
Abstract
Cardiovascular (CV) disease is a major cause of morbidity and mortality in the developing and the developed world. Mortality from CV disease had plateaued in the recent years raising concerning alarms about the sustained efficacy of available preventive and treatment options. Heart failure (HF) is among the major contributors to the CV-related health care burden, a persisting concern despite the use of clinically proven guideline-directed therapies. A requirement for more efficient medical therapies coupled with recent advances in bio-innovation led to the creation of sacubitril/valsartan, an angiotensin receptor-neprilysin inhibitor (ARNI), which demonstrated substantial CV benefit when compared with the standard of care, enalapril, in patients with HF and reduced ejection fraction. Further investigations of this novel combination ARNI at the tissue level shed light into the anti-remodeling and cardioprotective effects of sacubitril/valsartan, while clinical studies in the phenotypes of HF with preserved ejection fraction, hypertension and subsets, coronary outcomes, postmyocardial infarction, and renal disease suggested that this combination could be beneficial across a wide spectrum of CV disease. Sacubitril/valsartan is a much-needed therapeutic advance in the avenue of CV disease.
Keywords
Introduction
Cardiovascular (CV) disease is a major cause of morbidity and mortality in the developing and the developed world, and represents a major barrier to sustainable human development.1,2 In 2015, there were an estimated 422.7 million cases of CV disease and 17.92 million CV disease-related deaths around the world. 1 Although mortality from CV disease declined between 1990 and 2015, it had plateaued in recent years, raising concerning alarms about the sustained efficacy of available preventive and treatment advances over these years. 1 Ischemic heart disease, cerebrovascular disease, cardiomyopathy and heart failure (HF), and hypertension among other,s represent major forms of CV disease.1,2
HF is growing in epidemic proportions and has a current estimated prevalence of 5.8 million in the United States of America (USA) and over 23 million people worldwide.2,3 The last century witnessed significant progress in recognizing the neurohormonal systems responsible for the development and progression of HF including the sympathetic nervous system (SNS) and the renin-angiotensin-aldosterone system (RAAS). 