
Abstract
Chronic idiopathic constipation is highly prevalent among adults. Bile acids (BAs) and the enterohepatic BA circulation modulate colonic secretion and motility that affect transit. BAs in the colon have a dual action as osmotic and stimulant agents. Newer agents, such as elobixibat (A3309), an inhibitor of the ileal BA transporter, have the potential to improve significantly the management of chronic constipation, with minimal adverse effects. Elobixibat modulates the enterohepatic BA circulation, enhancing the delivery of BAs to the colon where they induce secretory and motor effects. Secondary effects of the inhibition of BA absorption are reduced activation of the farnesoid X receptor, decreased secretion of fibroblast growth factor-19 into the portal circulation, and increased BA synthesis. This review focuses on the role of BAs, the enterohepatic BA circulation, and an ileal BA transporter inhibitor (elobixibat) in chronic constipation.
Introduction
Constipation is a syndrome defined by abnormal bowel symptoms that may be primary or secondary to an underlying disorder [Bharucha et al. 2013b]. Commonly used criteria differentiate between ‘functional or chronic idiopathic constipation’ (CC) and ‘constipation-predominant irritable bowel syndrome’ (IBS-C), and define CC as two or more of the following for at least 12 weeks in the preceding 6 months: straining, lumpy or hard stools, sensation of incomplete evacuation, sensation of anorectal obstruction/blockade, manual maneuvers to facilitate defecation, and absence of loose stools [Longstreth et al. 2006]. CC can be associated with normal colonic transit, slow colonic transit, and/or defecatory disorders [Bharucha et al. 2013b; Camilleri, 2012]; it is worth noting that defecatory disorders may also be associated with slow colonic transit [Nullens et al. 2012].
The prevalence of CC is 16% in adults overall and almost double that number (33.5%) in people over 60 years of age [Bharucha et al. 2013b]. The diagnosis of CC requires a careful history and physical examination, including rectal examination. Organic disorders need to be excluded, especially with recent onset of constipation or alteration of bowel function. Treatment algorithms have been proposed based on consensus guidelines: for details, refer to the recent American Gastroenterological Association technical review on constipation [Bharucha et al. 2013b], and refer to Figure 1 for the diagnostic algorithm [Bharucha et al. 2013a]. The prevalence of each subclass of CC varies among different studies. In 1411 patients evaluated by a single gastroenterologist in a tertiary medical center, 960 (68%) patients had normal transit constipation, 61 (4.3%) patients had slow transit constipation, and 390 (27.6%) patients had a defecatory disorder [Nullens et al. 2012].

Diagnostic algorithm for chronic constipation. (Reproduced with permission from Bharucha et al. [2013a].)
In the case of CC without defecatory disorder, the available medications include: stool softeners (docusate sodium), osmotic agents (sorbitol, lactulose, and polyethylene glycol), stimulants (glycerin, bisacodyl, picosulfate, senna, and cascara), saline laxatives (magnesium), lubricant (mineral oil), oral secretagogues, such as lubiprostone [Drossman et al. 2009; Schey and Rao, 2011], and linaclotide [Lembo et al. 2011; Andresen et al. 2007], 5-HT4 agonists in several countries other than the USA, for example, prucalopride [Bouras et al. 2001; Camilleri et al. 2008], and enemas (mineral oil retention enema, tap-water enema, phosphate enema, and soapsuds enema). In spite of the availability of numerous pharmacologic options, up to half of the adults with CC reported that they were not completely satisfied with the current treatment options prior to the approval of linaclotide, lubiprostone, and prucalopride [Johanson and Kralstein, 2007], including patients participating in phase III clinical trials of new treatments for CC [e.g. Camilleri et al. 2008]. Thus, there is still an unmet need for safe and effective treatments for CC.
Significant advances in understanding the underlying mechanisms of CC have led to novel targets, receptors, neurotransmitters, and fluid and electrolyte secretion and reabsorption. In addition to the approved drugs detailed above, others are in development: prokinetic 5-HT4 receptor agonists, such as velusetrag and naronapride; guanyl cyclase C receptor agonists, such as plecanatide; a bile acid (BA) (delayed-release chenodeoxycholic acid [CDCA]); an ileal BA transporter (IBAT) inhibitor (elobixibat) [Camilleri, 2013].
This review focuses on the role of BAs, the enterohepatic circulation, and the IBAT inhibitor, elobixibat, in CC.
