
Abstract
Background:
Guideline-directed medical therapy (GDMT) prolongs survival in patients with heart failure with reduced ejection fraction (HFrEF). However, different countries implement GDMT differently, and many patients are still undertreated. Therefore, this study aimed to assess GDMT utilization in patients with chronic HFrEF at the adult cardiac clinics of three selected hospitals in Addis Ababa, Ethiopia.
Methods:
An explanatory sequential mixed-methods (quantitative cross-sectional followed by qualitative phenomenological) study design was used to assess GDMT usage in patients with HFrEF at the study settings from September 25 to November 25, 2022. Simple random and purposive sampling techniques were used to select participants for the quantitative and qualitative studies, respectively. Adherence level was defined as good (adherence score = 1), moderate (0.5 < score <1), and poor (score ⩽0.5). Quantitative data were analyzed using Statistical Package for the Social Sciences (SPSS) version 26.0. Logistic regression model was used to determine the association. Statistical significance was declared at p < 0.05. Qualitative data were analyzed with MAXQDA 2020.
Results:
Three hundred forty-one patients were included in the quantitative study. Adherence to GDMT was good in 128 (37.5%) of the patients. Patient parameters, including female gender (adjusted odds ratio (AOR) = 0.55, 95% CI: 0.32–0.93), unable to read and write (AOR = 0.31, 95% CI: 0.11–0.86), primary education (AOR = 0.27, 95% CI: 0.12–0.63), were negatively associated with Physicians’ good adherence. Hypertension was associated with lower odds of physicians’ good adherence (AOR = 0.41, 95% CI: 0.21–0.78). Absence of comorbidities (other than hypertension; AOR = 2.65, 95% CI: 1.36–5.15) were positive predictors. System, patient, and physician-related factors were reported as barriers to intensifying GDMT.
Conclusion:
Nearly one-fourth of eligible patients were on ⩽50% of guidelines-recommended drugs. Female gender, educational level, and comorbidities were the factors associated with adherence to GDMT. System, patient, and physician-related reasons for poor adherence were identified. Multipronged interventions are required to address those adherence barriers.
Plain language summary
Introduction
Various international guidelines, including the American College of Cardiology (ACC), the American Heart Association (AHA) and the European Society of Cardiology (ESC), recommend guideline-directed medical therapy (GDMT) to reduce morbidity and mortality in patients with heart failure with reduced ejection fraction (HFrEF).1,2 GDMT is defined as a pharmacotherapy that benefits patients with HFrEF. 3 Thus, initiation of GDMT, including angiotensin-converting enzyme inhibitors (ACEIs) or angiotensin receptor blockers (ARBs) or angiotensin receptor-neprilysin inhibitor (ARNI), beta-blockers (BB), mineralocorticoid antagonists (MRA), and sodium-glucose co-transporter 2 inhibitor (SGLT2i), is considered standard therapy proven to prolong survival and reduce morbidity in individuals with HFrEF. 2 Quick commencement of all core medications followed by titration to target dose (TD) with consideration to patient-specific aspects is crucial. 4 These recommendations are supported by several “landmark clinical trials.”5–12
Despite advancements in pharmacotherapy, morbidity, mortality, and poor health-related quality of life are still high worldwide.13,14 Though the rise in prevalence of mortality due to heart failure (HF) is global, the problem is worse among the elderly and those residing in low sociodemographic index countries. 15 Sub-Saharan Africa faces a critical HF problem, with a mortality rate of 34%—more than twice the global average and over three times that of South America. 16 This grim statistic is attributed to several factors, including the higher prevalence of HFrEF in the population, socioeconomic challenges limiting access to quality healthcare, and insufficient utilization of GDMT. 16
Despite the compelling evidence that displays the benefits of GDMT in HFrEF, several factors obstruct GDMT intensification: patient-related (comorbidities, affordability, side-effect concerns), clinician-related (limited awareness of optimal doses, reluctance to titrate, focus on symptom control, fear of side effects), and system-related (complex reimbursement, limited access to medication and specialists, inadequate support).17–19
In Ethiopia, in-hospital HF mortality was shown to be high. 20 A study showed that the absence of some drugs (spironolactone, ACEI, and statins) was found to be a strong predictor of morality in HF patients. 21 Another Ethiopian study reported under-utilization and sub-optimal dosing of ACEI.22,23 Studies on the utilization of all core pharmacotherapy recommendations in treating HF are limited in Ethiopia.
Thus, the purpose of this study was to evaluate adherence to evidence-based HF treatment guidelines.
Methods and materials
Study design and setting
A hospital-based explanatory sequential mixed-methods (quantitative cross-sectional followed by qualitative phenomenological (explanatory)) study design was carried out at adult cardiac clinics of Tikur Anbessa Specialized Hospital (TASH), St. Peter’s Specialized Hospital (SPH), and St. Paul’s Hospital Millennium Medical College (SPHMMC). Data collection period was from September 25 to November 25, 2022. To report the patients’ medical and medication-related data, a 1-year (September 24, 2021 to September 24, 2022) retrospective record review was conducted.
Adult (⩾18 years old) HF patients diagnosed with chronic HF (EF ⩽40%) and actively followed/treated for ⩾6 months during the study period were included in the study. End-stage HF patients requiring inotropes/mechanical devices/dialysis, with transplant history/plan, acute HF, incomplete records, or lacking consent were excluded. To triangulate the findings, key informants’ interview was conducted with purposively selected physicians from adult cardiac clinics at the selected hospitals during the study timeframe.
