
Abstract
Pancreatoblastoma (PB) is a rare epithelial malignancy usually occurring in the paediatric population. Adult PB is rare, and its imaging findings are similar to those of other tumours, making preoperative diagnosis a considerable challenge. We report correlative ultrasound, contrast-enhanced ultrasonography, contrast-enhanced magnetic resonance imaging, and positron emission tomography-computed tomography findings in a 60-year-old woman with PB. PB often presents with uncommon imaging features and should be considered in the differential diagnosis of pancreatic masses. It is important for clinicians to be aware of these differences to provide effective treatment.
Introduction
Pancreatoblastoma (PB) is known as infantile carcinoma of the pancreas. 1 This rare epithelial tumour is often misdiagnosed as neuroblastoma or hepatoblastoma. 2 It has mainly been reported in children with few cases in the adult population. 3 Here, we report a rare case of adult PB and discuss the imaging, clinicopathological features, and treatment modalities.
Case presentation
A 60-year-old woman presented with fatigue for half a year. She was examined and found to have a mass in the tail of the pancreas; thus, she was admitted to our hospital. The reporting of this case conforms to the CARE guidelines. 4
Laboratory tests identified elevated cancer antigen (CA)19-9 levels (492.6 U/mL, normal value: 0.0–37.0 U/mL), CA-125 levels (111.5 U/mL, normal value: 0.0–35.0 U/mL), cytokeratin (CK) 19 levels (4.7 ng/mL, normal value: 0.0–3.8 ng/mL), and neuron-specific enolase levels (26.3 ng/mL, normal value: 0.0–16.3 ng/mL). However, carcinoembryonic antigen (CEA) and α-fetoprotein (AFP) levels were within the normal ranges.
Abdominal ultrasound showed that the pancreatic body and tail were enlarged and demonstrated a 59- × 25-mm round lesion with clear boundaries and a regular shape near the splenic vein (Figure 1a). Otherwise, the pancreas was normal. The ultrasound also identified a 5- × 13-mm round lesion located in the right side of the liver (Figure 1b).

Ultrasound imaging of the 60-year-old patient reported in this case. (a) A hypoechoic mass was found in the pancreatic body and tail. (b) A hypoechoic mass was found in the right liver.
Contrast-enhanced ultrasonography showed equal enhancement in the arterial phase of the pancreatic lesion, with slightly faster withdrawal in the delayed phase (Figure 2a). This result suggested that the lesion had a rich blood supply, which was consistent with a neuroendocrine tumour. There was rapid and high enhancement in the arterial phase of the right liver lesion and low enhancement in the portal venous and delayed phases (Figure 2b), consistent with a metastatic tumour.
