
Abstract
Objective
Statins are recommended as the first-line treatments for reducing the risk of major adverse cardiovascular events (MACE) in patients with acute coronary syndrome (ACS). The present study aimed to establish the baseline lipid levels associated with the greatest benefit from statin therapy in this population.
Methods
The study used a retrospective cohort methodology. In total, 636 patients with ACS were enrolled at Shaanxi Provincial People’s Hospital from 2011 to 2013. Participants were divided into four groups (group 1, hyperlipidemia with inconsistent statin use; group 2, no hyperlipidemia with inconsistent statin use; group 3, no hyperlipidemia with consistent statin use; and group 4, hyperlipidemia with consistent statin use).
Results
Patients in groups 3 (hazard ratio [HR] = 0.49, 95% confidence interval [CI] = 0.29–0.82) and 4 (HR = 0.21, 95% CI = 0.10–0.45) had lower risks of MACE than those in group 1. In subgroup analysis, patients in group 4 had a lower risk of MACE than those in group 3 (adjusted HR = 0.43, 95% CI = 0.21–0.89).
Conclusion
Sustained statin therapy is associated with a lower risk of adverse outcomes in patients with ACS, especially in those with higher baseline lipid levels.
Keywords
Introduction
Elevated lipid levels represent a leading cause of morbidity and mortality globally. In several studies, low-density lipoprotein cholesterol (LDL-C) and triglyceride (TG) levels were identified as independent risk factors for coronary heart disease.1–4 Lipid profile management is the main strategy for primary and secondary cardiovascular prevention.5,6 Statins are recommended as first-line treatments for hyperlipidemia, and they are extremely effective in reducing the risks of major adverse cardiac events (MACE).7–10 Among patients with acute coronary syndrome (ACS), accumulating evidence suggests that reducing LDL-C levels lowers the risks of death and cardiovascular events.11–14 However, the baseline lipid profile most likely to result in a benefit from statin therapy is less well established. Previous studies illustrated that higher baseline lipid levels amplify the short-term benefit of early intensive statin therapy in patients with ACS. Early atorvastatin therapy reduced the rates of 1-year major adverse cardiovascular and cerebrovascular events (MACCE) in patients with baseline LDL-C levels ≥100 mg/dL. 15 However, it is currently unknown whether superior risk reduction is achieved in long-term secondary prevention in patients with higher baseline lipid levels. Thus, the present study assessed the association between baseline lipid levels and MACE risk in patients with ACS who received sustained statin therapy.
Materials and methods
Study population
The study used a retrospective cohort methodology. In total, patients with ACS who visited Shaanxi Provincial People’s Hospital (Shaanxi, China) between January 2011 and December 2013 were eligible for enrollment. This study was approved by the ethics committee of Shaanxi Provincial People’s Hospital and conducted in line with the requirements of the Declaration of Helsinki. Informed consent was not required as this was a retrospective study in which all patient data was de-identified prior to use.
Lipid measurement
Blood samples were obtained after an overnight fast. After collection, blood samples were rapidly centrifuged at 1800 × g for 10 minutes and analyzed using the immunoturbidimetric assay (Aidian, Espoo, Finland). All measurements were performed in the laboratory of Shaanxi Provincial People’s Hospital. Higher baseline lipid levels (hyperlipidemia) were defined as LDL-C ≥2.6 mmol/L (100 mg/dL) or TG ≥1.7 mmol/L (150 mg/dL) at the time of ACS onset. 6
Clinical data collection
The baseline characteristics and clinical outcomes of the patients were collected by experienced physicians. Finally, the data were entered and maintained in a network database (Likang Times Technology Co. Ltd, Beijing, China). Raw data were checked using the double entry method. Data were entered into the database only when the values of two entries were consistent. Otherwise, the system automatically flagged an error to permit correction by checking the raw data. Double entry of the same sample was performed by different researchers.