Sample size calculation and sampling technique
The sample size was calculated by using the single population proportion sample size formula, considering 36% proportion on GDMT utilization from a previous study among patients with HF (23), 95% CI, 5% margin of error, and the expected number of source population (N = 5746). The final sample size became 350 after applying corrections for small study population and 5% contingency. Of which nine participants were excluded due to incomplete medical records.
The three hospitals (TASH, SPH, and SPHMMC) were purposefully selected due to their cardiac medical service. Proportional allocation was done to each hospitals by dividing the expected number of patients on follow-up (TASH, N = 3366; SPH, N = 1658; SPHMMC, N = 722) during the study period by the total population of the three hospitals (N = 5746) multiplied by the final sample size (n = 350): TASH (n = 205), SPH (n = 101), and SPHMMC (n = 44; Figure 1). A simple random sampling technique (lottery method) was used to select study participants. The nursing appointment logbooks were used as a sampling frame. Patients were recruited randomly into the study during their appointment for medication refilling. For the qualitative study, practicing physicians were approached purposively and asked for a key informant interview using a semi-structured open-ended interview guide regarding barriers to GDMT implementation in the practice setting. Interviews were carried on until information saturation was reached. Thus, seven Physicians were interviewed.

Study population inclusion and exclusion criteria.
Data collection procedures and tools
Three trained pharmacists and nurses were involved in the data collection. The nurses’ role was recruiting the study participants while pharmacists conducted the interview and data abstraction. The data collection tool has two parts: Part I contains demographic characteristics, whereas part II contains parameters used to retrieve clinical and treatment characteristics. While sociodemographic data was collected through a patient interview, other clinical information was collected from the medical record.
After the quantitative data were collected and analyzed, the findings were used to collect qualitative data to explore the reasons for under-usage and under-dosing of GDMT from the physicians’ perspective. Thus, the physicians were interviewed using a semi-structured open-ended interview guide on possible barriers that prevent them from prescribing and up-titrating GDMT. Interviews were audio-taped to be transcribed verbatim. Field notes were also taken during the interview.
Data quality assurance
Data collectors have been trained on study goals and questionnaire completion. Experts assessed face and content validity. A 5% pretest, excluded from the final analysis, was used to ensure questionnaire clarity. Daily supervision ensured complete data collection.
Data interpretation
To assess adherence to GDMT, a global guideline adherence score was calculated. The QUality of Adherence to guideline recommendations for LIFe-saving treatment in heart failure surveY (QUALIFY) adherence score was used to score the adherence.24,25 The score was the ratio of the treatment actually prescribed to the treatment that should have theoretically been prescribed for each of the GDMT classes. The score was calculated for each patient by summing the following points: 0 point for non-prescription in the absence of specified contraindication, 0.5 for those on <50% of target dose (<100% for those on MRA), and 1 point each for the use of ARNI, ACEIs, ARBs, BBs, and MRAs. The score ranged from 0 to 1, and the level of adherence was defined as good (use of all indicated drugs; score = 1), moderate (use of more than half of the indicated drugs; 0.5 < score <1), and poor (use of ⩽50% of the indicated medications; score ⩽0.5). Non-prescription of recommended GDMT in the absence of contraindication was considered to be non-adherence.24,25 Eligibility criteria and algorithm of adherence to GDMT recommended by published guidelines were prepared to decide theoretically recommended class (s) and/or dose of specific GDMT (Table S1 and Figure S1).
Evidence-based target dose attainment was categorized into group 1 (not receiving medications), group 2 (receiving <50% TD), group 3 (receiving 50 to <100% TD), and group 4 (receiving ⩾100% TD).
ESC 2021, AHA/ACC 2017, and Ethiopian standard treatment guideline 2021 were used to assess adherence to GDMT.1,26,27
Data analysis
Statistical Package for the Social Sciences (SPSS) version 26.0, IBM Corp. originally released in 2019, was used for data analysis. Independent variables with variance inflation factor <6 or tolerance test >0.18 were included in the logistic model. Model fitness was tested using Hosmer and Lemeshow’s goodness-of-fit test, yielding a p value of 0.625. The dependent variable was dichotomized into two mutually exclusive parts (better vs poor) in accordance with related studies done elsewhere. When using over 50% of the indicated drugs, the degree of adherence was considered better; when using less than 50%, it was deemed poor.25,28,29 A logistic regression model was applied to identify factors affecting guideline adherence. Variables with p value <0.2 in univariate logistic regression were included in the multivariate logistic regression model to identify predictors of adherence. Association was declared at p < 0.05.
For the qualitative study, thematic analysis was used to categorize clusters of themes after interviews were transcribed verbatim using MAXQDA 2020 qualitative analysis software. 30 The data presentation and reporting were done in accordance with the standards for reporting qualitative research. 31
Reporting guideline: The manuscript followed the STROBE (Strengthening the Reporting of Observational studies in Epidemiology) guidelines of reporting studies for the quantitative study. 32 The manuscript also followed COREQ (Consolidated criteria for reporting qualitative research) checklist to report methods and results of the qualitative study. 33
Operational definitions
GDMT: Indicating pharmacologic treatment alternatives that are acceptable according to clinical practice recommendations. 3
Adherence: Clinicians following guideline recommendations.25,28,29
Good adherence: Use of all the indicated drugs in eligible patients (score = 1)
Moderate adherence: Use of more than half of the indicated drugs; 0.5 < score <1)
Poor adherence: Use of less than half of the indicated drugs in eligible patients (score ⩽0.5)
Better adherence: Use of more than 50% of the indicated drugs (0.5 < score ⩽1), which comprises the good and moderate adherences
HFrEF: Diagnosis of HF with an echocardiography confirmed ejection fraction of ⩽40%
Previous hospitalization: HF hospitalization in the past 12 months.
