
Abstract
Background:
The use of ultrasound-based methods for imaging of subclinical atherosclerosis, including measurement of carotid plaque burden (cPB), is a promising direction for further improvement of major adverse cardiac and cerebrovascular events (MACCE) prediction.
Objectives:
The aim of the study was to research the prognostic values’ significance of cPB indicators with regard to the short-term progression of polyvascular subclinical atherosclerosis and the long-term onset of MACCE.
Design:
Single-center prospective cohort study.
Methods:
The study included patients 40–64 years of age. All patients underwent duplex scanning (DS) of the carotid and lower limb arteries. The following cPB indicators were determined: carotid plaque score (cPS), maximum carotid plaque thickness (cPTmax), and carotid total plaque area (cTPA). The combined endpoint included the following components: cardiovascular death; nonfatal myocardial infarction; nonfatal stroke or transient ischemic attack (TIA); revascularization of the coronary and/or peripheral arteries.
Results:
The study included 387 patients, among whom 142 (36.7%) patients underwent repeated DS after 12–24 months. The median follow-up time was 20.0 (13.0; 36.5) months. MACCE were recorded in 33 (8.52%) of patients. cTPA and cPTmax, but not cPS, were independently associated with the progression of subclinical polyvascular atherosclerosis over a period of 13.9 months of follow-up. cTPA, but not cPTmax and cPS, was independently associated with the development of MACCE over a period of 20.0 months of follow-up. Only a cTPA > 42.0 mm2 proved to be an independent predictor of both the progression of subclinical polyvascular atherosclerosis and MACCE.
Conclusion:
In patients from 40 to 64 years of age with various cardiovascular risks, among the indicators of the cPB, only an increase in cTPA > 42.0 mm2 was shown to be independently associated with an increase in the relative risk (RR) of progression of subclinical polyvascular atherosclerosis by 2.38 (1.08–5.25) times, as well as with the development of MACCE by 3.10 (1.54–6.26) times.
Introduction
Existing methods for the assessment of cardiovascular risks (CVR) have a number of serious limitations that have led to the search for clinical approaches that are based on the wider use of circulating biomarkers and non-invasive imaging.1,2 The use of ultrasound-based methods for imaging of subclinical atherosclerosis, including measurement of plaque burden, is a promising direction for further improvement of major adverse cardiac and cerebrovascular events (MACCE) prediction.3,4
It should be noted that the search for non-invasive markers associated with the risk of MACCE is one that is relevant both in the context of primary and secondary cardiovascular prevention.5,6 Despite the increasing role that coronary artery calcium testing plays in the CVR stratification and guidance of personalized allocation of statins and aspirin, ultrasound imaging of atherosclerosis, including that which provides carotid plaque burden (cPB) assessment, still possesses a high potential as a tool for improving the prediction of MACCE.7–9 Moreover, dynamic cPB measurements may have certain advantages in evaluating the effectiveness of lipid-lowering therapy. 10 The most commonly used indicators of cPB are the carotid total plaque area (cTPA), and carotid plaque thickness (maximum carotid plaque thickness (cPTmax), and total carotid plaque thickness (carotid plaque score, cPS).11,12 Although the American Society of Echocardiography (ASE) Recommendations for the Assessment of Carotid Arterial Plaque by Ultrasound for the Characterization of Atherosclerosis and Evaluation of Cardiovascular Risk only recommend the use of cPTmax in clinical practice, other indicators of cPB, such as cTPA, may have an equal or even greater predictive value.3,13,14 However, there is currently only limited data concerning direct comparisons of the prognostic significance of various cPB markers.
One of the main tasks in the search for predictors of the progression of subclinical atherosclerosis is to improve the identification of patients with a higher RR of MACCE, which may be underestimated with a one-time assessment of CVR. 15 In a series of clinical studies, it was shown that the short-term progression of subclinical atherosclerosis may be associated with an increase in the RR of MACE (non-fatal myocardial infarction, death, unplanned coronary revascularization) and MACCE in the long term.16,17 In the study by Gacoń et al., which included 466 symptomatic patients with symptomatic coronary artery disease (CAD) and peripheral arterial disease (PAD), carotid intima-media thickness (cIMT) progression over 21–41 months was independently associated with an increased RR of MACCE over 5 years of follow-up (RR 1.22; 95% CI: 1.03–1.44; p < 0.001). 18 The results of the small number of studies currently available indicate that the initial cPB can be both a predictor of the short-term progression of atherosclerosis and one, which would indicate the risk of MACCE in the long term as well. 19 The aim of the current study was to research the prognostic values’ significance of cPB indicators with regard to the short-term progression of polyvascular subclinical atherosclerosis and the onset of MACCE.