Enterohepatic circulation of BAs
BAs are detergent molecules mainly responsible for fat emulsification, and lipid digestion and absorption in the small intestine. In addition, BAs are versatile molecules with multiple other functions in the gastrointestinal tract, such as antimicrobial activity, modulation of fluid and electrolyte absorption, regulation of epithelial gene expression, growth of intestinal epithelium, and gastrointestinal motility [Hofmann, 2009]. Primary BAs (cholic acid, CDCA, and ursodeoxycholic acid) are synthesized from cholesterol in the hepatocyte, secreted from the liver predominantly in a conjugated state with glycine and taurine, and, following their pivotal role in fat emulsification and lipid digestion and absorption in the small intestine, they are extensively (95%) reabsorbed through the IBAT (also called the apical sodium-coupled BA transporter). About 5% of BAs pass into the colon where they are deconjugated and dehydroxylated by intestinal bacteria into secondary BAs, deoxycholic acid (DCA) and lithocholic acid (LCA). Thus, the enterohepatic circulation of BAs is the process whereby primary BAs, secreted from the hepatocyte into the canalicular bile, traverse through the biliary tract into the duodenum, and course through the small bowel until actively absorbed in the terminal ileum, or passively absorbed by diffusion in the colon (Figure 2). Once they reach the portal circulation and are transported to the liver, BAs are taken up into the hepatocytes by specific transporter molecules [Hofmann, 2009].
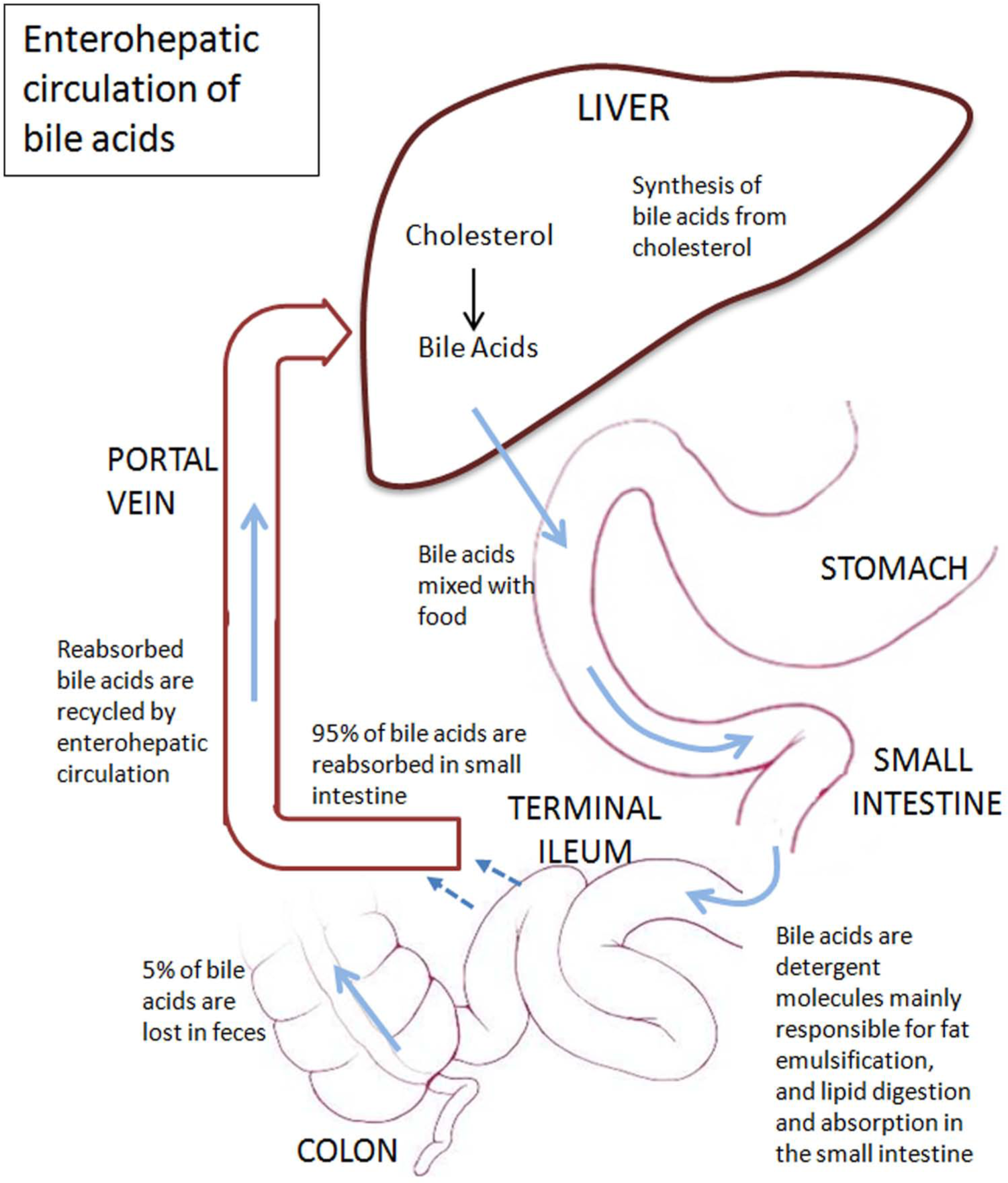
Enterohepatic bile-acid circulation and synthesis.