Results
Sociodemographic characteristics of the study participants
Three hundred fifty patients were approached, and 341 patients agreed to participate in the study, giving a response rate of 97.4%. The mean age of the participants was 53.86 ± 13.37 years. Three-fourth of them (75.7%) were younger than 65 years. Sixty percent of the participants were male. Most of the participants (79.2%) were urban residents. One-fourth (25.2%) of the participants completed secondary education. Two-third (66.3%) of the study participants had health insurance services. Most of the study participants never smoked (89.7%) and were non-alcoholic (88.3%; Table 1).
Sociodemographic characteristics of study participants at the public hospitals, Addis Ababa, Ethiopia, September to November 2022 (n = 341).

Labor worker, religious leader, and student.
According to NIAAA, more than 3 standard drinks per day or more than 7 standard drinks per week for females, and 4 standard drinks per day or 14 standard drinks per week for males will be considered to be alcoholic. 34
ETB, Ethiopian birr; NIAAA, National Institute on Alcohol Abuse and Alcoholism.
Clinical characteristics of the study participants
One-third (33.8%) of the study participants had a history of HF-related hospitalization in the past 1 year. The echocardiography study showed that 197 (57.8%) patients had an ejection fraction of 30%–40% (mean = 29.8 ± 7.4). More than two-third (70.7%) of the patients were in New York Heart Association (NYHA) Functional Classification class II and III HF. Cardiomyopathy and ischemic heart disease (IHD) were the two most common underlying conditions with HF, comprising 47.8% and 40.5%, respectively. Most (72.4%) of the patients had at least one comorbidity. Hypertension and diabetes mellitus were the most common comorbidities, with the frequency of 119 (34.9%) and 97 (28.4%), respectively (Table S2).
Medication characteristics of the study participants
Among 341 patients, 260 (76.2%) took at least five medications with a mean number of 5.92 ± 1.82 drugs. Atorvastatin, aspirin, and furosemide were the most common concomitant cardiovascular drugs prescribed in 245 (71.8%), 233 (68.3%), and 187 (54.8%) of the patients, respectively. The newer drugs, SGLT2i, were prescribed in 39 (11.5%) patients (Table 2).
Medication characteristics of patients with HFrEF attending cardiac clinics of public hospitals, Addis Ababa, Ethiopia, September to November 2022 (n = 341).

HFrEF, heart failure with reduced ejection fraction; Mg, milligrams; SGLT2i, sodium-glucose co-transporter inhibitor.
Adherence status of GDMT
Of the 341 participants, 128 (37.54%) were on all indicated drugs (score = 1) and 96 (28.15%) used ⩽50% of the indicated medications with a maximum score of 0.5 (Figure 2).

Clinicians’ adherence to prescribe and up-titrate GDMT for patients with HFrEF attending cardiac clinics of public hospitals, Addis Ababa, Ethiopia, September to November 2022.
Usage of different GDMTs
From the total study patient prescriptions, 257 (75.37%) of the patients were on the triple foundational drugs of evidence-based pharmacotherapeutic agents for HFrEF, that is, renin nd angiotensin system (RAS) inhibitor + BB + MRA (Figure 3).
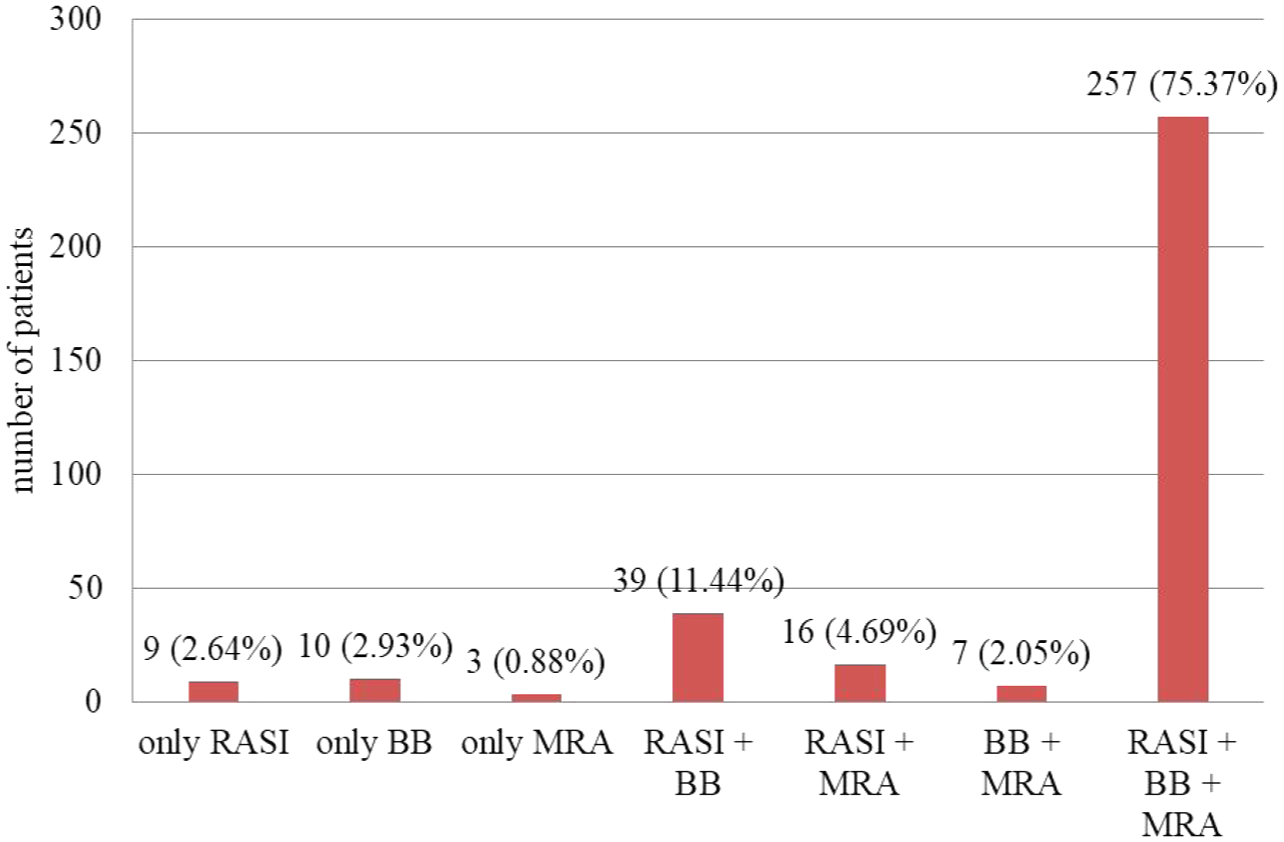