Methods
The current single-center prospective cohort study included men and women between the ages of 40 and 64. The study included outpatients referred by general practitioners to outpatient cardiovascular service by the institutional cardiovascular complications prevention program. All patients signed an informed consent agreement to participate in the study. The protocol covering the study was approved by the Ethics Committee (the minutes of the meeting of the Ethics Committee concerning Protocol No. 10 and dated 27 October 2018). The exclusion criteria for the study were the following clinical conditions: acute coronary syndrome; acute cerebrovascular events; symptomatic carotid artery disease (a history of stroke/transient ischemic attack (TIA), carotid revascularization); symptomatic lower limb peripheral artery disease (intermittent claudication, chronic limb-threatening ischemia, lower limb revascularization); severe liver dysfunction, and severe chronic kidney disease (decreased estimated glomerular filtration rate (eGFR) less than 30 mL/min/1.73 m2); malignant neoplasms; mental illnesses; alcohol and substance abuse.
All patients were assessed for baseline cardiovascular risk at inclusion in the study according to the algorithm as recommended by 2019 ESC/EAS guidelines for the management of dyslipidaemias. 20
Duplex scanning (DS) of the carotid and lower limb arteries (LLA)
All patients underwent DS of the carotid and LLA. The examination was carried out using B-mode, color mapping mode, pulse Doppler mode, power Doppler mode. The following vessels were examined from both sides in longitudinal and cross-section throughout: common carotid arteries (CCA) with bifurcation, internal carotid arteries, external carotid arteries, common femoral arteries, superficial femoral arteries, popliteal arteries, the tibioperoneal trunk, anterior tibial arteries and posterior tibial arteries.
Atherosclerotic plaque was considered a focal thickening of the intima-media complex ⩾1.5 mm or 0.5 mm more than the surrounding cIMT, or 50% more than the cIMT of adjacent CCA areas. 21 The percentage of stenosis was determined according to the ECST method (the European Carotid Surgery Trial).
The following cPB indicators were determined: cPS, cPTmax, and cTPA. cPS was determined by the method described earlier as the total thickness of all carotid plaques without taking into account their length. 22 The measurements of cPTmax were carried out in accordance with the ASE recommendations. 3 The cTPA measurements were also carried in accordance with the previously described method.22,23 Examples of the measuring indicators of the burden of carotid atherosclerosis are shown in Figure 1.

Example of cPB indicators measurement: (a) native image of carotid plaque in carotid bifurcation; (b) measurement of plaque area; (c) measurement of cPTmax.
The study was carried out with a linear transducer at a frequency of 10 MHz on a digital ultrasonic multifunctional diagnostic scanner ‘Canon Aplio 400’ (Tokyo, Japan). All studies were performed by one trained operator.
Laboratory examination
The following biochemical laboratory blood parameters were obtained after fasting for at least 8 h: total cholesterol (TC), low-density lipoprotein cholesterol (LDL-cholesterol), high-density lipoprotein cholesterol (HDL-cholesterol), triglycerides (TG), glycated hemoglobin, glucose (venous blood), high-sensitivity C-reactive protein (hsCRP), and creatinine (with subsequent calculation of eGFR using the CKD-EPI equation).