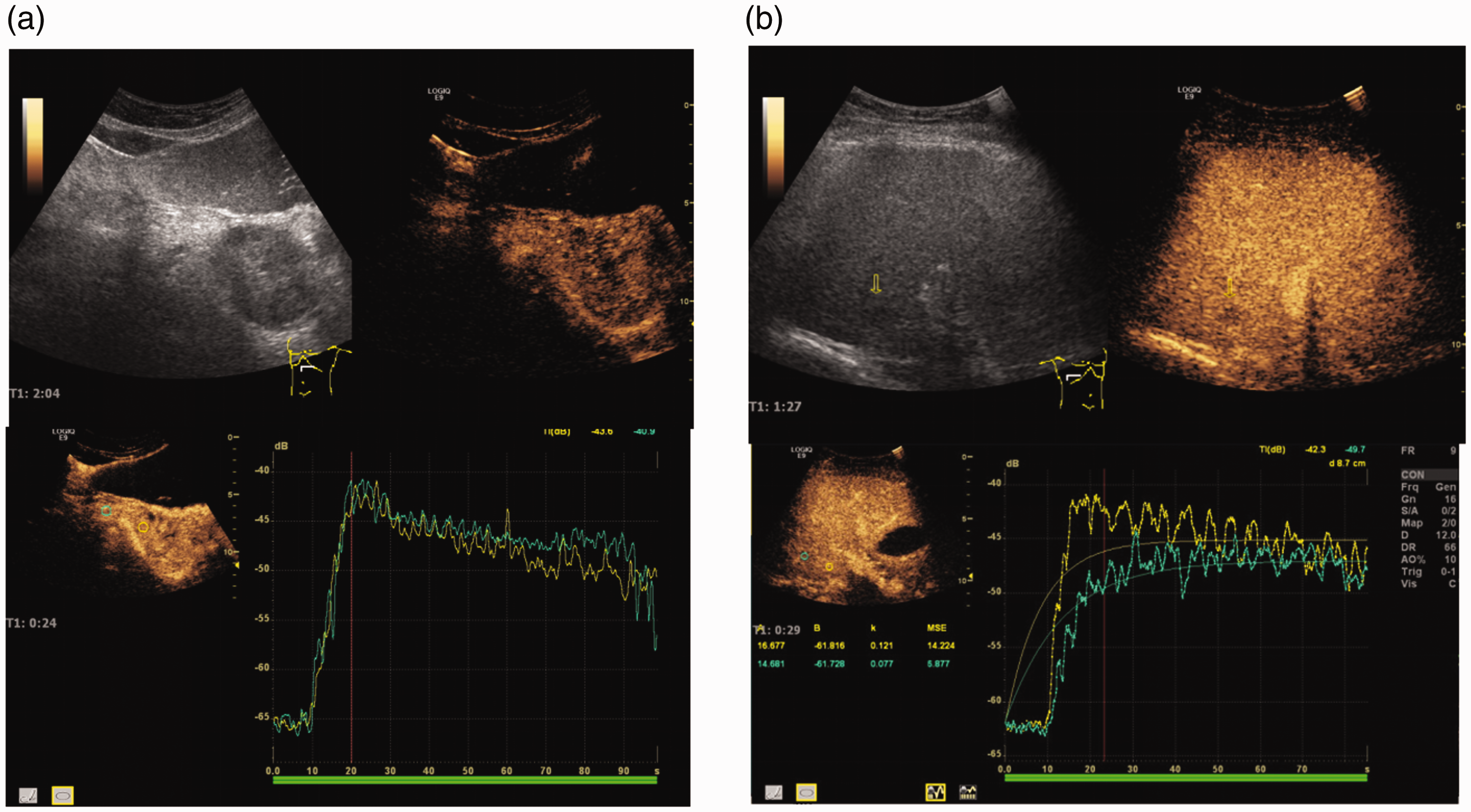
Contrast-enhanced ultrasonography analysis. (a) The pancreatic mass showed equal enhancement in the arterial phase and slightly faster withdrawal in the delayed phase. (b) The liver mass showed rapid and high enhancement in the arterial phase and low enhancement in the portal vein and delayed phase.
Contrast-enhanced magnetic resonance imaging (MRI) identified a round lesion 52 × 56 mm in size located in the pancreatic body and tail, with hypoenhancement on T2-weighted images and iso- to mild hypoenhancement on diffusion-weighted imaging (DWI). Thus, the lesion showed heterogeneous enhancement. In addition, vascular invasion of the spleen was observed (Figure 3a). In the liver, an 11- × 9-mm lesion was observed with ring hyperenhancement in the arterial phase and isoenhancement in the portal venous and delayed phases (Figure 3b).

Contrast-enhanced magnetic resonance imaging. (a) The pancreatic mass showed hypoenhancement on T2-weighted images and iso-to mild hypoenhancement on diffusion-weighted imaging. Vascular invasion of the spleen was observed. (b) The liver mass showed ring hyperenhancement in the arterial phase and isoenhancement in the portal venous and delayed phases.
Ultrasound-guided fine-needle puncture of the pancreatic lesion revealed a neuroendocrine tumour with necrosis, and the lesion was more likely to be a solid pseudopapillary tumour because of the limited number of tumour components in the puncture tissue. However, a neuroendocrine tumour could not be ruled out. The puncture biopsy specimen of the liver lesion revealed a small round cell malignant tumour.
Positron emission tomography-computed tomography (PET-CT) suggested a hypodense mass in the pancreatic body and tail and increased 18F-fluorodeoxyglucose metabolism, indicating pancreatic cancer with metastasis to the right liver.
We obtained patient consent to initiate treatment. The patient underwent surgery, during which a palpable mass measuring 7 × 7 × 8 cm was identified in the pancreatic body and tail. Invasion of the pancreatic capsule and transverse mesorectal root was observed. The pancreatic tail had adhered to the gastric fundus, and significantly enlarged lymph nodes were present. Adhesion between the right liver and the diaphragm was observed, and a lesion was identified on the surface. Therefore, laparoscopic exploration, liver lesion resection, splenectomy, pancreaticoduodenectomy, and partial gastrectomy were performed. The patient was discharged on the tenth post-operative day.