GDMT combinations in patients with HFrEF attending cardiac clinics of public hospitals, Addis Ababa, Ethiopia, September to November 2022 (n = 341).
Usage of GDMT in HFrEF
Among the 341 patients, 318 (93.3%) were eligible for ACEI/ARBs, of which 313 (98.4%) were prescribed any dose of ACEI/ARBs. Regarding ARNIs, only 10 (3.2%) of the eligible patients were prescribed. Among 328 eligible patients, BBs were prescribed to 312 (95.1%) patients. Less than 5% (3.8%) of the patients had contraindications for BB use, among which bradycardia 8 (61.5%) and hypotension 4 (30.8%) were the commonest of all. About 87.5% of the 321 eligible patients were prescribed with MRA (Table 3).
Usage of GDMT in patients with HFrEF attending cardiac clinics of public hospitals, Addis Ababa, Ethiopia, September to November 2022 (n = 341).

ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; ARNI, angiotensin receptor-neprilysin inhibitor; BB, beta-blocker; GDMT, guideline-directed medical therapy; HFrEF, heart failure with reduced ejection fraction; MRA, mineralocorticoid receptor antagonists.
GDMT chosen and dosing
Among 313 patients prescribed with ACEIs/ARBs, 35 (11.2%) were on 100% of the guideline-recommended target doses. Enalapril was the most prescribed ACEI used in 269 (85.9%) of the patients. Among 10 patients prescribed with ARNI, none were taking the TD. Among BBs, metoprolol succinate was prescribed in 285 (91.3%) of 328 eligible patients. Hundred percent 100% of the target dose was achieved in only 13 (4.2%) patients. Among patients prescribed with BB, over half of the patients (52.9%) were taking less than 50% of the recommended target dose. Spironolactone was the only MRA prescribed for 281 (82.4%) patients, with most patients dosed 50 to <100% of the TD (Figure 4).

Target dose attainment of GDMT by individual classes in patients with HFrEF attending cardiac clinics of public hospitals, Addis Ababa, Ethiopia, September to November 2022 (n = 341).
Reasons for not prescribing and not attaining target doses
For most patients, reasons for failure to prescribe or achieve target dose were not documented in the patients’ medical records. Worsening of renal function, 34 (12.2%), was the most common reason prohibiting up-titrating ACEI/ARB up to the target dose. The reason for failure to achieve the TD of the ARNI was unknown in 2 (20%) patients. The reason was unknown for non-prescription and not achieving target dose of MRA in 40 (66.7%) and 211 (88.3%) patients (Table 4).
Reasons for non-prescription and not achieving the target dose of GDMT in patients with HFrEF attending cardiac clinics of public hospitals, Addis Ababa, Ethiopia, September to November 2022 (n = 341).

Peripheral arterial disease, erectile dysfunction, gastrointestinal intolerance and second degree AV node block.
ACEI, angiotensin-converting enzyme inhibitor; AKI, acute kidney injury; ARB, angiotensin receptor blocker; ARNI, angiotensin receptor-neprilysin inhibitor; AV, atrioventricular; BB, beta-blocker; COPD, chronic obstructive pulmonary disease; GDMT, guideline directed medical therapy; HFrEF, heart failure with reduced ejection fraction; MRA, mineralocorticoid receptor antagonist; RF, renal function; TD, target dose.
