
Abstract
Background:
Rapid interpretation of electrocardiography (ECGs) is essential for reducing patient mortality and morbidity associated with heart conditions. Despite its significance, many healthcare providers struggle to achieve proficiency in ECG interpretation.
Objective:
This study assessed nurses’ knowledge, practices, and associated factors regarding ECG interpretation in the emergency and intensive care units of selected public hospitals in Addis Ababa, Ethiopia.
Methods:
A cross-sectional study was conducted to evaluate nurses’ knowledge, practices, and factors related to ECG interpretation in selected public hospitals of emergency and intensive care units in Addis Ababa, Ethiopia. Data were collected using structured, self-administered questionnaires and analyzed using SPSS version 26. Binary logistic regression models were employed to identify associations between the dependent and independent variables.
Results:
Among 255 of the study participants, only 60 (23.5%) and 69 (27.1%) of them demonstrated good knowledge and practice in ECG strip interpretation, respectively. The most frequently recognized ECG strip was asystole. Factors associated with good knowledge and practice encompassed holding a master’s degree, receiving ECG training, and working in intensive care units.
Conclusion:
This study identified the lack of knowledge and practice among nurses in ECG interpretation. The findings highlight the need for training programs and experience-sharing initiatives to enhance nurses’ proficiency in ECG interpretation which might ultimately improve patient outcomes.
Introduction
Electrocardiography (ECG) is an essential, noninvasive modern tool to assess the electrical activities of the heart. 1 It has a high capacity to detect any abnormalities in people with cardiovascular diseases.2,3 Cardiovascular diseases have increased worldwide, causing morbidity in half a billion people, and their mortality reached 20.5 million people. 4 Early ECG and its interpretation enhance patient survival. 5
Health professionals who work in emergency departments and intensive care units (ICUs), particularly nurses who are the first responders for patients, must be proficient in skills such as ECG interpretation. 6 The increasing shortage of physicians has shifted the responsibility of ECG interpretation to nurses, making their proficiency essential.1,6,7 Competency in ECG interpretation requires understanding of the features and concepts of ECG strips, as well as critical thinking skills. 8 Despite its importance, many healthcare providers struggle with ECG interpretation. 9 Poor knowledge and practice in ECG interpretation is a global issue that affects both low- and high-income countries. For instance, a study in China found that 70.9% of ICU nurses had low knowledge regarding ECG, which is consistent with findings from a study in Saudi Arabia.1,10,11 Similarly, studies conducted in Egypt and Addis Ababa indicated that 80% and 90.9% of the nurses studied had unsatisfactory levels of knowledge, respectively. 11 This lack of understanding among nurses can lead to inadequate management of potentially life-threatening cardiac arrhythmias. 6
A nurse who lacks proficiency in ECG interpretation can have significant consequences for patient care, including delays in diagnosis and treatment, medication errors, poor patient outcomes, and complications. In addition, it raises legal and ethical concerns while compromising patient safety, quality of care, and overall healthcare costs.3,12 Bridging these gaps requires a comprehensive approach that includes specialized training, clinical experience, certification, ongoing education, simulation and skill laboratories, and collaboration among various healthcare disciplines. 13 However, there is a lack of data regarding the knowledge and practice of nurses in ECG interpretation, specifically in Ethiopia. This study aimed to assess nurses’ knowledge, practices, and associated factors related to electrocardiogram (ECG) interpretation in the emergency and ICUs of selected public hospitals in Addis Ababa, Ethiopia.