Definitions
ACS was defined as high-risk unstable angina, non-ST elevated myocardial infarction (MI), or ST-elevated MI. MI was defined as acute myocardial injury with clinical evidence of acute myocardial ischemia and the detection of a rise and/or fall of cardiac troponin values with at least one value exceeding the 99th percentile of the upper reference limit. 16 The endpoint of MACE consisted of cardiovascular death, MI, ischemia-driven revascularization, progression to New York Heart Association (NYHA) functional class III or IV, and stroke. Ischemia-driven revascularization was defined as repeat percutaneous coronary intervention or coronary artery bypass grafting. 17 NYHA functional class III consisted of cardiac disease resulting in marked limitation of physical activity in patients who were otherwise comfortable at rest. In this group, less than ordinary activity caused fatigue, palpitation, or dyspnea. NYHA functional class IV consisted of patients with cardiac disease resulting in an inability to perform any physical activity without discomfort. Symptoms were present even at rest or on minimal exertion. If any physical activity is undertaken, discomfort was increased.
Statistical analysis
Participants were divided into four groups according to the presence of hyperlipidemia and frequency of statin use (group 1, hyperlipidemia with inconsistent statin use; group 2, no hyperlipidemia with inconsistent statin use; group 3, no hyperlipidemia with consistent statin use; and group 4, hyperlipidemia with consistent statin use). Patients did not consistently have previous histories of statin use at admission. Statin therapy was started at the time of ACS onset 18 and was newly provided after enrollment. Consistent statin use was defined as treatment with statins after admission and discharge and confirmed statin use at each interval. The group of patients who did not always use statins included patients who never used statins and those with inconsistent use. The baseline characteristics among the four groups were analyzed using analysis of variance for parametric variables, the Kruskal–Wallis test for nonparametric variables, and the chi-squared test for categorical variables. The cumulative event curves of MACE were derived using the Kaplan–Meier method, and the log-rank test was used for comparisons. The impact of baseline lipid levels and sustained statin therapy on MACE risk were estimated using univariate and multivariate Cox proportional hazards regression models. Model 1 was unadjusted. Model 2 was adjusted for age, sex, smoking, and body mass index. Model 3 was adjusted for age, sex, smoking, body mass index, diabetes, hypertension, prior MI, and atrial fibrillation. Model 4 was adjusted for age, sex, smoking, body mass index, diabetes, hypertension, prior MI, atrial fibrillation, high-sensitivity C-reactive protein (hs-CRP), N-terminal pro B type natriuretic peptide, Killip classification, consistent aspirin use, consistent clopidogrel use, consistent beta-blocker use, consistent angiotensin-converting enzyme inhibitor or angiotensin receptor blocker use, and revascularization at baseline. Furthermore, we also performed multivariate Cox analysis of MACE by subgroup.
All statistical testing was two-sided. Results were considered statistically significant at P < 0.05. All analyses were performed using PASW Statistics 20.0 software (IBM SPSS Statistics, New York, USA).
Results
Baseline characteristics
In total, 729 eligible patients visited our institution during the study period. Patients with incomplete data (21 patients), NYHA functional class III or IV (10 patients), active infection (7 patients), autoimmune or inflammatory disease (6 patients), kidney disease (estimated glomerular filtration rate <60 mL/min/1.73 m2) (4 patients), and cancer (2 patients) were excluded. Forty-three patients (6.3%) were lost to follow-up in the study. The final study cohort consisted of 636 patients (Supplemental Figure S1). The baseline characteristics of the study patients are listed in Table 1. The mean duration of follow-up was 4.2 years (interquartile range, 4.1 to 4.4 years). Patients ranged in age from 25 to 80 years old (mean, 60.42 ± 9.83 years), and 66.8% of patients were male. Patient age was higher in groups 2 and 3 (groups 1 to 4, 59.26 ± 10.31, 61.30 ± 10.12, 61.96 ± 9.20, and 58.14 ± 9.87 years, respectively, P <0.001), whereas diastolic blood pressure was lower in these groups (79.85 ± 9.78, 77.88 ± 11.17, 76.83 ±10.45, and 79.56 ± 11.10 mmHg, respectively, P = 0.008). Groups 3 and 4 featured higher rates of aspirin (groups 1 to 4, 90.6, 88.5, 99.6, and 99.4%, respectively, P <0.001) and clopidogrel use (53.8, 54.8, 81.3, and 76.8%, respectively, P <0.001) and higher rates of revascularization at baseline (65.1, 64.4, 76.3, and 77.4%, respectively, P = 0.016). The treatments received by the patients after enrollment are listed in Table S1. Patients in groups 3 and 4 had higher rates of consistent aspirin (groups 1 to 4, 73.6, 64.4, 90.5, and 89.6%, respectively, P <0.001) and beta blocker use (32.1, 35.6, 64.5, and 65.9%, respectively, P <0.001; Table S1).