4 The complex pathophysiological interactions between the SNS and the RAAS and the importance of their modulation in the development, progression, and treatment of HF were well described. Neuroendocrine modulation with beta-adrenergic blockers targeting the SNS; angiotensin-converting enzyme (ACE) inhibitors (ACEIs), angiotensin receptor blockers (ARBs), and mineralocorticoid receptor antagonists (MRAs) targeting the RAAS have become the cornerstone of medical therapy for chronic HF with reduced ejection fraction (HFrEF) to reduce morbidity and mortality. 4 Despite the use of these standard therapeutic agents, HF remains to be associated with significant morbidity, mortality, and healthcare expenditure.2,3
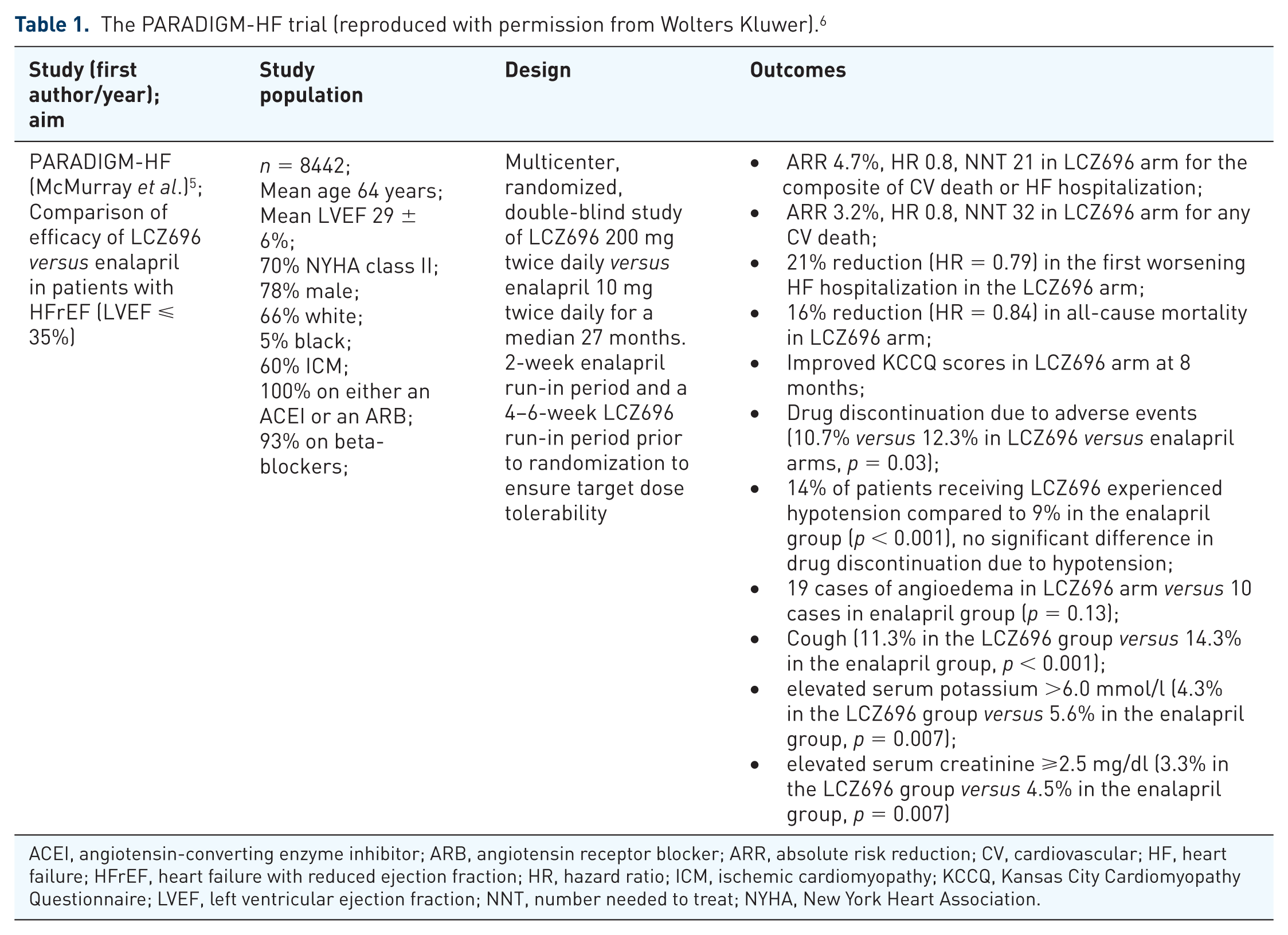
Increasing necessity for more efficient medical therapies combined with advances in pharmaco-innovation have led to the creation of an angiotensin receptor-neprilysin inhibitor (ARNI), which in the recent landmark PARADIGM-HF (Prospective Comparison of Angiotensin Receptor- Neprilysin Inhibitor with Angiotensin-Converting Enzyme Inhibitor to Determine Impact on Global Mortality and Morbidity in Heart Failure) trial showed compelling evidence for the CV benefit of sacubitril/valsartan when compared with the standard of care, enalapril, in patients with HFrEF; Table 1. 5 Further investigations of this novel combination ARNI at the tissue level shed light into the anti-remodeling and cardioprotective effects of sacubitril/valsartan, while studies in the clinical phenotypes of HF with preserved ejection fraction (HFpEF), hypertension and subsets, coronary outcomes, postmyocardial infarction (MI state), and renal disease, suggested that this combination could be beneficial across a wide spectrum of CV disease. In this article we briefly discuss the initial efforts directed at natriuretic peptide (NP) system (NPS) augmentation to manage HF, the landmark PARADIGM-HF trial, evidence for the efficacy of sacubitril/valsartan in various other CV conditions, and current guidelines recommending this drug in the management of HF patients.
The PARADIGM-HF trial (reproduced with permission from Wolters Kluwer). 6
ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; ARR, absolute risk reduction; CV, cardiovascular; HF, heart failure; HFrEF, heart failure with reduced ejection fraction; HR, hazard ratio; ICM, ischemic cardiomyopathy; KCCQ, Kansas City Cardiomyopathy Questionnaire; LVEF, left ventricular ejection fraction; NNT, number needed to treat; NYHA, New York Heart Association.