Factors associated with adherence to GDMT
Multivariable regression analysis results indicated that patient gender, education status, and comorbidity were associated with Physicians’ adherence to GDMT. Female gender of the patients was a negative predictor of Physicians’ better adherence compared to their male counterparts (adjusted odds ratio (AOR) = 0.55, 95% CI: 0.32–0.93). In patients unable to read and write (AOR = 0.31, 95% CI: 0.11–0.86) and who completed primary education (AOR = 0.27, 95% CI: 0.12–0.63), Physicians’ better adherence was less likely as compared to in patients who were diploma holders and above. In addition, hypertension was associated with lower odds of physicians’ good adherence (AOR = 0.41, 95% CI: 0.21–0.78). In individuals without comorbidity, Physicians’ adherence was 2.65 times more likely as compared to those patients with multiple comorbidities (AOR = 2.65, 95%CI: 1.36–5.15; Table 5).
Logistic regression analysis for the factors associated with clinicians’ guideline adherence in the treatment of patients with HFrEF attending cardiac clinics of public hospitals, Addis Ababa, Ethiopia, September to November 2022 (n = 341).
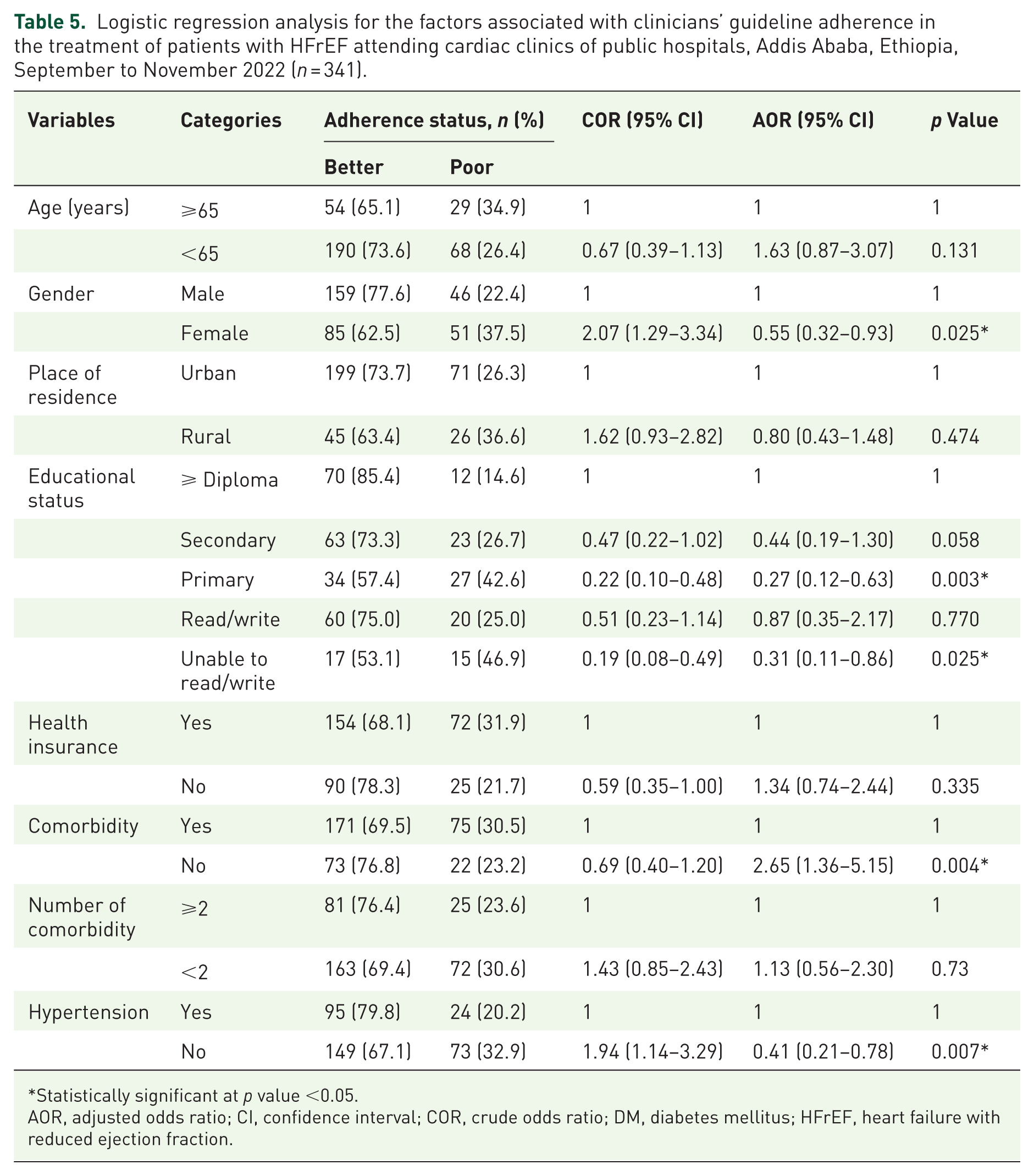
Statistically significant at p value <0.05.
AOR, adjusted odds ratio; CI, confidence interval; COR, crude odds ratio; DM, diabetes mellitus; HFrEF, heart failure with reduced ejection fraction.
Qualitative result
Seven physicians (1 senior cardiologist, 1 cardiology fellow, 3 third-year internal medicine residents, and 2 second-year internal medicine residents) were included for the qualitative study to identify possible barriers that prohibit clinicians from intensification of GDMT in HFrEF patients. Their reasons were clustered into themes using the thematic analysis method with MAXQDA 2020 software. Three themes were constructed: (a) system-related factors, (b) patient-related factors, and (c) physician-related factors (Table 6). The detailed barriers under each theme and subthemes are available in Table S3.