Baseline clinical characteristics of the study patients according to the presence of hyperlipidemia and statin use.

Continuous variables are presented as the mean ± SD, and categorical variables are presented as numbers or percentages.
a No patients were classified as Killip IV.
b Included percutaneous coronary intervention and coronary artery bypass grafting.
ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; BMI, body mass index; CRE, creatinine; DBP, diastolic blood pressure; HDL-C, high-density lipoprotein cholesterol; hs-CRP, high-sensitivity C-reactive protein; LDL-C, low density lipoprotein cholesterol; LVEDD, left ventricle end-diastolic diameter; LVEF, left ventricle ejection fraction; MI, myocardial infarction; Non-STEMI, non-ST segment elevation myocardial infarction; NT-proBNP, N-terminal pro B type natriuretic peptide; SBP systolic blood pressure; STEMI, ST segment elevation myocardial infarction; TC, total cholesterol; TG, triglyceride; UA, uric acid.
Clinical outcomes
During 4.2 ± 0.3 years of follow-up, 98 cases of MACE (15.4%) were recorded, including MI in 8 patients (1.3%), ischemia-driven revascularization in 73 patients (11.5%), progression to NYHA class III or IV in 17 patients (2.7%), and stroke in 14 patients (2.2%). During follow-up, the rates of MACE in groups 1, 2, 3, and 4 were 28.3 (30/106), 23.1 (24/104), 13.0 (34/262), and 6.1% (10/164), respectively (P <0.001; Table S2). Compared with the findings in group 1, the cumulative incidence of MACE gradually decreased in groups 2 to 4 (all P <0.001; Figure 1). The cumulative event curves of ischemia-driven revascularization were similar to those of MACE (P <0.001). The cumulative event curves of MI, ischemia-driven revascularization, progression to NYHA III or IV, and stroke are presented in Figure S2.

The cumulative incidence of MACE. Compared with the findings in group 1, the cumulative incidence of MACE gradually decreased in groups 2, 3, and 4 (P < 0.001).
We used univariate and multivariate Cox regression models to reveal the impact of hyperlipidemia and sustained statin use on MACE risk in patients with ACS. In univariate Cox regression analysis (Model 1), using group 1 as the reference, the hazard ratios (HRs) for MACE in groups 3 and 4 were 0.44 (95% confidence interval [CI] = 0.27–0.73, P = 0.001) and 0.19 (95% CI = 0.09–0.39, P <0.001), respectively. Similarly, multivariate analysis illustrated that patients in groups 3 and 4 had lower risks of MACEs than those in group 1 in Models 2 (group 3, HR = 0.45, 95% CI = 0.27–0.74, P = 0.002; group 4, HR =0.19, 95% CI = 0.09–0.39, P <0.001), 3 (group 3, HR = 0.44, 95% CI = 0.27–0.72, P = 0.001; group 4, HR = 0.18, 95% CI = 0.09–0.37, P <0.001), and 4 (group 3, HR = 0.49, 95% CI = 0.29–0.82, P = 0.007; group 4, HR = 0.21, 95% CI = 0.10–0.45, P <0.001). There was no significant difference in the relative risk of MACE between groups 1 and 2 (Table 2).
Univariate and multivariate Cox analyses according to the presence of hyperlipidemia and statin use.

