
Abstract
Background:
Benign occlusive esophageal strictures create substantial morbidity and have poor surgical outcomes. Various endoscopic techniques have been described to manage these strictures. The challenge remains to maintain adequate long-term esophageal patency and to limit the need for serial endoscopic dilations. Little has been reported regarding the management of these benign occlusive strictures.
Methods:
We report a case series describing the management of technically challenging benign occlusive esophageal strictures. Three patients with occlusive esophageal strictures of differing etiologies were treated using a variety of endoscopic methodologies.
Results:
The first patient sustained a caustic oropharyngeal injury resulting in a proximal esophageal stricture which was treated by using a combined antegrade retrograde dilation (CARD) with argon plasma coagulation (APC) and needle knife dissection resulting in the successful recanalization and patency of his stricture. A second patient developed an esophageal stricture following radiotherapy, and was treated with a CARD procedure and serial balloon dilations in combination with APC to successfully achieve esophageal luminal patency. The final patient acquired an occlusive esophageal stricture after treatment for thyroid cancer which was treated with endoscopic needle knife dissection followed by serial balloon dilations to successfully manage this stricture.
Conclusions:
Occlusive esophageal strictures pose a difficult challenge to gastroenterologists and little has been reported with regards to their endoscopic management. Using the CARD technique, needle knife dissection and APC, individually or in combination, luminal patency of occlusive esophageal strictures can be accomplished safely with good results.
Keywords
Introduction
Occlusive esophageal strictures carry significant morbidity for patients and are associated with poor surgical outcomes [Moyer et al. 2006; Hordijk et al. 2006]. The majority of strictures occur in the setting of malignancy from primary tumors of the esophagus causing direct luminal obstruction or other tumors of the head and neck leading to extrinsic esophageal compression. However, a considerable number of patients develop strictures secondary to benign causes [Moyer et al. 2006; Hordijk et al. 2006; Al-Haddad et al. 2007; Fry and Flesicher, 1997]. Whereas treatment of malignant esophageal strictures focuses on treating the underlying malignancy and is often palliative, patients with benign esophageal strictures generally have a longer life expectancy and need more permanent solutions.
Etiologies of benign occlusive esophageal strictures include peptic injury due to chronic esophageal acid exposure, anastomotic strictures, sequelae of radiation treatment, Schatzki’s rings, esophageal webs, caustic exposures and complications of ablative therapy for Barrett’s esophagus [Siersema and de Wijkerslooth, 2009; Baron, 2011]. Approximately 60–70% of benign strictures are caused by peptic injury followed by 5–45% of cases caused by anastomotic lesions [Hordijk et al. 2006; Siersema and de Wijkerslooth, 2009]. Other causes include aggressive treatments for Barrett’s esophagus and nasogastric tube injury [Baron, 2011].
The development of these strictures and the prolonged symptoms associated with them are associated with considerable morbidity as therapies are largely unsuccessful [Baumgart et al. 2005; Laurell et al. 2003; Cox et al. 1988]. The dysphagia to both solids and liquids often progresses to the inability of patients to swallow their own secretions and is, as a result, associated with aspiration, social isolation and severe depression [Mukherjee et al. 2008].
Currently, multiple endoscopic treatment modalities are utilized to treat esophageal strictures including serial dilations, needle knife dissection, argon plasma coagulation (APC), temporary stent placement, laser cannulation and self dilation [Siersema, 2008]. However, when complete luminal occlusion occurs, treatment options are limited. Combined antegrade and retrograde dilation (CARD) has been successfully utilized to attain esophageal patency in these situations [Bueno et al. 2001; Wang et al. 2002; Maple et al. 2006; Lew et al. 2004; van Twisk et al. 1998].
We describe a case series of three patients with benign occlusive esophageal strictures treated utilizing multiple endoscopic modalities to successfully restore esophageal luminal patency.
Methods
We describe three cases of benign occlusive esophageal strictures of differing etiologies which progressed to occlusive esophageal strictures despite standard therapies. All three patients were treated successfully using a combination of the CARD technique, laser cannulation, APC, needle knife dissection and, serial Savory dilations from 2006 to 2010. Table 1 provides a summary of patient characteristics and techniques.
Summary of patient characteristics and techniques.
