotherapy as well with concomitant capecitabine as a radiosensitizer. Chemotherapies included gemcitabine-based regimens in nine patients. Other cytotoxic agents exposed to these patients before received CAP-ERL included: 5-FU-based combination therapy with oxaliplatin (FOLFOX; FLOX), irinotecan (FOLFIRI) and all of them (FOLFIRINOX). Three patients started initially with gemcitabine alone and two of these later received gemcitabine combined with other agents after improvement in PS or test of the tolerability. One patient received gemcitabine combined with an oral hedgehog inhibitor (IPI-926) on a clinical study while four patients received gemcitabine doublet with platinum or a taxane. One patient received FOLFIRINOX as first-line therapy and later gemcitabine alone as second-line therapy. Four patients had also received FOLFOX and/or FOLFIRI after failing gemcitabine before they received CAP-ERL on our study. In summary, all of the patients had at least two lines of prior chemotherapy (three had three prior therapies and two had three prior therapies including capecitabine as a radiosensitizer with external beam radiation) except one who received one line of chemotherapy (GTX).
Summary of demographic characteristics of the study population.

ECOG, Eastern Cooperative Oncology Group; PS, performance status; G, gemcitabine; GEMOX, gemcitabine and oxaliplatin; GEM-CIS, gemcitabine and cisplatin; FOLFOX, folinic acid, 5-FU, and oxaliplatin; FOLFIRI, folinic acid, 5-FU, and irinotecan; GTX, gemcitabine, docetaxel, and capecitabine; GT, gemcitabine and docetaxel; FOLFIRINOX, folinic acid, 5-FU, irinotecan, and oxaliplatin.
Dose intensity
Median number of cycles with CAP-ERL was 4 (range 2–12).
Efficacy