Assessment of the progression of subclinical polyvascular atherosclerosis and collection of data on the onset of MACCE
The progression of subclinical polyvascular atherosclerosis was assessed in a subgroup of patients who underwent a repeated DS of the carotid and LLA after 12–24 months. For cTPA and cPS, intraobserver reproducibility was assessed (all measurements were taken by a single operator). For this purpose, measurements were taken in 20 patients at 24–48 h intervals, followed by a calculation of the coefficient of intra-class correlation with 95% CI: cTPA – 0.993 (95% CI: 0.982–0.997), cPS – 0.998 (95% CI: 0.996–0.999). 24 In order to assess the progression of carotid atherosclerosis using the dynamics of the changes in cTPA and cPS and to minimize the influence of measurement error, the measurement error was calculated for these indicators. The measurement error (σ) was equal to three standard deviations of the difference between two measurements carried out at an interval of 24–48 h. The measurement error calculation of the cTPA and cPS were determined as 0.053 cm2 and 0.16 mm, respectively. An increase in cTPA and/or cPS > 2σ, that is, more than 0.106 cm2 and 0.32 mm, respectively, was considered as progression. 19 It is known that 1.96σ includes 95% of errors, which makes it possible to determine with a high degree of reliability the true increase in the cPB. 25 Thus, the criteria for the progression of subclinical polyvascular atherosclerosis were: (a) the appearance of a new plaque in at least one vascular bed (carotid or LLA); (b) an increase in the degree of stenosis in previously existing stenosis at ⩾10%; (c) an increase in the cTPA by more than 0.106 cm2 and/or an increase in the cPS by more than 0.32 mm. In order to classify a patient under the category of progressor, it was necessary to possess a ⩾1 criterion in two vascular beds.