The enterohepatic circulation of BAs has two regulatory sites that produce negative feedback in BA synthesis. In the hepatocyte, BAs inhibit the function of the farnesoid X receptor (FXR) to induce a short heterodimer protein that activates cholesterol 7α-hydroxylase (CYP7A1), down-regulating BA biosynthesis [Twisk et al. 1995]. In the enterocyte, BAs activate FXR to induce the enterocyte to secrete fibroblast growth factor-19 (FGF-19), an analog of FGF-15 in mice, into the portal circulation. FGF-19 binds to fibroblast growth factor receptor 4 (FGFR4). This involves interaction of a separate molecule, klothoβ (KLB), on the hepatocyte that leads to the suppression of CYP7A1 expression and decreased BA synthesis [Wong et al. 2011a; Jung et al. 2007; Cicione et al. 2012; Johnston et al. 2011].
BAs and gastrointestinal motility
BAs modulate colonic transit by two mechanisms: secretory and prokinetic [Camilleri, 2014]. Thus, BAs increase colonic secretion of water and electrolytes. In 20 healthy volunteers, perfusion of dihydroxy BAs into the colon in concentrations of 3 mM or higher induced dose-related secretion of chloride, sodium, potassium, bicarbonate, and water when compared with an iso-osmolar control electrolyte solution [Mekhjian et al. 1971]. In addition, certain BAs are prokinetic in the colon, stimulating high amplitude, propagated contractions. In 10 healthy volunteers, when CDCA, was perfused into the rectum and left colon at 1 mM concentration, it doubled the frequency of propagated contractions [Bampton et al. 2002]. These findings on the effects of BAs on colonic motor function were confirmed by two randomized, double-blind trials using a BA sequestrant (colesevelam), which induced slowing of colonic transit in irritable bowel syndrome with diarrhea (IBS-D), whereas CDCA accelerated colonic transit in healthy subjects [Odunsi-Shiyanbade et al. 2010], and in patients with IBS-C [Rao et al. 2010]. Thus, for example, ileocolonic-release CDCA (IR-CDCA), 500 mg and 1000 mg, was tested in a randomized, double-blind, placebo-controlled study of 36 women with IBS-C. IR-CDCA accelerated colonic transit, induced looser stool consistency, increased stool frequency, and produced greater ease of stool passage when compared with placebo. The most common side effect was lower abdominal cramping and pain in 45% of participants, consistent with the significant stimulation of colonic motility [Rao et al. 2010].
Deficiency of FGF-19 produces increased BA synthesis and diarrhea [Walters et al. 2009]. In addition, variants in the genes for the proteins involved in the enterohepatic BA circulation may also provide evidence of the potential of BA to modulate colonic motility. Genetic variation in KLB (Arg728Gln) is associated with IBS-D and accelerated colonic transit: the gene variant results in instability of the KLB protein synthesized, resulting in the inability of FGF-19 to reduce hepatocyte BA synthesis [Wong et al. 2011a]. FGFR4 genetic variations alone [Camilleri et al. 2014], or by interaction with the KLB variations, alter colonic transit [Wong et al. 2011a]; in addition, FGFR4 polymorphisms are also associated with alterations in the colonic transit in response to administered CDCA [Rao et al. 2010].