a Model 1: Unadjusted.
b Model 2: Adjusted for age, sex, smoking, and body mass index.
c Model 3: Adjusted for age, sex, smoking, body mass index, diabetes, hypertension, prior myocardial infarction, and atrial fibrillation.
d Model 4: Adjusted for age, sex, smoking, body mass index, diabetes, hypertension, prior myocardial infarction, atrial fibrillation, high-sensitivity C-reactive protein, N-terminal pro B type natriuretic peptide, Killip classification, consistent aspirin use, consistent clopidogrel use, consisted beta-blocker use, consistent angiotensin-converting enzyme inhibitor or angiotensin receptor blocker use, and revascularization at baseline.
e compared with the hyperlipidemia and inconsistent statin use.
CI, confidence interval; HR, hazard ratio; MACE, major adverse cardiac events.
Compared with the findings in group 1, subjects in groups 3 and 4 had lower risks of ischemia-driven revascularization. Zero cardiovascular deaths and eight cases of MI were recorded during follow-up. These low rates did not permit further analysis (Table S3)
Subgroup analysis
In the univariate Cox regression model (Model 1), patients in group 3 had a lower risk of MACE than those in group 2 (HR = 0.56, 95% CI = 0.33–0.94, P =0.029). The lower risk of MACE in group 3 than in group 2 remained after adjustment for confounders (Model 2, HR = 0.58, 95% CI = 0.34–0.98, P = 0.042; Model 3, HR = 0.55, 95% CI = 0.32–0.94, P = 0.028; Model 4, HR = 0.53, 95% CI = 0.30–0.95, P = 0.031; Table 3 and Figure 2a).
Multivariate Cox analysis of MACE by subgroup.
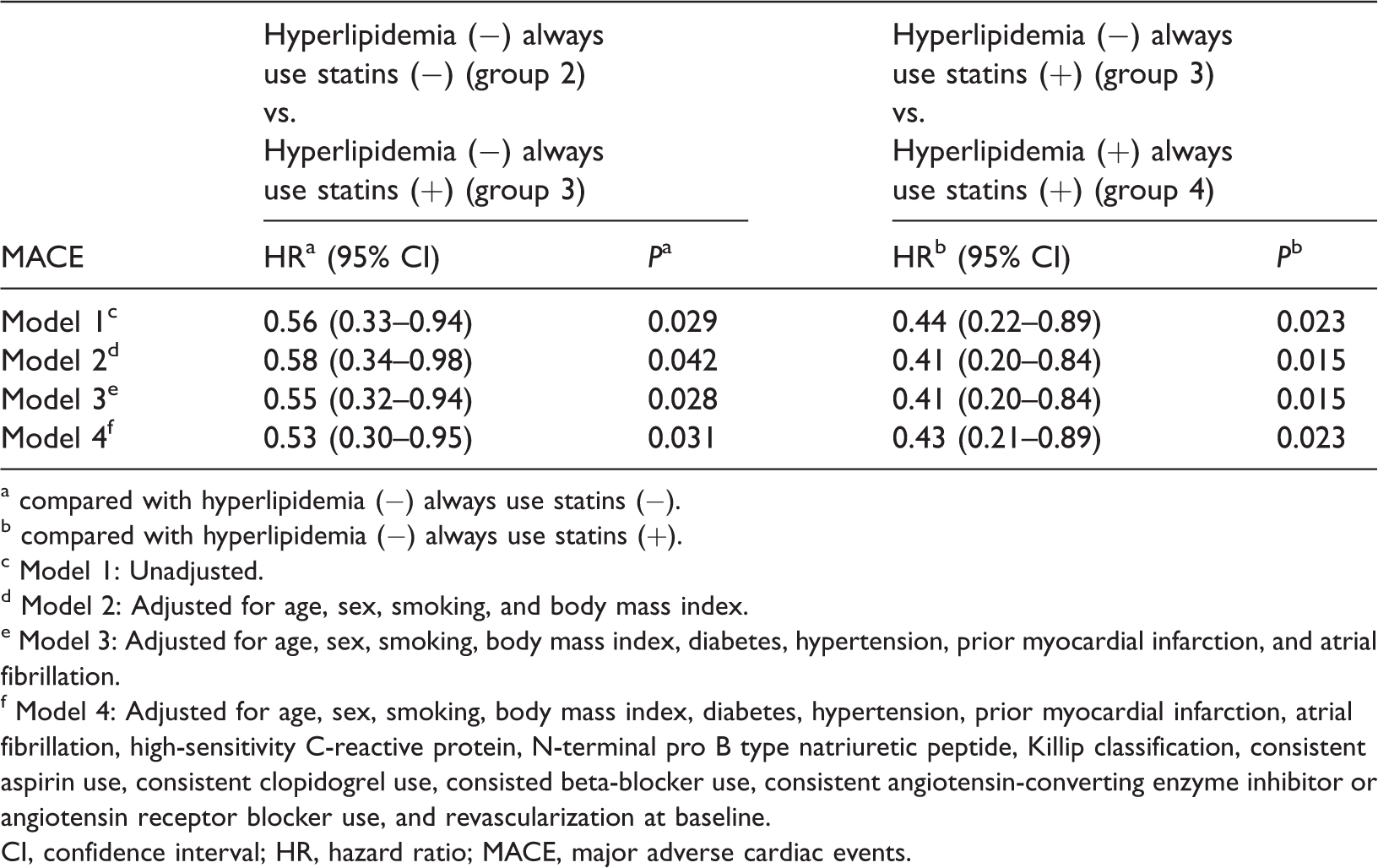
a compared with hyperlipidemia (−) always use statins (−).
b compared with hyperlipidemia (−) always use statins (+).
c Model 1: Unadjusted.
d Model 2: Adjusted for age, sex, smoking, and body mass index.
e Model 3: Adjusted for age, sex, smoking, body mass index, diabetes, hypertension, prior myocardial infarction, and atrial fibrillation.
f Model 4: Adjusted for age, sex, smoking, body mass index, diabetes, hypertension, prior myocardial infarction, atrial fibrillation, high-sensitivity C-reactive protein, N-terminal pro B type natriuretic peptide, Killip classification, consistent aspirin use, consistent clopidogrel use, consisted beta-blocker use, consistent angiotensin-converting enzyme inhibitor or angiotensin receptor blocker use, and revascularization at baseline.