The combined endpoint included the following components: cardiovascular death; nonfatal myocardial infarction; nonfatal stroke or TIA; revascularization of the coronary and/or peripheral arteries. Thus, the combined endpoint corresponded to MACCE plus revascularization. Data collection and the updating of data within the follow-up were carried out in different manners: through face-to-face dynamic patient visits and through data collection using medical information systems.
Statistical analysis
The statistical analysis of the data that was obtained was carried out using Microsoft Excel (Microsoft Corporation, Redmond, USA) and MedCalc software (version 20.216, MedCalc Software Ltd., Osten, Belgium). Qualitative variables were described using absolute and relative frequencies (percentages). Quantitative variables were described by a median (Me) with an indication of the interquartile range (lower quartile (LQ) and upper quartile (UQ)). In order to establish the cut-off values of the indicators which were studied, an ROC analysis was performed using a calculated level of sensitivity and specificity, as well as the calculation of the area under the characteristic curve (AUC) with a 95% confidence interval (CI). In order to identify the risk factors for MACCE and subclinical polyvascular atherosclerosis progression a step-by-step Cox regression analysis was performed. The dependent (predicted) variable was the time to the outcome, the independent variable was the studied factor. The critical significance level p for all statistical data analysis procedures used was assumed to be 0.05.
Results
The study included 387 patients, 193 male and 194 female; among the total, 142 (36.7%) patients underwent repeated duplex vascular scanning after 12–24 months (see Figure 2).
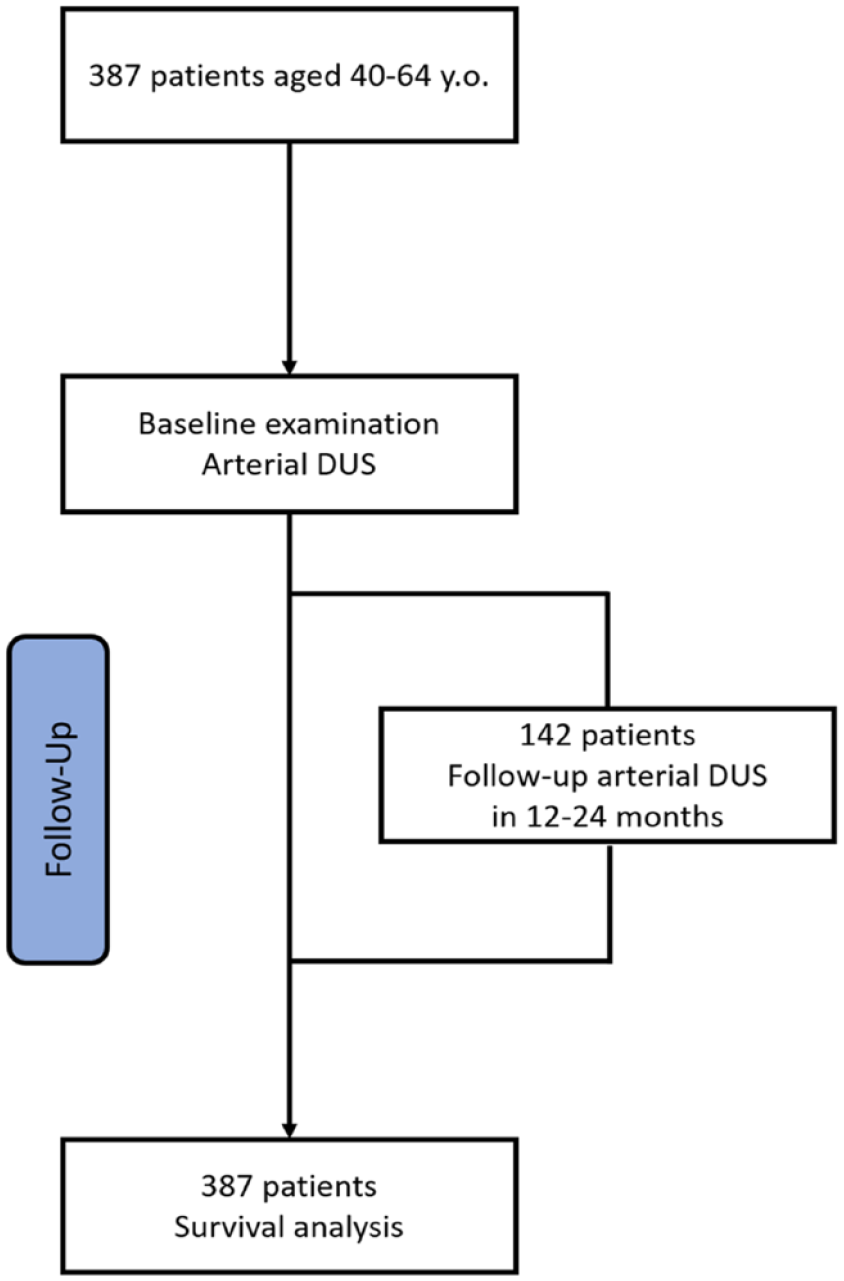
Study flowchart
Detailed clinical characteristics of patients and the results of the DS of the carotid LLA are presented in Table 1.
Clinical characteristics of patients and results of DS.