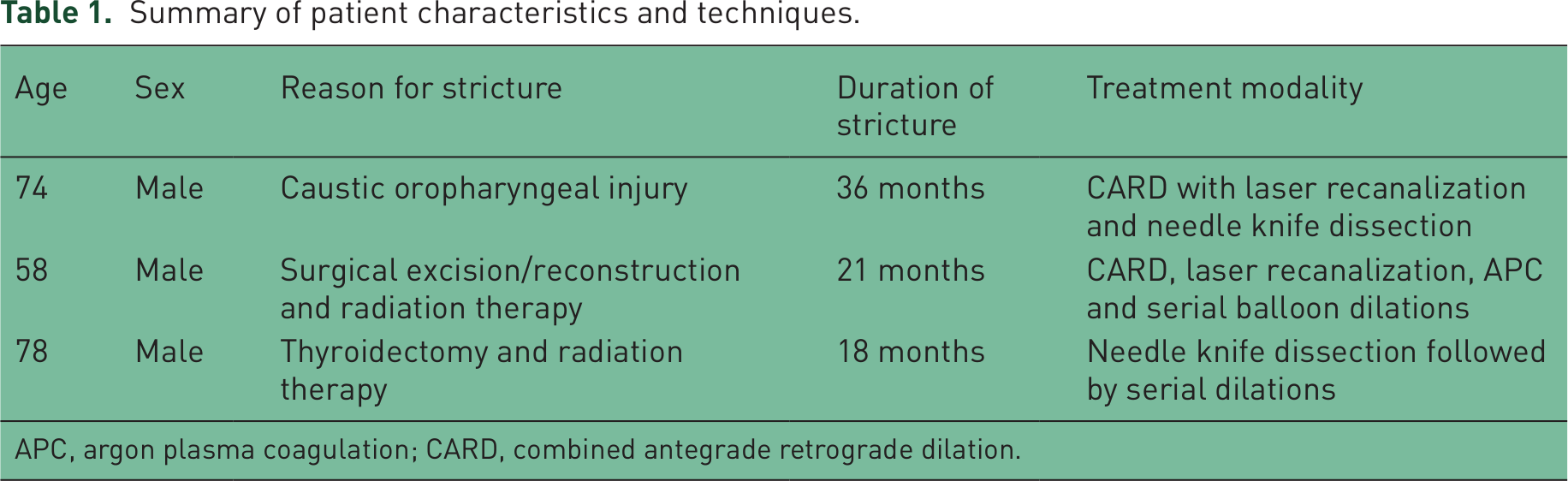
APC, argon plasma coagulation; CARD, combined antegrade retrograde dilation.
Case I
A 74-year-old man was involved in an accident with an acetylene torch and sustained significant blowback burns to the left side of his face, left eye, oropharynx and esophagus. He required a laryngectomy, permanent tracheal stoma, and reconstruction of the left face and eye. Esophageal reconstruction was attempted with a tabularized musculocutaneous free flap based on the radial artery subcutaneous flap procedure which was unsuccessful and eventually occluded. Over the course of 3 years, he underwent repeated esophageal dilations to which he did not respond. After having esophageal stents placed, the patient had pharyngeal irritation resulting in the dislodging of the stents and their expulsion. He eventually required a gastric feeding tube for nutrition. In addition, the patient developed severe depression and expressed suicidal ideation.
Due to the failure of standard techniques at maintaining esophageal patency, the patient was taken to the operating room for a multidisciplinary approach at recanalization of the occluded segment of the esophagus using the CARD approach. An adult upper endoscope was inserted antegrade through the oropharynx and a second ultrathin upper endoscope was inserted retrograde through the gastrostomy site. The two scopes were aligned under fluoroscopic visualization in two dimensions (Figure 1). A 19-gauge fine aspiration needle was then used to traverse the stricture; sequential 0.9, 1.7, 2.0 and 2.5 Spectranetics French Turbo Excimer laser fibers were then used to recreate the occluded esophageal lumen followed by immediate serial balloon dilatations up to 18 mm (Figure 2). After completing dilations, both the antegrade and retrograde endoscopes could easily traverse the previously occluded segment.

Fluoroscopic image showing orientation of two endoscopes around the stricture during combined antegrade and retrograde dilation (CARD) technique.

Endoscopic view of the stricture after canalization.