Initial efforts at NP system augmentation
In contrast with the detrimental CV effects of SNS and RAAS stimulation, activation of the NPS appeared to have a beneficial role in the treatment and prevention of progression of HF via their vasodilatory and anti-remodeling effects. 4 Initial efforts to augment the NPS focused on exploiting the vasodilatory action of NP via intravenous (IV) NP infusions in patients presenting with acute HF. Nesiritide, the recombinant human B-type NP (BNP), was extensively evaluated in this population.7–11 Although initial investigations of IV nesiritide infusion showed promising clinical benefits in acute HF patients, further larger clinical studies failed to show sustained improvements in clinical markers of HF, mortality, and readmissions.7–11 Similar disappointing findings were seen in more recent clinical trials evaluating ularitide, an A-type NP (ANP) homolog.12–14 Neprilysin (NEP) is a neutral endopeptidase responsible for the degradation of endogenous NPs. 15 Although NEP inhibition represented an approach to augment endogenous NP activity, studies of lone NEP inhibitors (NEPIs) did not show significant clinical benefit in patients with chronic HF or essential hypertension.16–20 In addition to degrading NPs, NEP also inhibited various vasodilator and vasoconstrictor peptides.4,21 NEPI led to disinhibition of potent vasoconstrictor peptides like angiotensin I and II, thereby potentiating the RAAS and resulting in neutralization of the clinical advantage expected with NP augmentation.4,20,21
With the failure of lone NEP inhibition, studies were designed to evaluate combination ACEI-NEPI in chronic HF and hypertensive patients. 4 The rationale behind using this combination vasopeptidase inhibitor (omapatrilat) is to augment endogenous NPs with the NEPI component while simultaneously causing ACEI-mediated inhibition of the vasoconstrictor peptides angiotensin I and II which were activated by the NEPI.4,22 Compared with the standard of care, enalapril, omapatrilat treatment showed a modest reduction in all-cause mortality and HF-related hospitalizations in chronic HF patients. 23 However, further development of this drug was stalled because of an observed higher frequency of angioedema with omapatrilat compared with enalapril in a large group of hypertensive patients, particularly smokers and African Americans. 24 Omapatrilat treatment led to a large increase in the levels of bradykinin by inhibiting multiple enzymes responsible for bradykinin degradation (ACE, NEP, and aminopeptidase) thereby causing angioedema. 4
NP infusion, lone NEP inhibition, and combination ACEI-NEPI were three unsuccessful attempts at NPS augmentation to benefit HF and hypertensive patients. To overcome the angioedema-related safety concerns observed with the ACEI-NEPI combination, a NEPI was combined with an ARB to create LCZ696, the first ARNI. 25 The combination of an ARB and NEPI would inhibit the RAAS and enhance the NPS without inhibiting ACE involved in bradykinin degradation. By using the ARNI combination, endogenous bradykinin would be metabolized by the uninhibited ACE, thereby minimizing the risk of angioedema. 4
Sacubitril/valsartan
LCZ696, the first-in-class ARNI is a 1:1 combination of valsartan (an ARB) and sacubitril (AHU377; prodrug of the NEPI - LBQ657). 25 LCZ696 is an orally active medication, which upon ingestion resulted in an almost simultaneous increase in plasma concentrations of valsartan, sacubitril and its active moiety LBQ657. 25 Clinical and laboratory data from preclinical investigations of this novel combination suggested simultaneous NEP inhibition and angiotensin receptor blockade while also providing evidence on its safety and tolerability.25,26 Favorable findings from these early studies paved way for the evaluation of sacubitril/valsartan in various CV disorders, largely in hypertensive and HF patients. Actions of LCZ696 on the CV system are briefly outlined in Figure 1.

Neurohormonal interactions in heart failure and their role in contributing to the progression of heart failure.
Sacubitril/valsartan in HF
HFpEF
The earliest clinical data on the safety and efficacy of LCZ696 in HF patients comes from the PARAMOUNT (Prospective comparison of ARNI with ARB on Management Of heart failUre with preserved ejectioN fracTion) trial. 27 This phase II proof-of-concept study randomized 301 New York Heart Association (NYHA) class II–IV chronic HFpEF patients with baseline elevated N-terminal pro B-type NP (NT-proBNP) levels in a double-blind fashion to a 12-week treatment with LCZ696 or valsartan and evaluated changes in NT-proBNP levels. 27 At 12 weeks, NT-proBNP was significantly reduced in the LCZ696 group [hazard ratio (HR) = 0.77, p = 0.005], an effect which was independent of the antihypertensive effects of this combination drug.27,28 The LCZ696 treated group had improved troponin levels and preserved renal function while adverse events were similar in both treatment groups.27,29,30 At 36 weeks, improvements in left atrial size and NYHA functional class were evident in the LCZ696-treated group. 27 Findings from this study demonstrated the safety of this combination and its beneficial effects on myocardial damage and left atrial remodeling which are important pathophysiologic changes in the HFpEF phenotype.