The insights gained from this study in Addis Ababa could serve as a model for other regions facing similar healthcare challenges related to the lack of knowledge and practice among nurses on ECG interpretation. Sharing best practices through publications or conferences could help disseminate knowledge about ECG interpretation. 1 Collaborating with international health organizations could facilitate research opportunities that further explore the effectiveness of this approach across diverse settings. 11 However, further research is necessary to address existing knowledge gaps and refine methodologies for effectively assessing its impact. The outcomes could enhance ECG interpretation knowledge and practice among healthcare professionals, particularly nurses, ultimately improving patient care in emergency rooms and ICUs. By focusing on policy implications and operational practices tailored to local contexts such as Addis Ababa, healthcare systems can better prepare for future challenges while improving patient outcomes. Many studies focus on specific contexts or populations, making it challenging to generalize findings across different healthcare settings. There is a need for more comprehensive studies that explore various factors influencing the knowledge and practice gap among nurses in ICUs and emergency rooms on ECG interpretation.
Method
Study design, area, and period
An institution-based cross-sectional study was conducted in five randomly selected public hospitals in Addis Ababa, Ethiopia, from March to April 2024. These hospitals include Tikur Anbessa Specialized Hospital, St. Peter Specialized Hospital, AaBet Referral Hospital, Menelik Referral Hospital, and Zewditu Memorial Hospital, focusing on the emergency and ICUs.
Inclusion criteria: All nurses with at least 6 months of work experience during the data collection period in the randomly selected public hospitals were included in the study.
Exclusion criteria: All nurses who were unavailable during the study period due to maternity leave, annual leave, or sick leave were excluded.
Sample size determination: The sample size was calculated using a single population proportion formula. n, where n the is required sample size, Zα/2 is the critical value of the standard normal distribution at the desired confidence level (95% confidence, Zα/2 = 1.96), d is the margin of error (precision of the estimate), and P is the estimated population proportion (set at 0.5 due to the lack of prior studies in both emergency and ICU in Ethiopia, which gives the maximum sample). The study population was less than 10,000; therefore, a sample size correction formula was applied, nadj = . After adding a 10% non-response rate, the total final sample size was 277.
Sampling method and procedure
This study employed a stratified random sampling method to enhance the representativeness and generalizability of the findings. First, five public hospitals in Addis Ababa with ICU and emergency department setups were selected using the lottery method of simple random sampling from a pool of 12 eligible public hospitals. The sample size was proportionally allocated to each hospital and department based on their nurse population size to ensure balanced representation. Within each hospital stratum, simple random sampling was used to select individual nurses until the required sample size was achieved. The use of stratification and random selection reduces selection bias and enhances the likelihood that the sample reflects the broader nursing population within similar hospital contexts.
While the sample focuses on public hospitals, the diversity across multiple hospitals and departments allows cautious generalization of findings to nurses working in comparable clinical settings in other public hospitals. However, generalizability to nurses in private hospitals or non-hospital care settings may be limited due to possible differences in organizational structures, resources, and patient populations. Future research could extend sampling to include private and non-hospital nursing staff to further validate applicability across broader nurse populations.
Data collection tool
A structured, self-administered questionnaire was used for data collection. The questionnaire was adapted from various sources1,9,10,13,14 and ECG interpretation guidelines, 15 and it was modified to fit the participants’ characteristics. Therefore, it was validated by two experts, one from the English, and the other from the course expert. The reliability of the tool was determined from the pretest results, yielding Cronbach’s alpha of 0.825. The questionnaire comprised three sections: The first section focused on the demographic characteristics of the nurses and included 12 questions. The second section consisted of 12 true or false questions assessing the nurses’ knowledge of ECG interpretation. The third section evaluated nurses’ practices in ECG interpretation and management for selected ECG strips, containing 20 multiple-choice questions. This section included 10 12-lead II ECG strips for interpretation.
Operational definition
The scoring system used to categorize knowledge and practice levels was based on a cutoff point of 65%. Nurses who scored more than 65% on knowledge-related questions were classified as having good knowledge, whereas those who scored more than 65% on electrocardiographic interpretation and/or management questions were classified as having good practice. 11 This cutoff was selected in line with previous studies assessing healthcare professionals’ knowledge and practice levels, where a threshold was around 60–70. 11
Data quality control and management
Two data collectors with a background in research education received training. During the data collection process, the principal investigator checked the data at each point to ensure completeness and identify any missing information. A pretest of the self-administered questionnaire was conducted on 5% of the final sample size at Yekatit 12 Hospital.