An Asahi 0.014 wire was left in place to be used for future dilatations. The patient tolerated the procedure well. This patient underwent serial dilations and was eventually taught to perform self dilations using an unguided Maloney Bougie dilator; after over a year of dilations there was no longer any need for the gastrostomy tube and it was removed. Subsequently, the patient has been able to tolerate a soft mechanical diet and is now able to tolerate almost all forms of food. The patient continues to perform self dilations with the Maloney Bougie dilator at 4–6 week intervals.
Case II
A 58-year-old man with a past medical history of a carcinoma of the base of the tongue was treated with definitive chemoradiation resulting in the development of an esophageal stricture and had a gastrostomy tube placed. After the stricture developed, dilation was performed resulting in perforation with resulting mediastinitis and pneumothorax. He then underwent a patch esophagostricturoplasty using a pedicled myocutaneous flap based on the sternocleidomastoid. Unfortunately, the patient developed complete re-occlusion with 2–3 weeks. Ultimately, the patient developed a complete occlusion of the lower cervical and upper thoracic esophagus. As a result, the patient was taken to the operating room for a multidisciplinary approach at recanalization of the occluded segment of the esophagus.
Using the CARD approach, an adult upper endoscope was inserted orally and a second was inserted retrograde through the patient’s gastrostomy site. The two scopes were aligned in an attempt to percutaneously join the upper and lower esophageal pouches aided by transillumination. A biopsy needle was then passed through the antegrade scope and into the area of esophageal occlusion at the distal esophageal pouch. A 0.018 guide wire was passed and was retrieved from the gastric lumen using alligator forceps passed through the retrograde endoscope.
Using the Spectranetics Excimer laser with 2-mm and 2.5-mm Turbo laser probes, a 5 mm channel was created across the occlusive stricture. Once the laser recanalization was accomplished, sequential dilations were accomplished using 5 mm × 4 cm, 7 mm ×4 cm, and 9 mm × 4 cm balloon dilatators. The patient tolerated the procedure well.
At a 1 month follow up, the stricture area was extensively treated with APC to ablate the mucosa followed by dilatation. After a year of dilations, the patient’s stricture stabilized and no longer requires dilation. Eighteen months after initial placement of his gastrostomy tube, it was removed as he was tolerating a regular diet. Patient had no dysphagia until his last follow up 2 years after the procedure.
Case III
A 78-year-old man with a past medical history of metastatic papillary thyroid cancer to the neck and lungs underwent total thyroidectomy and left modified neck dissection. He underwent I-131 ablative treatment with 100 mCi in addition to external radiation treatment to the neck. Due to the longstanding radiation, he developed a complete proximal esophageal occlusion that was not amenable to multiple attempts at dilation over 2 years.
Subsequently, he was taken to the operating room for an endoscopic needle knife mucosal dissection (Figure 3). Using an ultrathin upper endoscope, the stricture was visualized and the scope was advanced through the stricture into the esophageal lumen. It was noted that the proximal esophagus contained a 3 cm stricture from the cricopharyngeus to the upper esophagus with an unremarkable appearance of the remainder of the esophageal mucosa. The gastric lumen was examined in forward and retroflexed view and was unremarkable. A 0.035 guide wire was inserted through the scope and curled in the gastric lumen.

Endoscopic view of stricture.
The scope was withdrawn and a Pentax pediatric upper endoscope was inserted over the wire. The scope was advanced with some resistance through the esophageal stricture. A needle knife was then inserted through the scope and linear mucosal incisions were made along the stricture (Figure 4). Through-the-scope balloon dilation was then performed sequentially from 8 to 12 mm. The patient tolerated the procedure without any complications. The patient underwent a repeat needle knife mucosal dissection followed by serial dilations. Six months after initial mucosal dissection, patient was able to tolerate soft foods. Patient needed four more sessions of dilations with through the scope balloon at an interval of 2–3 months until his dysphagia was completely resolved. Patient had no evidence of stricture recurrence at 42 weeks follow up.

Endoscopic view after needle knife incisions.
Results
All three of our patients were successfully treated using individualized and varied therapeutic modalities without complications. All three patients required close follow up with serial dilations. All three patients resumed oral feedings with discontinuation of tube feedings.