The current phase III PARAGON-HF (Prospective comparison of angiotensin receptor-neprilysin inhibitor with ARB Global Outcomes in HF with preserved ejection fraction) trial [ClinicalTrials.gov identifier: NCT01920711] of around 4800 HFpEF patients with elevated baseline NT-proBNP levels is evaluating the effects of sacubitril/valsartan versus valsartan on the primary composite outcome of CV death and HF hospitalizations and is expected to finish in 2019 (Table 2). 31 The randomized, double-blind controlled study comparing LCZ696 with medical therapy for comorbidities in HFpEF patients (PARALLAX) is currently recruiting participants to demonstrate the superiority of LCZ696 over individualized medical therapy for comorbidities (with enalapril, valsartan, or placebo) in reducing NT-proBNP levels and improving HF symptoms and functional capacity in HFpEF patients (Table 2). 32
Currently undergoing clinical trials of sacubitril-valsartan.

ADHF, acute decompensated heart failure; BID, twice daily; BNP, B-type NP; c-GMP, cyclic-guanosine monophosphate; CKD, chronic kidney disease; CSS, symptoms and physical limitations; CV, cardiovascular; eGFR, estimated glomerular filtration rate; ESRD, end stage renal disease; HF, heart failure; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; IADL, instrumental activities of daily living; ICU, intensive care unit; KCCQ, Kansas City Cardiomyopathy Questionnaire; LAVI, left atrial volume index; LV, left ventricle; LVEF, left ventricular ejection fraction; MI, myocardial infarction; MRI, magnetic resonance imaging; N, number of patients in the trial; NP, natriuretic peptide; NT-pro BNP, N-terminal pro-brain natriuretic peptide; NYHA, New York Heart Association; RCT, randomized controlled trial; SUVr, standardized uptake value ratio.
HFrEF
Safety and efficacy data from the PARAMOUNT trial and other phase III randomized trials of LCZ696 in hypertensive patients led to the evaluation of sacubitril/valsartan in a large group of chronic HFrEF patients in the landmark PARADIGM-HF trial.5,27,41,42 The PARADIGM-HF was a phase III, randomized, double-blind, controlled trial of 8442 patients with NYHA class II–IV HF, left ventricular ejection fraction (LVEF) ⩽40% (later amended to ⩽35%), and elevated BNP or NT-proBNP levels to receive twice daily dosing of either 200 mg of LCZ696 or 10 mg of enalapril in addition to standard medical therapy for HF (Table 1). 5 Eligible patients had to be on a stable dose of an ACEI or an ARB that was the therapeutic equivalent of 10 mg of enalapril daily for at least 4 weeks prior to entry into the trial. 5 The primary endpoint was a composite of death from CV causes or hospitalization for HF. 5 The study was terminated early after a median follow up of 27 months because the significant CV benefit in the LCZ696 treated group met the prespecified cutoff for an immense clinical benefit. 5
At the 27-month follow up, LCZ696 was associated with a 20% decrease in the composite primary endpoint compared with enalapril (HR = 0.80, p < 0.001). 5 Additionally, LCZ696 reduced death from any CV cause by 20% (HR = 0.8, p < 0.001), first hospitalization for worsening HF by 21% (HR = 0.79, p < 0.001), all-cause mortality by 16% (HR = 0.84, p < 0.001), and prevented deterioration of symptoms and quality of life as measured on the Kansas City Cardiomyopathy Questionnaire (Table 1). 5 Overall, 14% of patients receiving LCZ696 experienced hypotension compared with 9% in the enalapril group (p < 0.001). 5 However, the number of patients who discontinued therapy due to hypotension was not significantly different (0.9% in the LCZ696 group versus 0.7% in the enalapril group). 5 Nonserious angioedema occurred more frequently in the LCZ696 group although the difference was not significant (19 cases versus 10 cases in the enalapril group). 5 Other important adverse effects are discussed in Table 1.