Statistical analysis
After verifying completeness, the data were coded and entered into Epi Data version 4.6, then exported to Statistical Product and Social Service (SPSS) version 27 for analysis. Outliers and multicollinearity were checked using standard residuals and the variance inflation factor, respectively, and all variables were a factor over 10. Goodness of fitness was checked using Hosmer–Lemshow test, and all variables showed p value >0.05, indicating fit to logistic regression. Binary logistic regression was used to identify associations between the dependent and independent variables; those with a p value under 0.25 candidates for multivariable analysis. Variables significant at a p value less than 0.05 and with an adjusted odds ratio within the 95% confidence interval were considered factors associated with the knowledge and practice of nurses on ECG interpretation. Results were presented using figures, tables, graphs, and narration.
Results
Socio-demographic characteristics
Of the 277 individuals invited to participate, 255 agreed, resulting in a response rate of 92%. The mean age of the study participants was 30.02 ± 4.7 years, with the majority being male (n = 157, 61.6%). Most participants worked in the emergency department (n = 135, 52.9%), and the majority were college or university graduates holding a bachelor’s degree (n = 188, 73.7%; Table 1).
Socio-demographic characteristics of nurses working in emergency rooms and ICUs of public hospitals in Addis Ababa, Ethiopia, 2024 (n = 255).

ACLS, advanced cardiac life support; BLS, basic life support; BSc, Bachelor of Science; ECCN, Emergency and Critical Care Nurse; ECG, electrocardiogram; ED, Emergency department; ICU, intensive care unit; MSc, Master of Science.
Description of knowledge of ECG interpretation