Finally, the G-protein-coupled BA receptor 1 (GPBAR1) is present in enteroendocrine cells and in components of the motor and sensory apparatus of the enteric nervous system [Poole et al. 2010]. Expression and function of GPBAR1 are involved in the prokinetic effects of BAs [Alemi et al. 2013]; genetic variation in GPBAR1 was associated with acceleration of small intestinal and colonic transit [Camilleri et al. 2011].
BAs and constipation
Individuals with IBS-C have a decreased concentration of secretory unconjugated BA, CDCA, nonsecretory BA, and DCA, when compared with healthy controls or patients with IBS-D (Figure 3) [Shin et al. 2013; Wong et al. 2012]. The nonsecretory, unconjugated BA, LCA, was the predominant fecal BA when compared with healthy controls in IBS-C [Shin et al. 2013]. In addition, there is a positive correlation between stool number and form, colonic transit at 24 h and 48 h, total fecal unconjugated BA, and percentage of primary BAs [Shin et al. 2013]. Conversely, there is a negative correlation between colonic transit and percentage of fecal LCA, that is, the slower colonic transit in patients with IBS-C is associated with higher fecal LCA [Shin et al. 2013].

Individual predominant fecal bile acids in patients with IBS-C and healthy controls. (Data taken from Shin et al. [2013].)
Elobixibat
Chemistry, pharmacology, and pharmacokinetics
Elobixibat (A3309) is the pure enantiomer of a synthetically modified 1,5-benzothiazepine, based on a seven-membered heterocyclic ring attached to a benzene ring (chemical formula C36H45N3O7S2). It acts locally in the lumen of the gastrointestinal tract by binding to and partially inhibiting IBAT in the ileal mucosa. Elobixibat is highly selective for IBAT, with an affinity more than 450-fold higher than for human liver sodium-dependent BA transporter, and more than 9000-fold higher than for neutral amino-acid transporter [Gillberg, 2010]. Elobixibat increased hepatic BA synthesis in dogs in a dose-dependent manner when compared with controls [Gillberg, 2010].
Elobixibat is minimally absorbed into the circulation after oral administration. The low systemic bioavailability supports elobixibat’s mechanism of action as a local inhibitor of IBAT. When absorbed, elobixibat is protein bound (> 99%) in plasma, with a half-life of less than 4 h. Elobixibat inhibits CYP2C9 and CYP3A4. However, since its absorption is so low, there is a low risk of drug–drug interactions as a result of inhibition of the CYP enzyme after oral dosing [Simren et al. 2011].
Clinical trials: pharmacodynamics, safety, and efficacy
The effects of elobixibat in CC have been assessed in three published trials to date.
A phase I, randomized, double-blind, placebo-controlled, single-center trial over 14 days focused mainly on safety and tolerability of elobixibat in 30 CC patients in six groups: placebo versus elobixibat at doses 0.1 mg, 0.3 mg, 1 mg, 3 mg, and 10 mg [Simren et al. 2011]. In addition, colonic transit time (CTT) by radiopaque markers, plasma C4 (a surrogate of the rate of hepatic BA-synthesis rate), and cholesterol levels were assessed. Elobixibat, 10 mg daily, accelerated colonic transit, reducing CTT when compared with placebo. Elobixibat also increased the plasma C4 levels and decreased total cholesterol and low-density lipoprotein (LDL) cholesterol in a dose-dependent manner. These three actions are consistent with the reduced ileal BA absorption in the ileum, reducing the negative feedback of hepatocyte BA synthesis, and therefore shunting steroid synthesis in the hepatocyte from cholesterol and LDL cholesterol to increased BA synthesis.
In a phase IIa, single-center, randomized, double-blind, placebo-controlled trial, 36 women with CC by Rome II criteria were randomized to oral placebo, 15 mg, or 20 mg elobixibat for 14 consecutive days. Colonic transit was measured over 48 h by a validated scintigraphic method. Bowel functions were assessed as secondary endpoints. Biochemical secondary endpoints included serum C4, triglycerides, total cholesterol, high-density lipoprotein (HDL) cholesterol, and LDL cholesterol. Elobixibat accelerated colonic transit, induced looser stool consistency, decreased constipation rating, and reduced straining compared with placebo (Figure 4). The most common side effects were lower abdominal cramping/pain in 36% of participants and 50% of participants on 15 mg and 20 mg, respectively (p = 0.004), and diarrhea in 30% of participants receiving the 20 mg dose (p = not significant) [Wong et al. 2011b].