Numerous post-hoc analyses have demonstrated the superiority of sacubitril/valsartan over enalapril irrespective of age, systolic blood pressure (BP), LVEF, baseline HF risk scores, glycemic status, and the presence of an intracardiac device.43–48 LCZ696 exhibited additional clinical benefit over enalapril in HF patients by attenuating progression of the HF disease process. 49 Patients taking sacubitril/valsartan had early and sustained reduction in biomarkers of myocardial wall stress and injury (NT-proBNP and troponin) and increased plasma BNP levels versus enalapril. 49 Fewer LCZ696-treated patients required intensification of medical treatment for HF or an emergency department visit for worsening HF. 49 Putative placebo analysis of LCZ696 using results from previous landmark placebo-controlled trials of RAAS blockade in HF showed significantly greater reductions in CV death, HF hospitalization, and all-cause mortality with LCZ696. 50 More recent analyses have demonstrated that the clinical benefit of sacubitril/valsartan combination in HFrEF was not affected by differences in sex, geographic variations, and etiology of HF (ischemic and nonischemic).5,51,52
Several questions and concerns have been raised by clinicians and researchers regarding the generalizability of the PARADIGM-HF trial results with regards to the study design, the effect of achieved target dose of medications on clinical outcomes, study population representativeness of the real-world HFrEF patients, and the effect of ethnic and geographic variations on outcomes.6,53 Most of these concerns were answered in post-hoc analyses and addressed in expert review articles.53,54 Ongoing clinical trials will evaluate the safety and efficacy of sacubitril/valsartan and its effects on clinical and exercise-related outcomes, biomarker changes, and cardiac remodeling parameters in HFrEF patients in the acute HF, post-MI HF, and in those with left ventricular assist devices (Table 2). As patients with advanced heart failure were poorly represented in the PARADIGM-HF trial, an ongoing trial in symptomatic advanced HFrEF patients will determine if treatment with LCZ696 compared with valsartan for 24 weeks will improve NT-proBNP levels to reflect hemodynamic and clinical status. 55 A study has been planned to evaluate the safety and efficacy of sacubitril/valsartan in the pediatric HF population and is currently recruiting. 56
Sacubitril/valsartan and coronary outcomes
ACEIs and ARBs have been shown to improve outcomes in acute MI patients, findings which triggered the evaluation of the coronary outcomes of sacubitril/valsartan. 57 A post-hoc analysis of the PARADIGM-HF evaluated the effect of sacubitril/valsartan compared with enalapril on the primary composite outcome of CV death and HF hospitalization. 57 A secondary outcome evaluated was the coronary composite of CV death, nonfatal MI, angina hospitalization or coronary revascularization. Compared with enalapril, sacubitril/valsartan reduced the risk of the primary outcome (HR 0.80, p < 0.001) as well as the coronary composite (HR 0.83, p < 0.001). 57 Although each of the components of the coronary composite outcome occurred less frequently in the sacubitril/valsartan-treated group compared with the enalapril group, only CV death was reduced significantly with LCZ696 treatment. 57 Findings from this post-hoc analysis suggest an interesting possibility that LCZ696 might decrease the occurrence of atherothrombotic events as well as HF events. To validate this hypothesis, the phase III, randomized controlled PARADISE-AMI (Prospective ARNI versus ACE Inhibitor Trial to DetermIne Superiority in Reducing Heart Failure Events After MI) study is currently recruiting post-acute MI patients without prior chronic HF, with LVEF < 40%, or pulmonary congestion at the time of randomization. 37 This trial will evaluate the benefit of sacubitril/valsartan versus ramipril in reducing the occurrence of the primary composite endpoint of CV death, HF hospitalization, and outpatient HF (time to first event analysis). 37 Secondary endpoints include a composite of CV death, nonfatal spontaneous MI or nonfatal stroke (Table 2). 37
Sacubitril/valsartan after acute MI
Coronary artery disease and MI are important and common causes of HF in the western world. Post- MI cardiac remodeling has a major role to play in the development of HF which then progresses with continued cardiac remodeling. In experimental animal models of HFrEF, LCZ696 ameliorated cardiac remodeling and improved LVEF compared with vehicle and valsartan.58,59 These effects were hypothesized to be from ARNI-mediated inhibition of hypertrophy and fibrosis and suppression of local transforming growth factor-β by the sacubitril moiety of LCZ696.58,59 These data encouraged researchers to investigate the cardioprotective effects of sacubitril/valsartan in the short-term phase after an acute MI.