Good ECG knowledge was defined by a test score above the 65th percentile. Among the 255 participants, only 60 (approximately 23.5%, with a 95% confidence interval of 19.0–29.0) achieved a score that placed them in this upper quartile. Most nurses correctly answered that the “QRS complex represents right and left ventricular depolarization” (n = 207, 81.2%). However, only 125 participants (49%) could appropriately recognize the order of ECG waves and intervals (Table 2).
Description of the knowledge of ECG interpretation of participants working in public hospitals in Addis Ababa, Ethiopia (n = 255).
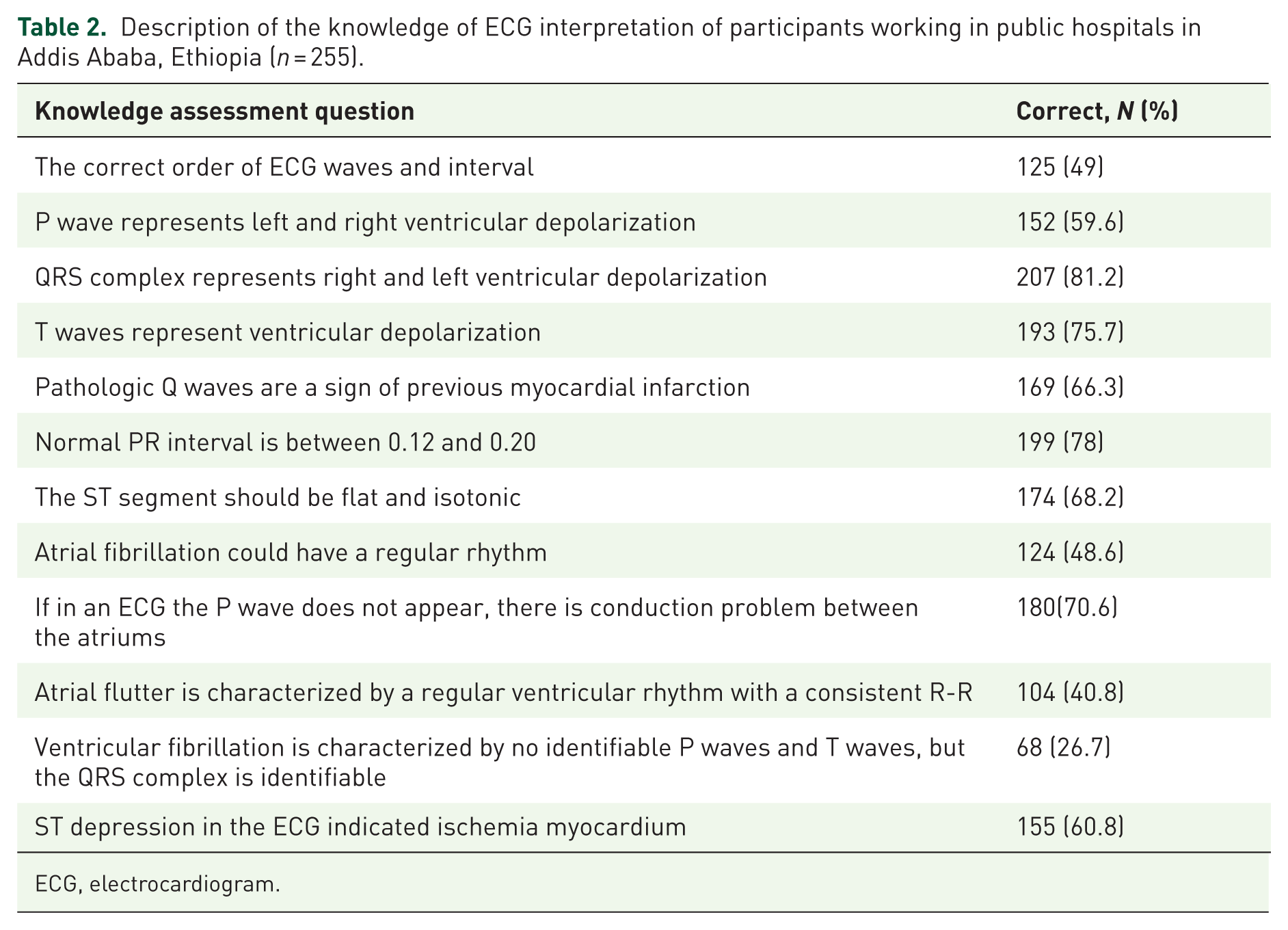
ECG, electrocardiogram.
Description of practice in ECG interpretation
Good ECG practice was defined by a test score above the 65th percentile. Among the 255 participants, only 69 (approximately 27.1%, with a 95% confidence interval of 21.7%–33.0%) achieved a score that placed them in this upper quartile. The practice-related question results indicated that the most frequently known items were interpretation and recognition of sinus bradycardia, 194 (76.1%); asystole, 195 (76.5%); and myocardial infarction (MI), 146 (57.3%). Poor recognition of atrial flutter (33.3%) and supraventricular tachycardia (SVT) (38%) likely reflects both gaps in detailed knowledge and limited clinical exposure. These complex rhythms require specific training and experience to identify accurately. In Ethiopia, ECG interpretation is neither incorporated into the nursing curriculum nor provided as in-service training, contributing to the poor recognition rates. This combination of insufficient formal education and limited hands-on exposure hinders nurses’ ability to confidently identify these arrhythmias. Moreover, more than half of the participants were correctly able to identify the correct management of asystole 165 (64.7%) and MI 152 (59.6%; Table 3).
Description of practice in ECG interpretation of participants working at the public hospital of Addis Ababa, Ethiopia (n = 255).