Discussion
The pivotal target in management of esophageal strictures is relief of dysphagia. Treatment of simple strictures (focal, straight, less than 2 cm, allow passage of endoscope) can be accomplished by dilation using balloon or other mechanical dilating devices under endoscopic and or fluoroscopic guidance [Lew and Kochman, 2002]. Complex strictures (longer than 2 cm, tortuous or with diameter that prevents passage of an endoscope of normal diameter) often require combination of modalities such dilation, intralesional steroid injection, sent placement or incisional therapy using electrocautery with or without APC [Hordijk et al. 2006; Al-Haddad et al. 2007; Fry and Fleischer, 1997].
Occlusive benign esophageal strictures pose a challenge to gastroenterologists and thoracic surgeons. Recent advancements in endoscopic techniques have provided various modalities which can be individualized or used in combination to restore esophageal luminal patency. In our case series, we have demonstrated that a multidisciplinary approach (gastroenterologists, thoracic surgeons and vascular surgeons) utilizing modalities such as the CARD approach, laser recanalization, APC and needle knife along with balloon or Savory dilations used in combination are safe and sustainable methods with which to achieve esophageal patency after complete occlusion. The applicability of each modality in a particular setting is very important for final success.
Clinical judgment based on individualized anatomical variations should determine the utilization of the endoscopic techniques implemented. The CARD approach and laser recanalization, in particular, seem best utilized when blind pouches are encountered in the esophagus. The CARD approach especially is valuable in identifying the initial site to attempt canalization. Fluoroscopic alignment of the antegrade and retrograde endoscope, as well as transillumination seen by the antegrade endoscope, helps in identifying the safest site for needle puncture in occlusive strictures. Different accessories have been used to puncture the membrane ranging from biopsy forceps for a thin membrane to an endoscopic ultrasound (EUS) needle to traverse longer obstruction [Moyer et al. 2006]. We have found this method to be safe and effective as also described in some other reports [Moyer et al. 2006; Al-Haddad et al. 2007; Dellon et al. 2010]. Appropriate patient selection is important as the incidence of esophageal perforation can be significant [Dellon et al. 2010]. Laser has classically been used to recanalize malignant obstructions in the gastrointestinal tract [Kiefhaber, 1987]. Use of laser in benign esophageal strictures has not been reported earlier. In our experience laser is extremely valuable in cases with extensive fibrosis making other modalities of recanalization technically challenging. With the use of laser more precise results can be achieved without conferring additional risk of perforation. Needle knife dissection and APC can be applied where a lumen is still visible based on operator comfort. Both modalities were sequentially used in our cases after canalization was achieved. In our third case needle knife was used to make radial cuts prior to dilation in an attempt to distribute the radial force of the dilating balloon evenly to avoid perforation. APC can specially be useful in management of strictures after failed stent placement as it can also aid in trimming or removal of stents [Setoyma et al. 2013]. Covered self-expanding metal stents have been used for benign esophageal strictures, but are often associated with complications such as stent migration and recurrence of symptoms after stent removal [Hirdes et al. 2012].
Minimally invasive esophagectomy has been described in recent years for the management of patients refractory to other modalities [Nguyen et al. 2003]. Esophagectomy can be a potential option for some of these patients, but in our experience it can be technically challenging in the setting of extensive fibrosis and radiation-induced changes. Plastic reconstruction is another option and is often associated with failure in patients with prior radiation [Taghinia et al. 2009]. It is notable that two of our patients had failed plastic reconstruction, the gold standard of treatment in radiation-induced esophageal occlusion. The reconstructive surgeries are associated with the risk of surgery and flap loss. As such, based on this small series, antegrade–retrograde laser recanalization should be considered prior to embarking on open surgical techniques. Since many of these patients have had radiation, reconstruction is a high risk procedure.
Moreover, in addition to nutritional deficiencies, our patients suffered from significant psychological morbidity secondary to their inability to manage their own secretions and inability to partake in the social aspect of oral food intake. All three displayed evidence of clinical depression or suicidal ideation or both. As a result, the use of our techniques is likely to have implications far greater than the provision of nutrition to patients as they address the psychosocial needs of patients suffering from benign esophageal occlusions. This psychological distress appears greater than we have experienced in patients with malignant strictures. This discrepancy is likely due to the prolonged life expectancy and nonpalliative nature of their treatment course.
Multiple factors need to be addressed while managing patients with occlusive esophageal strictures. A multidisciplinary team with expertise in different therapeutic modalities can improve success rates. Further studies are needed to determine if one technique is superior to another regarding the sustainability of esophageal patency.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.