A recent study utilized a systems biology approach to understand the mechanism of action of sacubitril/valsartan on cardiac remodeling. 60 Myocardial transcriptome obtained in response to MI in swine was analyzed to study post-MI ventricular remodeling. 60 An artificial neural network analysis revealed that sacubitril/valsartan acts synergistically against cardiomyocyte cell death and left ventricular extracellular matrix remodeling. 60 Valsartan improved cardiac remodeling, while sacubitril attenuated cardiomyocyte cell death, hypertrophy, and impaired myocyte contractility. 60 In a mice-model of experimental acute MI randomized to vehicle, enalapril, or LCZ696 treatment 1 day after the MI, LCZ696 significantly suppressed the production of proinflammatory cytokines, matrix metalloproteinase-9 activity and aldosterone, while enhancing NPs. 61 These findings provide a mechanistic insight into the cardioprotective effects of LCZ696 against acute MI. 61 The clinical implications of these findings are being evaluated in the PARADISE-AMI trial. 37
Sacubitril/valsartan in essential hypertension
Initial evaluation of sacubitril/valsartan before the PARADIGM-HF trial included two phase III industry-sponsored studies in hypertensive patients. A proof-of-concept trial in 1328, mostly white, mild-to-moderate hypertensive patients demonstrated that compared with valsartan or AHU377 alone, sacubitril/valsartan treatment for 8 weeks provided additional reduction of BP without any cases of angioedema or other serious adverse effects attributable to the study drug. 41 There was a reduction in mean sitting diastolic BP across the doses of sacubitril/valsartan compared with valsartan (2.17 mmHg, p < 0.0001). 41 Data from this study showed that reduction in systolic, diastolic, and pulse pressures, both sitting and ambulatory, was greater with LCZ696 than with either valsartan or AHU377. 41
A similarly designed trial in 389 mild-to-moderate hypertensive Asian patients demonstrated the efficacy of sacubitril/valsartan in reducing BP in a dose-dependent manner compared with valsartan without reporting any cases of angioedema. 42 Analysis of PARADIGM-HF showed a mean reduction in systolic BP of 3.2 ± 0.4 mmHg from baseline at randomization in participants receiving sacubitril/valsartan compared with enalapril (p < 0.001). 5 A small study in Asian patients with severe hypertension (mean systolic BP 173.4 mmHg, mean diastolic BP 112.4 mmHg) demonstrated the efficacy of sacubitril/valsartan in reducing mean systolic/diastolic BP by 35.3/22.1 mmHg at 8 weeks. 62 Sacubitril/valsartan has also been shown to be well tolerated and efficacious as an add-on therapy to amlodipine in Asian patients with systolic hypertension which was not adequately controlled with amlodipine. 63
Hypertension subsets
Arterial stiffness
In the PARAMETER (Prospective Comparison of Angiotensin Receptor Neprilysin Inhibitor With Angiotensin Receptor Blocker Measuring Arterial Stiffness in the Elderly) study, sacubitril/valsartan demonstrated efficacy in reducing arterial stiffness in the elderly with systolic hypertension and pulse pressure >60 mm Hg indicative of arterial stiffness. 64 At 12 weeks, sacubitril/valsartan reduced central aortic systolic pressure by 3.7 mmHg more than olmesartan (an ARB) (p = 0.01) and reduced mean 24-hour ambulatory brachial and central aortic systolic pressure by 4.1 mmHg and 3.6 mmHg respectively (p < 0.001). 64 Although BP parameters were similar between groups at 52 weeks, more patients in the olmesartan group required add-on antihypertensives. 64 NEP inhibition is postulated to be responsible for the additional BP-lowering effects of sacubitril/valsartan and these interesting findings may lead to newer approaches in risk factor modification in elderly patients with arterial stiffening which has been shown to be a predictor of adverse CV effects, stroke, chronic kidney disease (CKD) and HF.
Salt-sensitive hypertension
Sacubitril/valsartan has been shown to be more efficacious in salt-sensitive hypertension compared with valsartan alone with a significant increase in natriuresis and diuresis on day 1 and greater reductions in office and ambulatory BP on day 28. 65
Obesity and hypertension
Sacubitril/valsartan, via its NP augmenting and angiotensin receptor blockade activity, has been hypothesized to improve insulin sensitivity and have beneficial pleiotropic effects on glucose and lipid metabolism. 66 In a recent study in obese patients with hypertension randomized to receive either sacubitril/valsartan or amlodipine, sacubitril/valsartan-treated patients had significant increases in the insulin sensitivity index and abdominal adipose tissue interstitial glycerol concentrations. 66 These benefits in addition to the antihypertensive efficacy of sacubitril/valsartan are promising and further studies are needed to elucidate the clinical meaning of these findings.