The overall response rate was 20%. Two patients achieved partial response (PR) at second restaging scans at 16 weeks after their dose of erlotinib and capecitabine escalated, respectively (Table 2). One of two PRs was observed in a patient who only received prior systemic chemotherapy and the second patient had received radiotherapy as well. Four patients achieved SD at the end of 8 weeks or 16 weeks as their best responses on restaging CT scan or MRI. The overall disease control rate was 60%. However, there were no complete responses. CA19-9 was reduced by at least 25% in four patients, stable in three and increased in another three patients.
Summary of treatment and efficacy on capecitabine 7/7 plus erlotinib schedule.
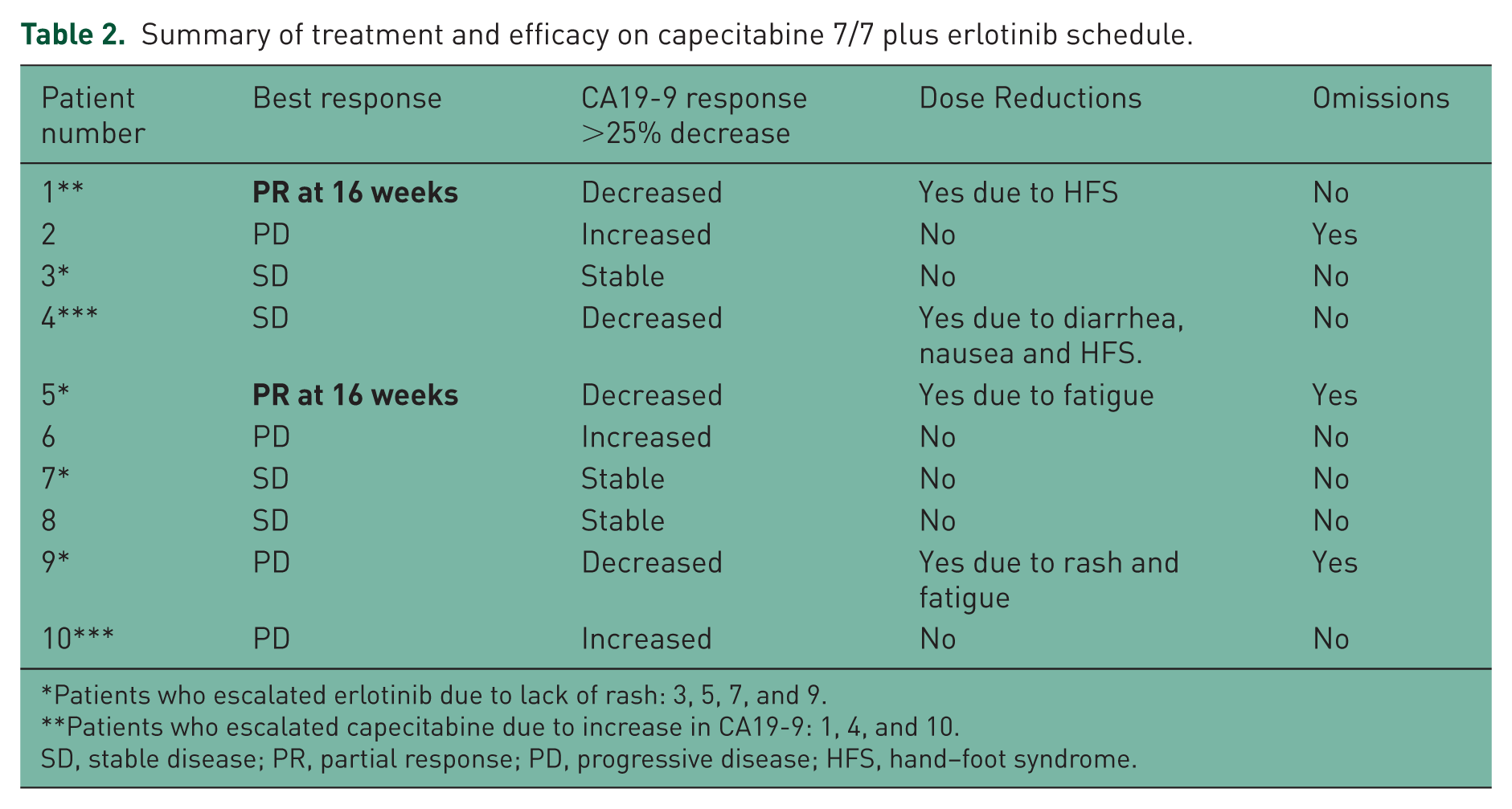
Patients who escalated erlotinib due to lack of rash: 3, 5, 7, and 9.
Patients who escalated capecitabine due to increase in CA19-9: 1, 4, and 10.
SD, stable disease; PR, partial response; PD, progressive disease; HFS, hand–foot syndrome.
Toxicity
The most common toxicities were mild (grade 1 or 2) consisting of rash, paronychia, diarrhea, nausea, vomiting, fatigue, anorexia, trichomegaly, hypomagnesaemia, and hyperbilirubinemia (Table 3). Grade 3 toxicities included HFS, nausea, vomiting, diarrhea, rash, and fatigue. None of these patients had grade 4 side effects, indicating that the treatment regimen was well tolerated. Due to severe side effects, only four patients had dose reduction. However, there were no patients withdrawn from the study except one who was included in this case series.
Summary of grade 1–4 toxicities observed on capecitabine 7/7 and erlotinib schedule.
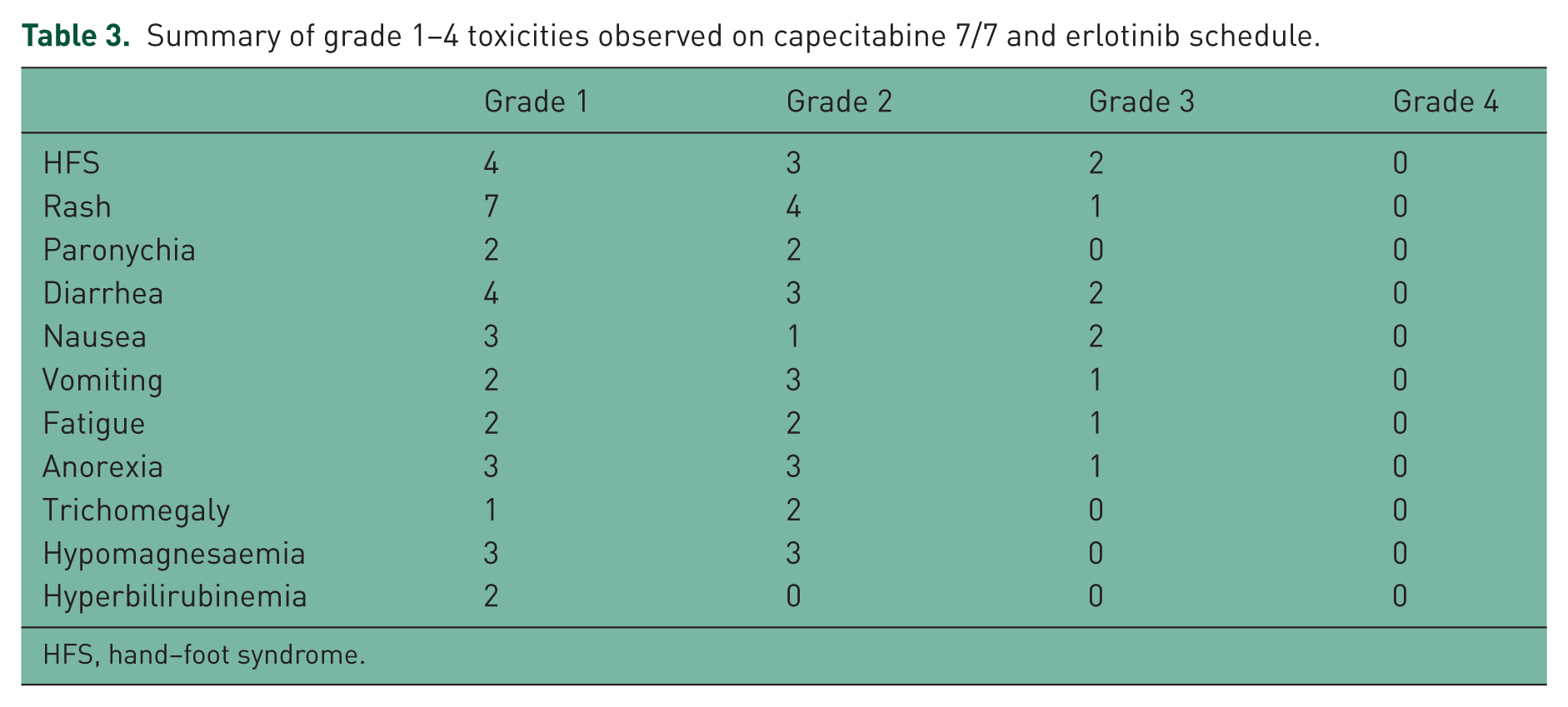
HFS, hand–foot syndrome.
Dose of capecitabine was increased in three patients (1, 4, and 10) to 1300 mg orally twice daily and then 1500 mg twice daily: two patients tolerated the 1500 mg dose level with no added toxicity while the third patient was not able tolerate and hence reduced back to 1000 mg due to diarrhea and HFS. The first two patients who tolerated dose escalation had PR in one and SD in the other. Both had decreased CA19-9.