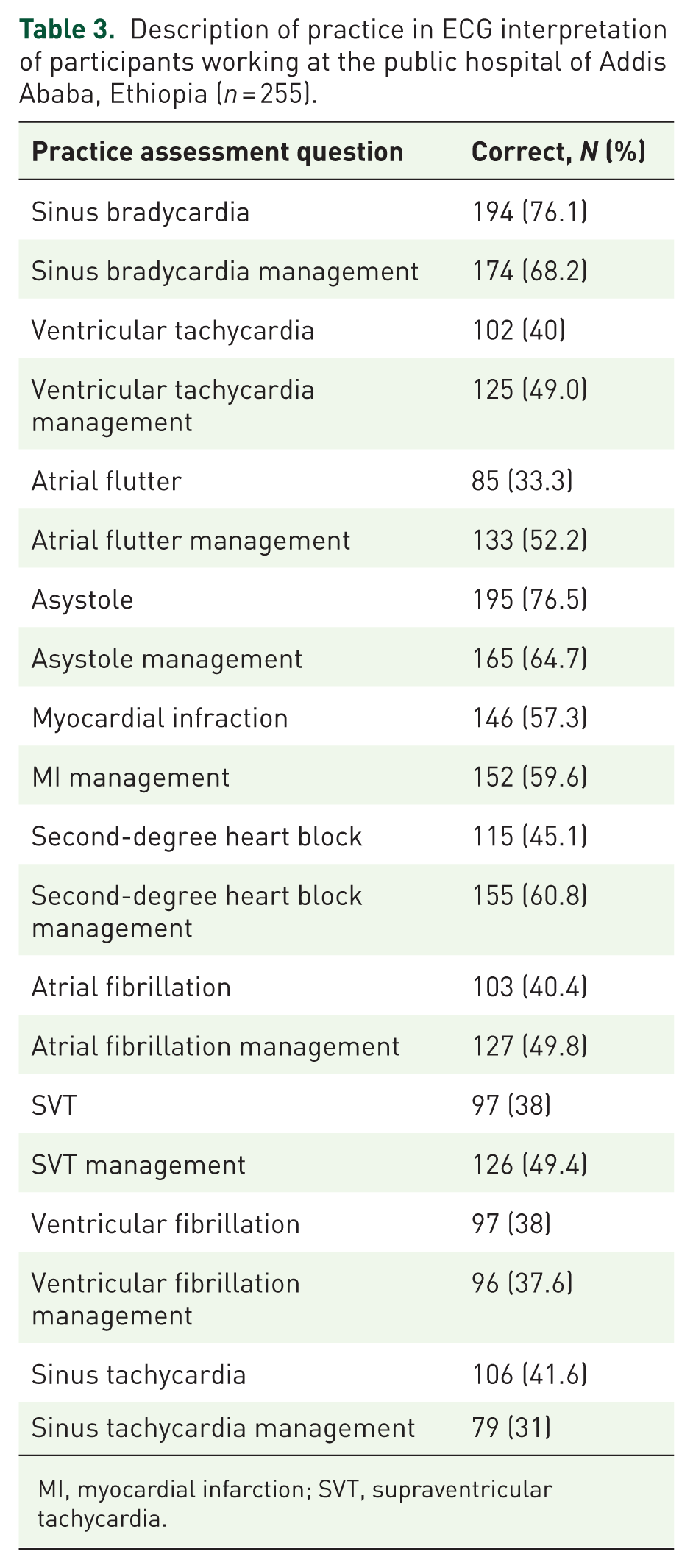
MI, myocardial infarction; SVT, supraventricular tachycardia.
Factors associated with knowledge and practice of ECG interpretation for nurses
The logistic regression model with multivariable analysis revealed that the level of education, workplace, and ECG training were significantly associated with the knowledge and practice of nurses in ECG interpretation. Nurses working in ICUs demonstrated three times more knowledge (adjusted odds ratio (AOR) = 2.79; 95% CI: 1.27–6.16) and practice (AOR = 2.72; 95% CI: 1.26–5.88) in ECG interpretation compared to their counterparts in other departments. In addition, nurses with a master’s degree were six times more likely to possess good knowledge (AOR = 6.74; 95% CI: 2.7–8.45) and five times more likely to practice effectively (AOR = 5.64; 95% CI: 3.41–12.47) than those with a bachelor’s degree. Furthermore, nurses who received ECG training had two times more knowledge (AOR = 2.89; 95% CI: 1.11–7.47) and four times more practice (AOR = 4.31; 95% CI: 1.7–10.94) than those who did not receive any training (Table 4).