Macroscopically, there was a 6- × 6- × 4.5-cm mass in the pancreatic body and tail. The mass was greyish-white and solid and exhibited intratumoral haemorrhage (Figure 4). Histology and immunohistochemistry showed typical pancreatoblastoma (PB) features. The tumour was composed of acinar cells and showed ductal and squamous differentiation (Figure 5). Immunohistochemical staining showed alpha-1 antitrypsin (+), CK19 (+), P40 (+), beta-catenin (+), CK (Pan) (+), epithelial membrane antigen (EMA) (+), CD10 (+), synaptophysin (Syn) (+), DuPan-2 (+), and B72.3 (+). The liver mass was determined to be a hepatic metastasis from the primary PB.
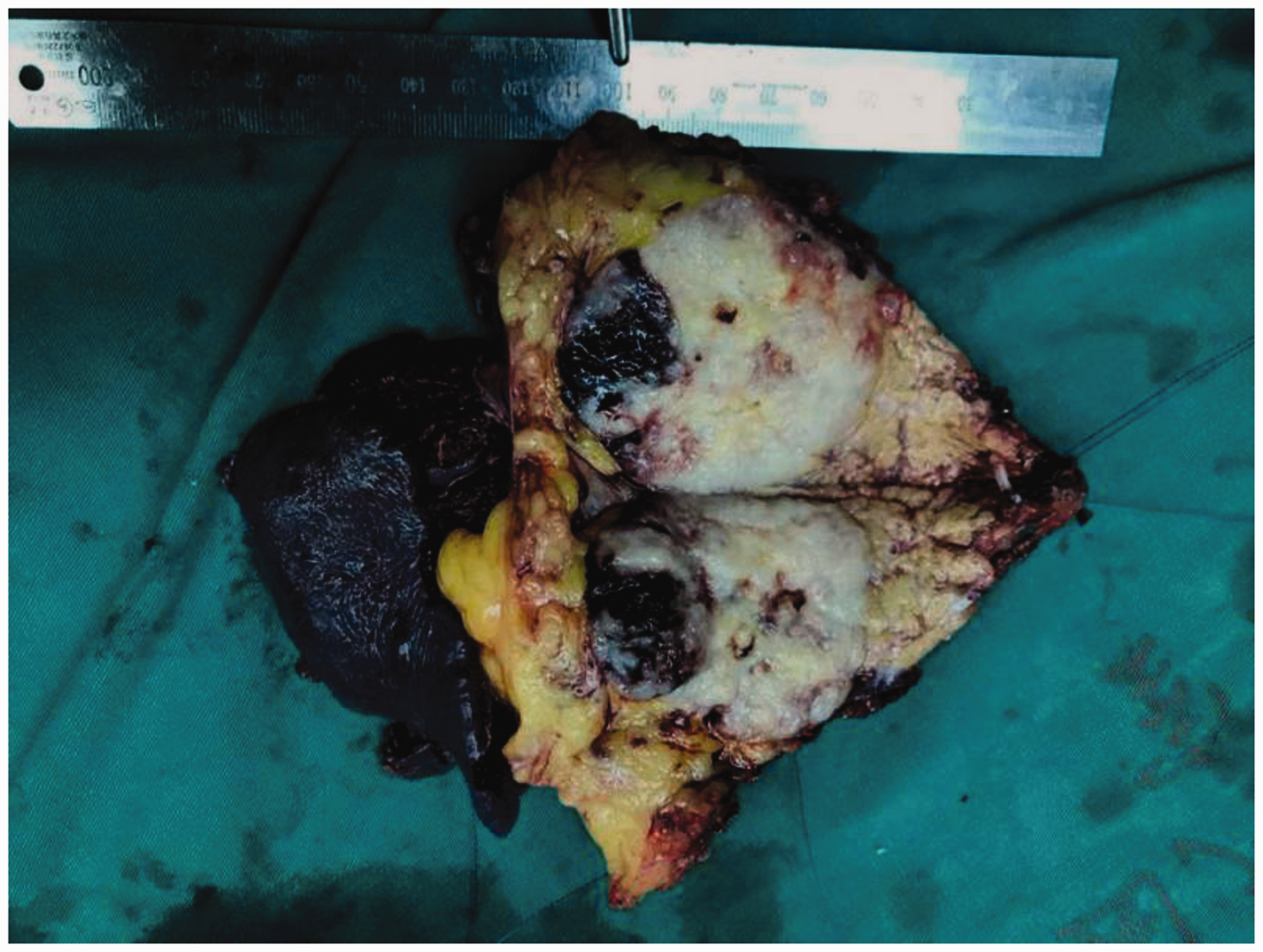
Gross pathology of the mass in the pancreatic body and tail. The pancreatic mass was greyish-white and solid and exhibited intratumoral haemorrhage.