Erlotinib was only escalated in four patients (3, 5, 7, and 9) and only two of them were able to tolerate the 150 mg dose level and developed rash with favorable outcome both with decrease in CA19-9 (33%) and SD while the other two did not tolerated due to diarrhea and fatigue. Although 1 of these two had SD as his best response.
Survival
The overall response rate was 20%. CA19-9 was reduced by more than 25% in 40% of patients. The median OS and progression-free survival from the start of CAP-ERL were 4.5 months (range 3–7.5) and 2 months (range 1.5–4), respectively. At the time of data collection (46 weeks from the first patient), the 3-month survival rate was 70% (7/10), 6-month survival was 30% (3/10), and 1-year survival rate was 10% (1/10).
Discussion
As EGFR is frequently activated in pancreatic cancer (PC), targeted therapy against EGFR has been used in combination with chemotherapeutic agents [Saif, 2014; Kang and Saif, 2008; Moore et al. 2007; Epelbaum et al. 2007]. EGFR inhibitor erlotinib has been studied in several clinical trials in both untreated patients. It has also been tested in patients previously treated with gemcitabine. In these studies, erlotinib produced modest response while dosage escalation was limited by its side effects. In the present study, we employed a novel schedule of 7/7 capecitabine and escalating doses of erlotinib in 13 patients who had previous treatment with various chemotherapeutic agents including gemcitabine, 5-FU and oxaliplatin, and radiotherapy. A majority of the patients had a response or decrease in CA19-9. Although the number of patients in this case series is small, it does provide a rationale to test a novel and comparatively more tolerable combination of erlotinib and capecitabine in patients with refractory PC.