Factors associated with knowledge and practice of ECG interpretation for nurses working in emergency rooms and intensive care units of public hospitals in Addis Ababa, Ethiopia.

Significant at p < 0.05.
AOR, adjusted odds ratio; CI, circumference interval; ECG, electrocardiogram; ICU, intensive care unit; MSc, Master of Science.
Discussion
This study assessed nurses’ knowledge and practice on ECG interpretation, showed that only 23.5% demonstrated adequate knowledge and 27.1% demonstrated explicit good practice. While some ECG components, such as identifying the QRS complex and recognizing MI, were correctly interpreted by most of the participants. Other critical arrhythmia, such as ventricular tachycardia and atrial flutter, showed remarkably lower accuracy. Educational level, clinical area, and prior ECG training emerged as significant factors influencing nurses’ knowledge and practice in ECG interpretation. This highlights the need for ongoing educational support and training programs to enhance nurses’ competence in ECG interpretation.
Our findings align with those of many international studies, reporting suboptimal ECG knowledge among nurses. For instance, a study in China found that 70.9% of ICU nurses had low ECG knowledge, 12 while similar findings were reported in Saudi Arabia 10 and Egypt, 2 where 61% of nurses could not accurately interpret the ECG 12-lead rhythm. Similarly, Indonesian nurses struggled with the ECG interpretation, with 70.9% showing inadequate skill. 16 A prior study in Addis Ababa showed that 90.9% of nurses had inadequate ECG competence. 11 The slight variation in this figure might be explained by the difference in the study population; for instance, ICU nurses in our study demonstrated adequate knowledge levels than nurses working in the emergency room, likely due to ICU nurses having more frequent exposure to cardiac cases, thus might contribute to nurses having better knowledge and skill on ECG interpretation. 1
By contrast, a Spanish study reported that 93% of emergency nurses correctly interpreted ECGs. 17 This stark difference might be attributed to variations in healthcare infrastructure, nurses’ training curricula, and continuing education availability. In addition, many nurses in our study had received cardiac-related training 2–5 years prior, suggesting that knowledge decay over time without refresher courses could contribute to lower ECG competence levels.5,6 This highlights the critical importance of regular, updated ECG training to maintain proficiency. 9
More than half of the study participants (50%) were unfamiliar with the correct order of the ECG wave and intervals; this finding contrasts with a Pakistan study, where over 50% answered correctly. 14 Similarly, 51.4% of participants incorrectly believed that atrial fibrillation could have a regular rhythm, whereas 61.5% of Turkish nurses answered this correctly. 1 However, questions related to fundamental ECG components such as the P wave representing atrial depolarization (59.9%), the QRS complex representing ventricular depolarization (81.2%), and ST depression indicating myocardial ischemia (60.8%) were answered correctly by most of the nurses, mirroring results from Turkey and China.1,12
Regarding ECG practice, the most commonly recognized arrhythmias were asystole (76.5%), sinus bradycardia (76.1%), and myocardial infarction (MI; 57.3%). These rates are somewhat lower than those reported in Turkey, where asystole recognition reached 94.1%, 1 and Pakistan, where 61.7% correctly identified acute MI. 14 Conversely, ventricular tachycardia and atrial flutter were poorly identified, with correct response rates of 40% and 33.3%, respectively. This contrasts sharply with Turkish nurses, who recognized ventricular tachycardia and atrial flutter at rates above 80%. 1 Such discrepancies may reflect differences in training emphasis, clinical exposure, or availability of ECG interpretation resources.1,14 In Ethiopia, a significant proportion of nurses have limited ECG-related training and poor practice in ECG interpretation, which likely contributes to these lower recognition rates.