Hypertension and CKD
Hypertension is both a cause and complication of CKD. The BP-lowering effects of sacubitril/valsartan was studied in a small group of Japanese patients with hypertension and CKD [estimated glomerular filtration rate (eGFR) between 15 to 60 ml/min/1.73 m2]. 67 After 8 weeks, mean sitting systolic/diastolic BP reduced by 20.5 ± 11.3/8.3 ± 6.3 mmHg from baseline. 67 There was a 15% reduction in albuminuria without any significant changes in serum creatinine, potassium, blood urea nitrogen, and eGFR. 67 These findings provide evidence for the safety of sacubitril/valsartan in patients with hypertension and CKD.
The UK HARP-III (Randomized Multicenter Pilot Study of Sacubitril/Valsartan versus Irbesartan in Patients with Chronic Kidney Disease: United Kingdom Heart and Renal Protection) study compared LCZ696 with irbesartan (an ARB) in 414 patients with proteinuric CKD (eGFR 20–60 ml/min/1.73 m2) to assess the short-term safety and efficacy of LCZ696 in this population with respect to changes in eGFR. 68 At 1-year follow up, measured eGFR was similar between the treatment groups. 69 Sacubitril/valsartan-treated patients had a reduced BP of 5/2 mmHg and a nonsignificant reduction in albuminuria. 69 Rates of adverse events were similar between groups. 69 These data strengthen the evidence for the safety of sacubitril/valsartan in patients with CKD although the clinical implications of these findings have to be evaluated.
Investigations of sacubitril/valsartan in other CV diseases
Pulmonary hypertension
The PARENT (Pulmonary Artery Pressure Reduction with Entresto) trial is an ongoing study that aims to study the effects on pulmonary artery pressure reduction in patients with congestive HF with an implanted hemodynamic monitor (CardioMEMSTM HF System) randomized to receive sacubitril/valsartan versus ACEI/ARB. 70 Data from this study may provide important mechanistic insights into the incremental acute and long-term hemodynamic effects of composite ARNIs over enalapril in HF patients. 70
Mitral regurgitation
The PRIME (Pharmacological Reduction of Functional Ischemic Mitral Regurgitation) trial is a randomized trial to test the efficacy of sacubitril/valsartan versus valsartan alone in reducing functional ischemic mitral regurgitation in patients with HF and LVEF between 25% and 50% at 12 months of follow up. 71 To date, no medical therapy has been proven to improve functional mitral regurgitation and the investigators hope that the neurohormonal effects of sacubitril/valsartan will open new avenues in the treatment of this difficult subset of HF. 71
Endothelial function
The PARADOR (Comparing ARNI With ACE Inhibitor on Endothelial Function) trial is a planned multisite, randomized, double-blind trial designed to compare the effects of sacubitril/valsartan with enalapril on endothelial function in patients with HFrEF. 72 The favorable neurohormonal effects of sacubitril/valsartan are hypothesized to improve endothelial function assessed by an increase in flow mediated vasodilation measured by brachial artery reactivity test. 72
Peripheral arterial disease
Peripheral arterial disease due to blockages in the aorto-iliac vessels is due to atherosclerotic plaque formation which was traditionally treated by aggressive risk factor modification and mechanical revascularization when critical. 73 At a cellular level, mitochondrial and microvascular dysfunction are thought to play a role in the development of peripheral arterial disease. 73 NPs are known to increase mitochondrial and microvascular density and in turn should improve oxygen consumption and perfusion to skeletal muscles. 73 There has been recent interest in using NEPIs to improve limb ischemia. Sacubitril/valsartan is currently being studied in a randomized placebo-controlled trial to evaluate increase in treadmill walk time to pain onset as the primary outcome and novel markers of mitochondrial and microvascular function as secondary outcomes. 73
Limitations
As discussed above, clinical trial experience with ARNIs has shown ARNI use offers a significant benefit when compared with ACEI or ARB alone in patients with HFrEF and several studies are evaluating the use of this drug class in other CV disease conditions. As with the pros, the limitations associated with ARNI use also deserve acknowledgement.
The primary reason that led to ACEI-NEPI combination being decommissioned was the increase in incidence of angioedema. While ARNIs, due to the ARB component, are not associated with an increased risk of angioedema to the same extent as an ACEI-NEPI combination, these agents still are associated with an increased risk of angioedema compared with ACE inhibitors alone. 5 ARNIs are also associated with more symptomatic hypotension compared with ACEIs or ARBs alone. 5 Symptomatic hypotension was the most common adverse event reported with sacubitril/valsartan in the PARADIGM-HF and PARAMOUNT trials with a frequency of 18% and 19%, respectively.5,27 The risk of other adverse effects of ACEI or ARB use such as hyperkalemia, cough, and worsening renal function persist with ARNI but have been shown to be lower than ACEI use alone. 5 The risk of hyperkalemia with ARNI use increases with the concurrent use of potassium sparing diuretics.