Haematoxylin and eosin staining of the tumour. The pancreatic mass was composed of acinar cells and showed ductal and squamous differentiation (×100).
Follow-up CT scans of the abdomen were performed 3 months after surgery and revealed multiple liver metastases. The patient underwent five cycles of systemic chemotherapy with a regimen consisting of cisplatin, vindesine, and bleomycin and immunotherapy with an intravenous administration of programmed cell death 1 antibodies (120 mg). The patient died 16 months after surgery due to tumour spread.
Discussion
PB is a rare exocrine pancreatic malignancy. It mainly occurs in infants and young children under 10 years old, and it rarely occurs in adults, with no significant difference between the sexes. However, some literature reports suggest that the incidence in men is slightly higher than that in women.5,6 PB is a slow-growing tumour with diverse and nonspecific clinical manifestations. Clinically, it is often insidious until it reaches a considerable size, and in adult patients, abdominal pain, weight loss, or an abdominal mass are the main symptoms. 7 Other common symptoms include anorexia, changes in bowel habits, and jaundice. The prognosis of children is better than that of adults. The survival time in children is 5 to 22 years, whereas the average survival time in adults is only 18 months. 3 PB grows slowly, and most tumours are large with a diameter of 15 to 20 cm. 8 Tumours often compress the surrounding organs without invasion or local invasion, and vascular invasion is rare. PB usually presents as a well-defined and lobulated heterogeneous mass. It occurs in all areas of the pancreas, with the head of the pancreas as the most common location, 7 but the body and tail have also been reported to be involved in some cases. 9 In our patient, PB occurred in the tail of the pancreas.
PB varies greatly in biological behaviour, is often accompanied by local infiltration, and is prone to metastasis. The most common site for metastasis is the liver, followed by the lung and regional lymph nodes, and systemic spreading is rare. 10 In our patient, liver metastasis occurred. Beckwith–Wiedemann syndrome 11 and Cushing’s syndrome 12 can co-occur with this tumour in some patients, and the specific mechanisms need to be further studied.
There is no significant radiographic difference between adult and child PB. 9 , 15 Ultrasound images show a substantial mass in the pancreatic area, with uneven internal echocardiography and blood flow signals. On CT images, the main manifestations are a single, large, circular or lobulated mass, usually solid or cystic with clear boundaries due to a capsule and accompanied by scattered or aggregated calcification. On MRI, the main manifestations are low-to-medium-intensity signals on T1-WI, high-intensity signals on T2-WI, and mixed signals if intratumoral haemorrhage is present. MRI is favourable for visualizing the tumour capsule; the capsule shows moderate-intensity signals on T1-WI and low-intensity signals on T2-WI. In addition to invading the surrounding vessels, the mass also compresses the surrounding tissues, and common bile duct and intrahepatic bile duct dilatation are observed when the tumour is located in the head of the pancreas.
In previous reports, contrast-enhanced MRI showed uneven moderate enhancement of the septum, rapid enhancement of the capsule, and wash-out, and the central part was mostly necrotic without enhancement due to insufficient blood supply.13,14 The ultrasonographic and MRI findings in our patient were consistent. Sometimes, metastases to the liver, blood vessels, or lymph nodes are detected on imaging. 15
The diagnosis of PB is mainly based on pathology. 16 Epithelial cells are abundant and separated by fibres into well-defined islands, which present a “map” appearance at low magnification, and squamous bodies and cell structures containing zymogen granules are characteristic of PB. The tumour cells comprise multiple pancreatic cells and show simultaneous adenoid, tubular adenoma, and endocrine differentiation.
Immunohistochemical staining showed a positive reaction for cytokeratins, AFP, CEA, EMA, Syn, DuPan-2, and B72.3, which supports the diagnosis of PB to a certain extent. 17
Because of the small number of patients receiving treatment for adult PB reported to date, the optimal treatment strategy has not been standardized. However, for the treatment of adult PB, surgical resection is currently the main strategy, 2 the role of adjuvant chemotherapy and radiotherapy remains controversial, and the optimal chemotherapy regimen is still under discussion.
Conclusion
The preoperative diagnosis of adult PB is particularly challenging. The diagnosis cannot be confirmed according to clinical manifestations and imaging examinations, and the diagnosis depends on pathological examination. However, we believe that the clinical awareness of this disease should be improved, and PB should be considered during the diagnosis of solid or cystic abdominal masses to achieve early detection and proper treatment and improve patient prognosis.
Footnotes
Ethics statement
Informed written consent was obtained from the patient prior to the publication of this report, and ethical approval was given by Zhejiang Provincial People’s Hospital (202107071600000113105).
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.