A significant difference in ECG knowledge was observed based on the nurses’ work area. ICU nurses demonstrated superior knowledge compared to nurses working in the emergency department, probably due to frequent exposure of ICU nurses to ECG. This increased exposure to cardiac patients and ECG interpretation likely enhances ICU nurses’ skills in ECG. Remarkably, a Pakistani study found the opposite trend, with coronary care and emergency nurses scoring higher than ICU nurses, 14 suggesting that institutional roles and patient distribution critically influence ECG competency. 14
Educational level, such as nurses’ masters’ degree level, also played a role; nurses with a master’s degree performed better than those with bachelor’s or diploma qualifications. This aligns with findings from Malaysia and Saudi Arabia, where higher academic attainment correlated with improved ECG knowledge and practice. 17 These results reinforce the value of advanced education and specialized training in developing clinical competencies.
Our study demonstrated a significant association between prior cardiac-related training and both knowledge (p = 0.006) and practice (p = 0.014) of ECG interpretation. This is consistent with studies from Spain, 17 Turkey, 1 and Malaysia,25 which showed that recent and ongoing training substantially improves nurses’ ECG interpretation skills. However, the effectiveness of training depends on its frequency and recency; outdated training may not sufficiently equip nurses to interpret complex arrhythmias accurately.
The overall low levels of ECG knowledge and practice among nurses in this study highlight a critical gap in emergency and intensive care settings that could impact patient outcomes. Given the demonstrated benefits of training and education, healthcare institutions should prioritize regular, updated ECG interpretation training tailored to nurses’ clinical roles. In addition, integrating ECG competency assessments into professional development and certification processes may help maintain high standards. The differences observed across countries emphasize the influence of healthcare infrastructure, nurse education systems, and resource availability. Future research should explore these contextual factors in greater depth to design targeted interventions that address local challenges. This study briefly highlights potential curriculum gaps in nursing education that may contribute to the poor recognition of certain cardiac rhythms, such as atrial flutter and SVT. This addition underscores the need for strengthened ECG interpretation training within nursing curricula.
Limitation
The study is limited by its cross-sectional design, which restricts the ability to establish cause-and-effect relationships. In addition, private hospitals were excluded due to budget constraints, limiting the generalizability of findings to public hospital settings only, where patient flow, resource availability, and management systems may differ from public hospitals in Addis Ababa. The use of self-reported questionnaires may also introduce response bias, as participants might overestimate or underestimate their knowledge and practices, potentially affecting the accuracy of the results. These factors should be considered when interpreting the findings and applying them to broader nurse populations.
Conclusion
The results showed a lack of knowledge and practice among nurses in Ethiopia, especially in the study setting of Addis Ababa. The precision of responses to specific ECG interpretation questions varied; some questions received high response rates, while most demonstrated lower accuracy. This finding underlined the importance of providing ongoing learning opportunities and experience-sharing programs for nurses. Factors such as educational level, practice area, and previous training significantly affect knowledge and practice on ECG interpretation. Therefore, it is crucial to implement educational programs and continuous training to support nurses in staying updated with the latest advancements in ECG technology.
Implications of the study
This study identified areas where nursing professionals may require supplementary provision. Moreover, it serves as a foundation for initiating training programs, new clinical guidelines, and protocols that emphasize the importance of accurately interpreting ECGs. Moreover, these findings are valuable for policymakers and hospital administrators as they seek to address gaps in staff knowledge, allocate resources effectively, and enhance the quality of care within emergency departments and ICUs.
Footnotes
Acknowledgements
The authors are grateful to the data collectors, the Addis Ababa University College of Health Sciences Department of Emergency and Critical Care, the health professionals in the pediatric emergency unit, and all study participants for their contributions to the study’s success.