CI, confidence interval; HR, hazard ratio; MACE, major adverse cardiac events.

The cumulative incidence of MACE in each subgroup. (a) Patients without hyperlipidemia who always used statins (group 3) had a lower risk of MACE than those without hyperlipidemia and inconsistent statin use (group 2). (b) Patients with hyperlipidemia and consistent statin use (group 4) had a lower risk of MACE than those in group 3.
More interestingly, compared with the findings in patients in group 3, those in group 4 had a 56% lower risk of MACE (HR = 0.44, 95% CI = 0.22–0.89, P = 0.023). This reduced risk of MACE was not attenuated after adjustment for confounders (Model 2, HR = 0.41, 95% CI = 0.20–0.84, P = 0.015; Model 3, HR = 0.41, 95% CI = 0.20–0.84, P = 0.028; Model 4, HR = 0.43, 95% CI = 0.21–0.89, P = 0.023; Table 3 and Figure 2b).
Discussion
In this retrospective cohort study, we found that sustained statin therapy was linked to a lower risk of MACE in patients with ACS, consistent with previous findings. Notably and interestingly, patients with higher baseline lipid levels more greatly benefited from sustained statin therapy than those with lower baseline lipid levels.
A large number of clinical trials have demonstrated that statin therapy could reduce long-term mortality in patients with coronary heart disease.11,13,19,20 However, the lipid profiles most greatly associated with benefits from statin therapy have not been established. Our results demonstrated that patients with ACS and higher baseline lipid levels more greatly benefited from sustained statin therapy than those with lower baseline lipid levels. The association between baseline lipid profiles and the development of adverse outcomes of ACS were assessed using multivariable Cox proportional hazards regression. To remove the effect of the drug, we followed patients closely and assessed drug treatment including baseline and follow-up analyses. We also used several Cox proportional hazards regression models (Models 1–4) to examine the association between baseline lipid levels and the risk of adverse outcomes in patients with ACS. All analyses demonstrated that sustained statin therapy may decrease the risk of MACE in patients with ACS, especially among those patients with higher baseline lipid levels.