Main themes and subthemes emerged on possible barriers to use and up-titrate GDMT in patients with HFrEF attending cardiac clinics of public hospitals, Addis Ababa, Ethiopia, September to November 2022 (n = 7).

GDMT, guideline-directed medical therapy; HFrEF, heart failure with reduced ejection fraction.
Theme I: System-related factors—System-related factors, like the unavailability of medications and key investigations, understaffed clinics, and a lack of reimbursement or insurance, were barriers emphasized by most of the physicians.
Yeah, except for the ACEI/ARBs, the MRA and BBs, barriers are related to the cost of the medications. (Physician 1) Even in those that were covered by insurance, patients cannot access all medicines in the Kenema pharmacies, so they go to the other branch, and then to another two or three branches, and even may fail to get them after multiple attempts. (Physician 1)
Theme II: Patient-related factors—Some patients are reluctant to adhere to the physician’s plan. Other patient-related barriers include failure to come up with relevant investigations on the follow-up day, inability to afford some medications and/or investigations, and the presence of comorbidities or intolerances.
The ACE inhibitors and ARBs are better titrated to achieve an optimal goal, but the problem again is that our patients will not be available on time because of different reasons. (Physician 4) The first thing, most of the patients don’t want to come early. The earliest time that you can appoint is one month, so you need at least a month, two months, or three months to have an optimal dose of these guidelines directed medical therapies. As I told you before, most of the patients don’t have updated renal function and electrolytes, which make it difficult to up-titrate ACE inhibitors, ARBs, and spironolactone. (Physician 5) In heart failure patients, up-titrating the ACE inhibitors and ARBs might cause or worsen the hyperkalemia in CKD patients. (Physician 1)
Theme III: Physician-related factors—Inertia of previous practice, lack of outcome expectation, fear of side effects, time limits, and lack of awareness were barriers identified under the physician-related theme.
In most of our patients, they are being prescribed at some point, and they will be continued with that same dose rather than up-titrating. (Physician 1) The second barrier is physicians’ fear of side effects because the patient follow-up is not optimal. It is every three or two months. In contrast to guideline recommendations to have patient follow-up every two to three weeks. Our setup is not quite optimal. (Physician 2)
Discussion
In this multicenter study, we assessed the usage and dosing of GDMT, extent of use of GDMT, extent of target dose achievement, factors associated with GDMT use and up-titration, and possible reasons that affect intensification of GDMT in patients with HFrEF.
The result of this study indicates that clinician adherence to GDMT was good, moderate, and poor in 37.5%, 34.3%, and 28.2% of stable outpatients with HFrEF, respectively. Our finding is similar to a previous retrospective study, where good adherence was estimated to be 36%.
23
However, it is lower than the findings of the QUALIFY International Survey, the MAHLER Survey, and the Oman Study.25,28,35 The difference in the country contexts might have contributed to the difference in adherence seen in our study, since low income is directly related to less GDMT usage.
36
Overall, 28.2% had poor global adherence. The level of adherence was lower than the findings of a study conducted in Korea, which indicated that poor adherence was seen in only 12.8% of the prescriptions.
29
System-related, patient-related, and physician-related factors might be the possible contributing factors for such a low adherence level in our study, as stated by interview respondents: This is mainly due to: one, the drugs are not readily available, and even if they are available in certain pharmacies, they are expensive, so our patients usually cannot afford them, which is why we don’t usually prescribe them. (Physician 3) One is lack of regular follow-up; the other is lack of investigations like renal function tests and electrolytes upon follow-up day. (Physician 7) I think it won’t be physicians’ knowledge gaps but rather inertia. The other is physician inertia, which is common for all of the drugs in prescribing and dosing. The patient’s and physician’s inertia can be solved by time and training. (Physician 2)
Among patients who met the criteria for ACEI/ARBs and BBs, prescription rates at any dose were 98.4% and 95.1%, respectively. This is higher than a report from the United States, ACEI/ARB were prescribed in 81.4% and BBs in 94.4% of HFrEF patients.
37
However, the finding is in line with a Canadian study.
38
The rates of RAS inhibitor use in our setting were higher than the findings reported from the Oman study.
35
The reason for such a huge difference in the prescription rate of RAS inhibitors might be due to the effect of the low ARNI prescription rate in their study. In our study, the ARNI prescription rate was reported separately from other RAS inhibitors (ACEI/ARB). Only 3.2% of the eligible patients were prescribed ARNI, which is lower than the result reported from the US study of 27%.
37
The possible reason might be less availability and affordability of ARNI in our settings. Most eligible patients were prescribed MRA. This is higher than that reported from studies done in Turkey and in the United States, with 55.4% and 54% prescription rates, respectively.17,37 It is not surprising, since spironolactone is less costly and easily available in our settings and in patients with low income, it is prescribed to every eligible patient unless there is clinical inertia.