Our regimen was based on many facts such as the following.
Capecitabine is rarely tolerated at the recommended dose in USA population, especially in patients with APC [Saif et al. 2008a].
Erlotinib was planned to be escalated to 150 mg in the Moore study but due to toxicity 100 mg was the dose approved by FDA [Moore et al. 2007].
Rash has been found to be a surrogate maker for response to erlotinib [Saif et al. 2008b].
Efforts have been conducted to escalate erlotinib alone or in combination with gemcitabine to cause rash to achieve response but results were not consistent [Renouf et al. 2014].
RR of 5-FU is directly proportional to AUC and hence increasing the dose may achieve a better outcome [Saif and von Borstel, 2006].
The dose of capecitabine was increased in three patients to 1300 mg orally twice day and then 1500 mg twice daily: two patients tolerated the 1500 mg dose level with no added toxicity while the third patient was not able tolerate and hence the dose was reduced back to 1000 mg. The first two patients who tolerated dose escalation had PR in one and SD in the other. Both had decreased CA19-9. Both patients developed grade 2 HFS. Erlotinib was only escalated in four patients and 1 of them PR and 2 SD with decrease in CA19-9 as well (Table 3).
Recently the impact of HFS on outcome in patients receiving CAP-ERL was published [Kruger et al. 2015]. A total of 281 patients were randomized patients in a multicenter phase III study (AIO-PK0104) to first-line treatment with either capecitabine plus erlotinib (150 mg/day, arm A) or gemcitabine plus erlotinib (150 mg/day, arm B). A crossover to either gemcitabine (arm A) or capecitabine (arm B) was undertaken if the first-line treatment failed. They found that time to treatment failure after first- and second-line therapy (TTF2) and OS both were significantly prolonged for the 44 patients (44%) with HFS compared with 57 patients without HFS (56%) (TTF2 7.8 versus 3.8 months, HR 0.50,p = 0.001; OS 10.4 versus 5.9 months, HR 0.55, p = 0.005). They concluded that HFS may serve as an independent clinical predictor of benefit from capecitabine in patients with APC. Our two patients who received increasing doses of capecitabine did develop grade 2 HFS and both showed clinical benefit as described earlier.
Recent literature also contains a single-arm phase II study of CAP-ERL in first-line treatment of PC (XELTA trial) [Lopez et al. 2013]. In this study, 32 patients with APC received capecitabine at 1,000 mg/m2 twice daily on days 1-14, of a 21-day treatment cycle and oral erlotinib at 150 mg daily. The overall RR was 6%, median TTF of 2.1 months, median progression-free survival of 2.1 months and median OS was 4.3 months. The 1-year survival rate was 22%. Influenced by the underlying science and oral convenience, other investigators have also tested CAP-ERL in combination with concurrent radiation therapy in patients with PC [Ma et al. 2010]. A total of 13 patients with resected PC were administered erlotinib in doses from 150 mg orally daily to a lower dose of 100 mg if not tolerated and capecitabine at fixed doses of 800 mg/m2 twice daily Monday to Friday concurrently with IMRT delivered at 1.8 Gy daily in 28 fractions (total of 50.4 Gy). They concluded that erlotinib 100 mg daily and capecitabine 800 mg/m2 twice daily (Monday to Friday) with concurrent IMRT can be administered safely in resected PC patients, again indicating the paucity of data due to a lower number of patients as well as tolerability of higher doses of erlotinib when combined with capecitabine.
One may ask about the selection of doses of CAP-ERL in our study. We chose a fixed dose and low doses of both agents as almost all of our patients had received at least two lines of prior chemotherapy, hence these were receiving CAP-ERL as a third-line or in some fourth-line treatment option, and also due to their performance status related to the cancer. There is limited data on this combination oral chemotherapy regimen in second-line therapy of APC. Only one study as mentioned earlier treated 30 patients with gemcitabine-refractory disease resulting in overall response rate of 10%, median OS of 6.5 months and more than 50% drop in CA19-9 in 17% of patients [Kulke et al. 2007]. Therefore, no comparison can be made as the patient populations are different and hence the tolerance and outcomes differ too.
In summary, our unique dosing of CAP-ERL resulted in a well-tolerated oral regimen in this case series. Although the number of patients in this study is small, it triggers interest for future studies. Future prospective trials should assess the novel schedule of this regimen.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.