The urine albumin to creatinine ratio (UACR) is used as a marker of renal disease progression. Using the PARADIGM-HF data, Damman and colleagues compared the effect of sacubitril/valsartan and enalapril on renal disease progression using indicators such as eGFR and UACR. 74 The study reported that sacubitril/valsartan had a lower reduction in eGFR compared with enalapril. There was a significant increase in UACR in the sacubitril/valsartan group while UACR in the enalapril group did not change significantly (p-value between groups = 0.016). 74 The increase in UACR with sacubitril/valsartan is postulated to be due to an increase in glomerular permeability, hydraulic conductivity and change in renal arteriolar tone. This increase in UACR is not associated with significant progression of renal disease leading to worse renal outcomes. 74
As with other ACEIs and ARBs, ARNIs also inhibit RAAS and have potential teratogenicity, precluding the use of this class of medications in pregnancy. Switching from a generic ACEI to an ARNI could potentially result in an eight-fold increase in the medication cost and has been a barrier to the widespread adoption of ARNI in the groups that have been shown to derive a benefit. 75
Current guidelines and place in therapy
The strongest evidence for the use of sacubitril/valsartan in CV disease comes from the PARADIGM-HF trial in which patients treated with this ARNI had substantially improved CV outcomes compared with the current standard of care. The United States Food and Drug Administration (US FDA) reviewed LCZ696 under its priority review program with a fast-track designation and approved this drug for the treatment of all NYHA functional class II–IV HFrEF patients in July 2015. 53 The European Medical Agency approved the use of sacubitril/valsartan for the treatment of adult patients with symptomatic chronic HFrEF. 53
In the 2016 focused update on HF guidelines, the American College of Cardiology, the American Heart Association, and the Heart Failure Society of America gave a class I recommendation to sacubitril/valsartan for the treatment of HFrEF patients. 76 The guidelines recommended replacing an ACEI or ARB with an ARNI in patients with chronic symptomatic HFrEF, NYHA class II or III, currently tolerating an ACEI or ARB, to further reduce morbidity. 76 The guideline also recommended against concomitant use of ARNI with ACEI or within 36 hours of the last ACEI dose to prevent possible angioedema (class III recommendation). 76
The Canadian Cardiovascular Society was the first to incorporate the use of sacubitril/valsartan in HF patients. In their 2017 update on Heart Failure Management Guidelines, the Canadian guidelines recommend the use of LCZ696 in place of an ACEI or an ARB in patients with HFrEF, who remain symptomatic despite treatment with appropriate doses of guideline-directed medical therapy, to reduce CV death, HF hospitalizations, and symptoms (strong recommendation; high-quality evidence). 77 A currently ongoing prospective open label trial (PARTHENON) will evaluate the safety and efficacy of sacubitril/valsartan in reducing the rate of all-cause hospitalization or all-cause mortality in relation to NT-proBNP or BNP levels (Table 2). 38
The 2016 European Society of Cardiology HF guidelines recommend the use of sacubitril/valsartan as an ACEI replacement to further reduce the risk of death and HF hospitalization in ambulatory patients with HFrEF (LVEF < 35%) who remain symptomatic despite optimal treatment with ACEI, a beta-blocker, and an MRA (class IB recommendation). 78
Conclusion
Sacubitril/valsartan represents a major therapeutic advance in the avenue of CV disease, particularly HF. While the major focus of research for the use of ARNI in CV disease will be in the realm of HF, sacubitril/valsartan has shown tremendous promise in the treatment of important CV risk factors like hypertension. Investigative research to identify mechanistic insights into the actions of sacubitril/valsartan continue to provide positive data on the CV actions of this ARNI on cardiac remodeling, vascular function, and endothelial dysfunction. Numerous currently undergoing clinical trials will study if the substantial clinical benefit demonstrated by this combination ARNI in HFrEF patients will extend across various other forms of CV disease. The expansion of therapeutic indications of sacubitril/valsartan and development of more novel ARNIs to target different subsets of CV disease remain promising questions at this time.