The MRA (spironolactone) is accessible, and it is cheap even for the patient not having insurance. So in this case, if it is not prescribed, it might be due to our knowledge gap. (Physician 1) MRA, ACE inhibitors, or ARBs are better prescribed. If there is a barrier, it is only the follow-up, organ function tests like renal function tests and serum potassium; otherwise, they are better prescribed. (Physician 4) We usually adhere to prescribing and escalating beta-blockers based on the guidelines unless there are contraindications like asthma, some other chronic obstructive airway disease, or low blood pressure. Usually we refrain from titrating up when patients have low or borderline blood pressure or bradycardia; we just continue or even deescalate rather than titrating up. (Physician 3)
Evidence-based target doses of ACEI/ARBs were achieved in only 11.1% of the patients prescribed with these agents. This is lower than the Italian study, where the target dose was achieved in 27.9% of patients.
25
The target dose for ARNI (sacubitril/valsartan) was not achieved in all patients in contrast, in the report from the CHAMP-HF registry, 9.9% of patients prescribed with ARNI were on the target dose.
39
The low prescription rate and underdosing of sacubitril/valsartan might result from inadequate availability due to the late arrival of these agents in this country, together with cost issues. Including this low prescription rate in the final analysis may underestimate the overall adherence score as well as clinicians’ efforts. Relative to ACEI/ARB, ARNI, and BB, target dose achievement was better with MRA. But our finding is very low compared to the Oman study, in which 94% of patients taking MRA were on the target dose.
35
When compared to a meta-analysis comprising many studies, the target dosage accomplishment of ARNI and spironolactone was lower, whereas ACEI/ARB and BB were within the range.
40
Regarding the ACE inhibitors or ARBs, usually patients come without investigations like renal function tests or electrolytes. Without those things, it is difficult to up-titrate the ACE inhibitors, or ARBs, or ARNIs, for that matter. (Physician 5) But because of the expensiveness of the ARNIs and SGLT2 inhibitors, most of our patients are taking less optimal guideline-guided recommendations. (Physician 5) Due to the fact that most clinicians fear causing hypotension, they will usually not up titrate for patients with borderline blood pressure, which is around eighty-five to 60 or 55 mmHg. (Physician 1)
In our study, female gender was a negative predictor of better adherence to GDMT. Other studies have also reported this.41,42 However, in the Canadian study, female gender had no association with guideline adherence.
38
Consistent with a study from China, we found a significant association between lower levels of education with poor adherence.
36
Patients’ educational status may directly affect their information and decision-making abilities regarding their treatment. Indeed, in our qualitative analysis, a contributing factor to the patient-related factor was identified as one of the reasons for non-adherence.
Some of our patients don’t know their diagnosis or why their drugs are up-titrated. So whenever we make a diagnosis, we have to tell our patients. Knowing the diagnosis and the benefit of the drug will make the patients more realistic, more involved in their disease, and more likely to purchase these drugs. (Physician 5) Most of our patients don’t want to increase the dose of the drug unless they have some symptoms because they believe that “we are ok now so that we will increase the dose this month or for the next month” is the common term used by the patients. These are inertias from the patient side. (Physician 2)
Patients with hypertension were significantly less likely to receive good GDMT prescription adherence compared to those without hypertension. This might be due to the complexity in the management of the comorbidities. Thus, the Physicians might not merely depend on guidelines, rather case-by-case clinical decisions might be applied. In contrast, a study from the Netherlands’ study showed an association between hypertension and GDMT use.
43
In fact, hypertension experience or related awareness was found to promote medication adherence for other comorbidities like HF.
22
In addition, hypertension comorbid patients are less prone to drug-related hypotension, which is a common barrier to prescribing and up-titrating most of the GDMT, as articulated by interview respondents: The first thing is, most of the patients have borderline blood pressure due to the reduced ejection fraction. Due to most of the clinicians fear causing hypotension so usually they will not up titrate in patients having borderline blood pressure. (Physician 1) And the only thing that may hinder is patients being bradycardic or hypotensive. (Physician 4) The other thing is the side effect of the medications can be the barriers because it can cause bradycardia and hypotension. (Physician 7)
Absence of other multiple comorbidities was associated with better adherence. Patients with more comorbidity, specifically asthma, chronic obstructive pulmonary disease, or cardiac arrhythmias, were more difficult to treat in a German study.
44
It might, in part, result from the presence of other comorbidities like kidney problems and asthma/COPD, which are known reasons for RAS inhibitor and BB non-use, respectively. Evidently, pill burden in comorbid patients increases the risk of drug-drug interactions and adverse reactions. As such, physicians may refrain from prescribing or up-titrating medications in accordance with guidelines. The interview respondents, indeed, noted this: The other thing is the issue of renal dysfunction, especially in CKD patients. In heart failure patients, up-titrating the ACE inhibitors and ARBs might cause or worsen the hyperkalemia in CKD patients. (Physician 1) Patients may have renal impairment, or patients may have hyperkalemia and other electrolyte disturbances. So as not to get worse, we may refrain from titrating up these drugs. (Physician 3)
However, the actual reasons physicians did not follow guideline recommendations were difficult to determine from registries because patient-level data on roughly comparable contraindications, previous medication trials, and patient preferences were not systematically collected. However, due to inadequate documentation, identifying all the possible reasons for non-adherence from patient chart review is difficult. Moreover, by considering variations in different settings, we tried to let the physicians identify possible reasons for non-adherence to GDMT recommended by evidence-based guidelines. Thus, the qualitative study approach was employed. The qualitative findings of this study revealed that system-related factors, patient-related factors, and physician-related factors were identified as possible reasons for inadequate GDMT usage and dosing (Table S3). This finding is in line with the findings reported in a review article. 40
Our study has some limitations. Exclusion of patients without an appointment for follow-up and missing values are possible selection bias. However, the reason is the inclusion of only public hospitals was due to the availability of cardiac clinics/services in these hospitals, unlike the private hospitals and any other public hospitals in the study area that do not have separate cardiac clinic. The mixed-methods approach allowed us to incorporate qualitative insights, providing a richer understanding of the quantitative data. The bias due to possible medical record incompleteness (especially for actual reasons for physicians’ non-adherence to GDMT) was managed with triangulation using qualitative exploration through Physicians’ interviews. No power analysis was done due to resource constraints, but the results were interpreted cautiously by taking into consideration this limitation. Future studies might consider expanding the sample size or exploring additional variables to further validate our findings. Nonetheless, this study is the first to assess the usage and dosing of GDMT and barriers negating the good adherence of clinicians to prescribe and up-titrate GDMT in patients with HFrEF in Ethiopia using a mixed-methods multicenter approach.