The influence of baseline lipid levels on the clinical benefit of lipid-lowering therapy remains controversial. On the one hand, the HPS trial revealed that statin therapy was beneficial in patients with baseline LDL-C levels of less than 100 mg/dL. 20 Furthermore, the LIPID and CARDS trials demonstrated that statin therapy reduced the risk of cardiovascular events, and the finding was not associated with baseline lipid levels.9,21 On the other hand, the PROVE IT–TIMI 22 trial revealed that the baseline LDL-C level is an important predictor of the benefit of intensive therapy compared with moderate lipid-lowering therapy. 22 However, a key limitation of these findings is that therapy was not randomized according to low and high pretreatment lipid levels. Sub-analysis of the Extended-ESTABLISH trial demonstrated that early atorvastatin therapy reduced the 1-year MACCE rate in patients with baseline LDL-C ≥ 100 mg/dL. 15 These findings accord with our results that patients with higher baseline lipid levels have a lower risk of MACE than those with lower baseline lipid levels during statin therapy. The revascularization rate in our study was lower than that reported previously. In our study, all patients were of Chinese Han ethnicity. The discrepancy of the revascularization rate may be attributable to the economic and cultural backgrounds of patients in Shaanxi Province, which is an underdeveloped area in western China in which many patients cannot receive contemporary management strategies. 23
The reasons for the reduced benefit of statin therapy in patients with lower baseline lipid levels are not fully understood. The benefit of intensive statin therapy progressively decreases as the baseline LDL-C levels decrease. 22 Early intensive lipid treatment might not be required in patients with lower baseline lipid levels. The milder management required in patients with lower baseline lipid levels might result in fewer side effects, reduced drug costs, and higher adherence to therapy.24,25 However, in the secondary prevention of ACS, statins are the most promising and effective therapies for stabilizing vulnerable coronary plaques. Patients with lower baseline lipid levels should pay more attention to other coronary risk factors, such as lifestyle factors, which may have a more important role in the risk of future events than lipid levels.
Limitations
There were some limitations in our study. This was a retrospective cohort study, and our population was small. The patients enrolled in this study were recruited from a single center, and they resided in an underdeveloped area in western China, which may have resulted in biases. In addition, 6.3% of patients were lost to follow-up in the present study, which might introduce biases. hs-CRP levels were measured at enrollment, but this variable was not measured at the time at which patients’ conditions stabilized. In addition, lipid levels were only measured at the onset of ACS. We did not perform serial measurements of lipid levels during follow-up in this study. These factors may limit the generalizability of our findings.
Conclusion
Our results illustrated that sustained statin therapy is associated with a lower risk of adverse outcomes in patients with ACS, especially those with higher baseline lipid levels.
Supplemental Material
sj-pdf-1-imr-10.1177_0300060520965848 - Supplemental material for Higher baseline lipid levels amplify the benefit of secondary prevention therapy with statins in Chinese patients with acute coronary syndrome
Supplemental material, sj-pdf-1-imr-10.1177_0300060520965848 for Higher baseline lipid levels amplify the benefit of secondary prevention therapy with statins in Chinese patients with acute coronary syndrome by Ling Zhu, Ying Liu, Wei Zhang, Zhu Zhang, Liqin Zhou, Hong Zhang, Yong Zhang, Fuqiang Liu, Peng Liu, Zhongwei Liu and Junkui Wang in Journal of International Medical Research
Footnotes
Acknowledgements
We appreciate the help and support of all of the participants involved in the study.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (grant No. 81700401), Natural Science Basic Research Program of Shaanxi (grant Nos. 2018JQ8053 and 2017KJXX-70), Science and Technology Program of Xi’an, China (grant No. 201805094YX2SF28(12)), Free Exploration and Innovation Project (Teacher Category) of Xi’an Jiaotong University (No. xzy012019127), Chinese Cardiovascular Association-Access fund (No. 2019-CCA-ACCESS-052), and Special Financial Grant from China Postdoctoral Science Foundation (grant No. 2017T100789).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.