ACE, angiotensin-converting enzyme; ARBs, angiotensin II receptor blockers; BMI, body mass index; CA, carotid arteries; cPS, carotid plaque score; cPTmax, maximum carotid plaque thickness; cTPA, carotid total plaque area; CVR, cardiovascular risk; eGFR, estimated glomerular filtration rate; hsCRP, high-Sensitivity C-Reactive Protein; LLA, lower limb arteries.
Assessment of the short-term progression of subclinical polyvascular atherosclerosis
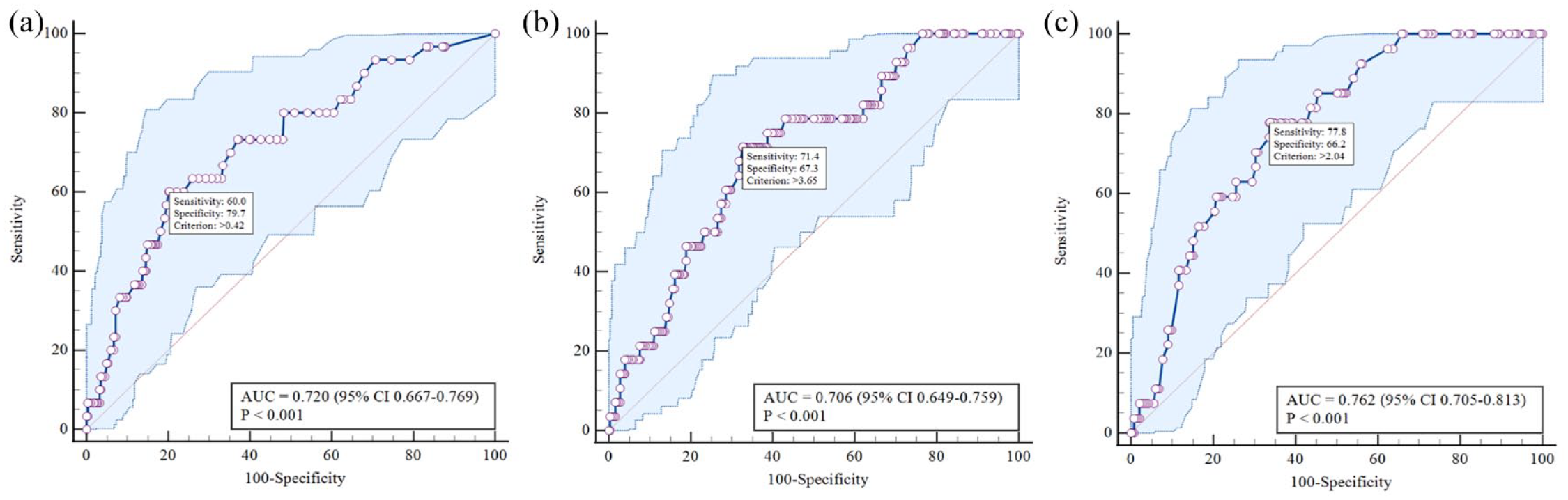
As mentioned earlier, repeated DS of the carotid and LLA was performed in 142 (36.7%) patients. The median time between the two studies was 13.9 (12.1; 22.7) months. The progression of subclinical carotid atherosclerosis was detected in 63 (44.3%) patients, LLA atherosclerosis – in 49 (34.5%) patients. The progression of subclinical atherosclerosis in both vascular beds was diagnosed in 31 (21.8%) patients. In order to determine the diagnostic values of cTPA, cPS and cPTmax in predicting the progression of subclinical polyvascular atherosclerosis, an ROC analysis was performed, the results of which are presented in Figure 3.

ROC-curves demonstrating the prognostic significance of cTPA (a), cPS (b), and cPTmax (c) in relation to the progression of subclinical polyvascular atherosclerosis.
The results showed that the diagnostic effectiveness of the cPB indicators according to the ROC analysis was comparable and the AUC did not differ significantly. Table 2 presents the results of the Cox regression analysis, demonstrating the relationship of the cPB indicators with the progression of subclinical polyvascular atherosclerosis.
Cox regression analysis results demonstrating relationships between cTPA, cPS and cPTmax, and progression of subclinical polyvascular atherosclerosis.
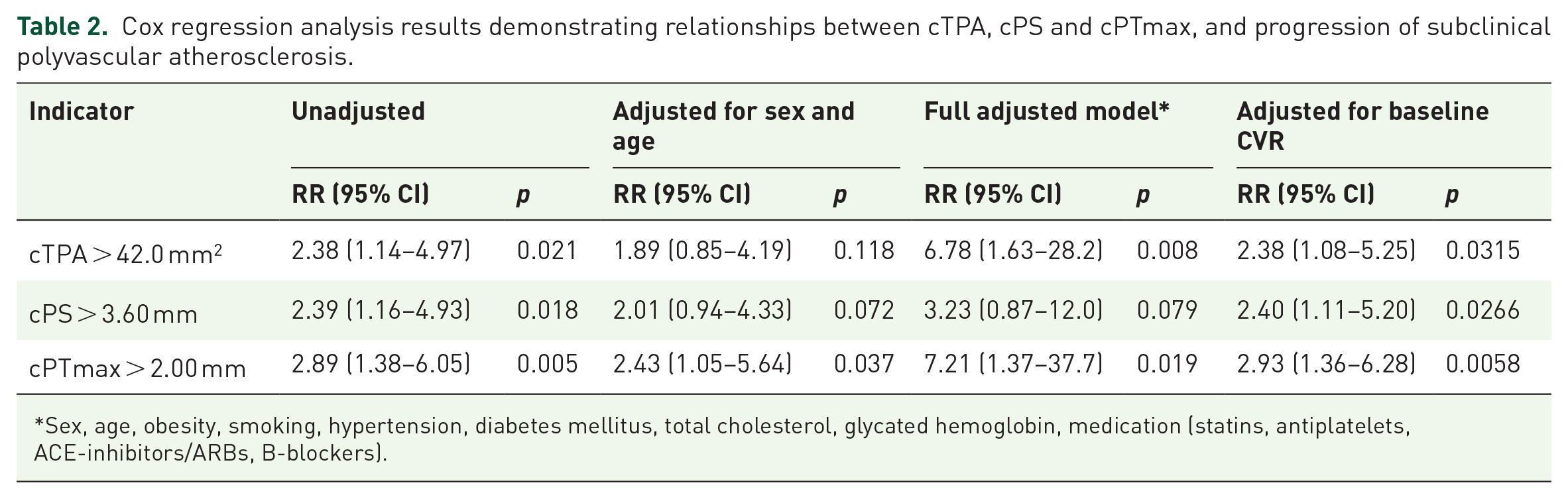
Sex, age, obesity, smoking, hypertension, diabetes mellitus, total cholesterol, glycated hemoglobin, medication (statins, antiplatelets, ACE-inhibitors/ARBs, B-blockers).