Conclusion
Our findings revealed that nearly one-fourth of eligible patients with HFrEF are still on less than 50% of the indicated drugs. Large disparities were found in GDMT utilization, especially target dose attainment. Reasons regarding the low prescription rate and failure to up-titrate the dose of GDMT were poorly documented in the patients’ charts. However, the study tried to explore such reasons through a qualitative method. Patient parameters, including female gender and having lower educational levels, were negatively associated with Physicians’ better adherence. The presence of hypertension and the absence of other comorbidities were associated with Physicians’ better adherence. Healthcare delivery system, patient, and physician-related factors were reported as causes of poor adherence.
Multipronged interventions are required to address the barriers to attaining GDMT. We recommend hospitals to initiate dose optimization, establish a dedicated GDMT clinic, and develop a harmonized practical institutional protocol or an algorithm to improve pharmacotherapy of patients with HFrEF. Efforts from policymakers to ensure the availability of these essential HF medications are required. In addition, patient education regarding their treatment can help improve patient-related factors influencing GDMT intensification. Further studies to assess the outcomes associated with GDMT usage are also recommended.
Supplemental Material
sj-docx-1-tak-10.1177_17539447251411121 – Supplemental material for Evaluating the implementation of guideline-directed medical therapy in the treatment of chronic heart failure at public hospitals in Ethiopia
Supplemental material, sj-docx-1-tak-10.1177_17539447251411121 for Evaluating the implementation of guideline-directed medical therapy in the treatment of chronic heart failure at public hospitals in Ethiopia by Akalu Fetene, Amsalu Degu, Chalelgn Kassaw, Chala Fekadu Oljira, Kale Gubae, Tariku Shimels and Getachew Alemkere in Therapeutic Advances in Cardiovascular Disease
Supplemental Material
sj-docx-2-tak-10.1177_17539447251411121 – Supplemental material for Evaluating the implementation of guideline-directed medical therapy in the treatment of chronic heart failure at public hospitals in Ethiopia
Supplemental material, sj-docx-2-tak-10.1177_17539447251411121 for Evaluating the implementation of guideline-directed medical therapy in the treatment of chronic heart failure at public hospitals in Ethiopia by Akalu Fetene, Amsalu Degu, Chalelgn Kassaw, Chala Fekadu Oljira, Kale Gubae, Tariku Shimels and Getachew Alemkere in Therapeutic Advances in Cardiovascular Disease
Supplemental Material
sj-docx-3-tak-10.1177_17539447251411121 – Supplemental material for Evaluating the implementation of guideline-directed medical therapy in the treatment of chronic heart failure at public hospitals in Ethiopia
Supplemental material, sj-docx-3-tak-10.1177_17539447251411121 for Evaluating the implementation of guideline-directed medical therapy in the treatment of chronic heart failure at public hospitals in Ethiopia by Akalu Fetene, Amsalu Degu, Chalelgn Kassaw, Chala Fekadu Oljira, Kale Gubae, Tariku Shimels and Getachew Alemkere in Therapeutic Advances in Cardiovascular Disease
Supplemental Material
sj-docx-4-tak-10.1177_17539447251411121 – Supplemental material for Evaluating the implementation of guideline-directed medical therapy in the treatment of chronic heart failure at public hospitals in Ethiopia
Supplemental material, sj-docx-4-tak-10.1177_17539447251411121 for Evaluating the implementation of guideline-directed medical therapy in the treatment of chronic heart failure at public hospitals in Ethiopia by Akalu Fetene, Amsalu Degu, Chalelgn Kassaw, Chala Fekadu Oljira, Kale Gubae, Tariku Shimels and Getachew Alemkere in Therapeutic Advances in Cardiovascular Disease
Supplemental Material
sj-docx-5-tak-10.1177_17539447251411121 – Supplemental material for Evaluating the implementation of guideline-directed medical therapy in the treatment of chronic heart failure at public hospitals in Ethiopia
Supplemental material, sj-docx-5-tak-10.1177_17539447251411121 for Evaluating the implementation of guideline-directed medical therapy in the treatment of chronic heart failure at public hospitals in Ethiopia by Akalu Fetene, Amsalu Degu, Chalelgn Kassaw, Chala Fekadu Oljira, Kale Gubae, Tariku Shimels and Getachew Alemkere in Therapeutic Advances in Cardiovascular Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.