Effect of elobixibat (A3309) and placebo on overall colonic transit at 24 h and 48 hours (left panel), mean ± standard error of mean by Dunnett’s test (each dose versus placebo) *p < 0.05, ** p < 0.01, *** p < 0.001. Note acceleration of colonic transit with both A3309 doses.
In a multicenter, phase IIb, double-blind, placebo-controlled trial, 190 CC patients were randomized to placebo, 5 mg, 10 mg, or 15 mg elobixibat daily for 8 weeks. The primary endpoint was change in the frequency of spontaneous bowel movements (SBMs) per week at week 1 of treatment, compared with baseline. Other bowel function characteristics, plasma C4, total cholesterol, HDL cholesterol, LDL cholesterol, and triglycerides were secondary endpoints. Elobixibat was associated with a significantly greater increase in the number of SBMs per week from baseline to placebo (mean change 4.0 for 10 mg [p < 0.002], and 5.4 for 15 mg [p < 0.001] elobixibat versus 1.7 for placebo). The increased SBMs with elobixibat were dose dependent and maintained over the duration of the 8-week treatment period, when compared with placebo (Figure 5). In addition, elobixibat significantly loosened stool consistency and decreased straining during all 8 weeks of treatment compared with placebo, and elobixibat, 15 mg, improved bloating severity, but not abdominal discomfort or pain. The studies reported similar adverse effects described as mild or moderate abdominal cramps or pain (0%, 10%, 11%, and 27% in the placebo, 5 mg, 10 mg, and 15 mg elobixibat, respectively), and diarrhea (2%, 8%, 6%, and 13% in the placebo, 5 mg, 10 mg, and 15 mg elobixibat groups, respectively). There were no severe adverse events [Chey et al. 2011].

Change from baseline in weekly SBM frequency for treatment week 1.
Currently, two large, multicenter phase III trials, ECHO 1 and ECHO 2, are enrolling patients with a goal to recruit 1700 patients in 200 sites worldwide. The study is intended to demonstrate the efficacy and safety of repeated daily doses of elobixibat compared with placebo over a period of 26 weeks in the ECHO 1 trial [ClinicalTrials.gov identifier: NCT01827592], and for 12 weeks in the ECHO 2 trial [ClinicalTrials.gov identifier: NCT01833065]. Both trials are expected to be completed by the end of 2014.
Potential role of elobixibat in patients with chronic constipation
The presumed dual action of elobixibat on colonic secretion and motility may be advantageous in the treatment of CC when compared with single-action agents such as osmotic agents, secretagogues, or prokinetics. The dual action may potentially simplify the treatment of patients with constipation with no evidence of a rectal evacuation disorder without having to determine whether the problem is due to normal transit or slow transit constipation. However, formal studies are required to assess the effects of elobixibat on colonic contractility, and on the resolution of symptoms and delayed transit in patients with slow transit constipation before it can be recommended in preference to other agents. In fact, the relative efficacy of all these agents in the treatment of slow transit constipation has not been tested.
Theoretical risk of colorectal cancer
A meta-analysis of 20 clinical trials showed increased fecal excretion of the primary BA, CDCA, in patients with colorectal cancer [Tong et al. 2008]. However, there is no direct evidence of causation between BAs and the development of colorectal cancer based on epidemiological studies [Haines et al. 2000; Little et al. 2002; Hill et al. 1982], therapeutic studies in patients who received CDCA for several months or years for gallstone dissolution [Iser and Sali, 1981], and in patients after partial ileal bypass performed for hyperlipidemia at 5 years [Buchwald et al. 1998], or in 25 years of follow up [Buchwald et al. 2010]. Thus, the theoretical colorectal cancer risk with exposure to increased intracolonic BA concentrations needs to be further evaluated, but the current evidence is reassuring. As with all new drug-development programs, meticulous studies including risk management programs will be necessary to exclude potential for colonic carcinogenicity.
Conclusion
Chronic constipation has a high prevalence among adults, and the current treatments do not meet patients’ expectations. Elobixibat, an IBAT inhibitor, modulates the enterohepatic BA circulation, and increases BA synthesis, enhancing the delivery of BAs to the colon to increase colonic motility, and secretion and fecal excretion of BAs. Elobixibat has significant effects on the manifestations of CC, with minimal and tolerable adverse effects.
Footnotes
Acknowledgements
The authors thank Mrs Cindy Stanislav for secretarial support.
Funding
MC is supported by the NIH (grant number RO1-DK92179).