Assessment of the MACCE onset
The median follow-up time was 20.0 months (13.0; 36.5), which provided 895.4 patient-years of follow-up. MACCE were recorded in 33 (8.52%) of patients: 1 (0.26%) cardiovascular death; 8 (2.06%) – nonfatal myocardial infarction; 5 (1.29%) – nonfatal ischemic strokes or TIA; 12 (3.10%) – endovascular coronary revascularization; 5 (1.29%) – coronary artery bypass surgery; 1 (0.26%) – carotid endarterectomy; 1 (0.26%) – endovascular revascularization of the LLA.
In order to determine the cut-off values of cTPA, cPS and cPTmax in relation to the prediction of MACCE, an ROC analysis was performed, the results of which are presented in Figure 4.
ROC-curves demonstrating the prognostic significance of cTPA (a), cPS (b), and cPTmax (c) in relation to MACCE.
Table 3 presents the results of the Cox regression analysis, which demonstrates the relationship of the cTPA, cPS and cPTmax with the development of MACCE.
Cox regression analysis results demonstrating relationships between cTPA, cPS and cPTmax and MACCE.

Sex, age, obesity, smoking, hypertension, diabetes mellitus, total cholesterol, glycated hemoglobin, medication (statins, antiplatelets, ACE-inhibitors/ARBs, B-blockers).
Baseline cardiovascular risk assessment was performed according to the algorithm as recommended by 2019 ESC/EAS guidelines for the management of dyslipidemias.
Discussion
The assessment of the plaque burden in various vascular beds has proven to be a valuable source of additional prognostic data, regardless of other clinical and instrumental indicators. Thus, the burden of coronary atherosclerosis is a strong predictor of major adverse cardiovascular events (MACCE) and all-cause death regardless of the degree of coronary artery stenosis and myocardial ischemia according to the SPECT.26,27 The assessment of cPB also makes it possible to improve the cardiovascular events (fatal or non-fatal myocardial infarction, coronary revascularization, fatal or non-fatal stroke or TIA, or presence of a significant (⩾50%) stenosis assessed by invasive coronary angiography; new onset CAD or stoke) prediction in various patient populations.28,29 However, the search continues for the optimal indicators of the cPB for use at the current stage, as well as their validation on different patient populations.
The main results of the present study are the following: (a) cTPA and cPTmax, but not cPS, were independently associated with the progression of subclinical polyvascular atherosclerosis over a period of 13.9 months of follow-up; (b) cTPA, but not cPTmax and cPS, was independently associated with the development of MACCE over a period of 20.0 months of follow-up; (c) only a cTPA > 42.0 mm2 proved to be an independent predictor of both the progression of subclinical atherosclerosis and MACCE.
The independent prognostic value of cTPA in relation to cardiovascular events has been demonstrated in a number of clinical studies. It should be noted that the fairly wide range of optimal cut-off cTPA values obtained in these studies (from 18.7 mm2 to 119 mm2), can probably be partially explained by the varying characteristics contained in patient samples (age, initial CVR, the proportion of patients with established atherosclerotic cardiovascular disease (ASCVD) (including cerebrovascular diseases).22,28,30,31
A few studies have been conducted which directly compare the diagnostic and prognostic values of cPTmax and cTPA. In the work of Johri et al., which included 318 patients who underwent coronary angiography, the diagnostic efficacy of cPTmax, when used for the detection of coronary atherosclerosis, was higher than cTPA (AUC 0.752 versus 0.696 without specifying p for AUC difference). 32 In a study by Nicolaides et al. (the Cyprus Atherosclerosis Study), which included 985 patients without established ASCVDs, research was carried out on the prognostic significance of various indicators of the burden of carotid and femoral atherosclerosis in relation to the development of combined endpoint (fatal or nonfatal myocardial infarction, onset of angina, coronary artery revascularization, ischemic stroke, TIA, onset of claudication, or critical limb ischemia) over 13.2 ± 3.7 years of follow-up. 33 Among others, it was found that adding both the total carotid plaque thickness and cTPA to conventional risk factors led to a significant increase in the diagnostic effectiveness of the model (an increase in AUC to 0.751 and 0.742, respectively). 33 The Net Reclassification Improvement (NRI) values after addition to the standard model of total carotid plaque thickness was 9.5, which was significantly less than the NRI values produced by cTPA – 14.2 (p = 0.0017).
In the present study, the diagnostic values of cTPA, cPTmax, and cPS both in relation to the progression of subclinical polyvascular atherosclerosis and MACCE did not differ significantly (when evaluating p for AUC). However, according to the Cox regression analysis, after adjustment for potential confounders, an increase in cTPA was independently associated with the RR of progression of subclinical atherosclerosis and MACCE, while cPTmax was associated only with progression of subclinical atherosclerosis. It is possible that when assessing the cPB, it would be appropriate to measure both cPTmax and cTPA. 34 cTPA measurement is also likely to have an advantage over cPTmax in the dynamic evaluation of the effectiveness of therapy.31,33
A rapid progression of subclinical atherosclerosis may be associated with an increase in the RR of MACCE in both the short and long term. 35 The search for predictors of atherosclerosis progression and the identification of patients with rapid progression of subclinical atherosclerosis can improve and serve to personalize the management of this category of patients. 36 In our study, cTPA >42.0 mm2 was associated with both the progression of polyvascular atherosclerosis and the development of MACCE (mainly coronary, but also in the beds of the carotid arteries and arteries of the lower limb). It is thus likely that patients with cTPA > 42.0 mm2 can be considered as candidates for screening for asymptomatic polyvascular atherosclerosis, including for peripheral arterial diseases, as well as proactive testing for dynamic assessment of atherosclerosis. 37 Moreover, further study of the benefits of image-guided cardiovascular prevention and therapy is required.38,39
It should be noted that each of the indicators of cPB has strengths and limitations. 40 So, ASE only recommend the use of cPTmax in clinical practice as it allows a quantitative assessment of plaque burden, but its measurement demonstrates technical simplicity and minimal risk of error. 3 However, the cTPA measurement also shows almost perfect interobserver reliability (0.95; 95% CI: 0.83–0.99) and intraobserver reliability (0.96; 95% CI: 0.94–0.97). 41 Furthermore, the wider use of semi-automated or automated edge detection and image analysis software, in the future is expected to promote the use of more technically sophisticated and informative indicators. Another promising direction is the implementation of artificial intelligence technologies and machine learning approaches to measurement and analysis of 2D and 3D ultrasound images.42,43
According to the post hoc analysis of the sufficiency of the sample size, we found that the total sample size for a correct survival analysis should be at least 160 participants and according to the ROC analysis, at least 176 participants. The limitations of the study included: (a) the single-center character of the study; (b) a heterogeneous sample of asymptomatic patients with high/very high CVR and symptomatic patients with ASCVDs, which could have caused distortions in the assessment of the RR of ACE and (c) a limited number of patients who underwent repeated DS of peripheral arteries; (d) insufficient data on the treatment and frequency of achieving the goal LDL levels during the prospective phase of the study. This made it impossible to perform an analysis aimed at establishing the influence of this factor on the progression of atherosclerosis and cardiovascular outcomes.
Conclusion
In patients from 40 to 64 years of age with various CVR, among the indicators of the cPB, only an increase in cTPA > 42.0 mm2 was shown to be independently associated with an increase in the RR of progression of subclinical polyvascular atherosclerosis by 2.38 (1.08–5.25) times, as well as with the development of MACCE by 3.10 (1.54–6.26) times.