
Abstract
A sizable proportion of coronary artery disease (CAD) patients undergoing percutaneous coronary intervention (PCI) with stent implantation have an indication for treatment with oral anticoagulant therapy (OAC). The coexistence of atrial fibrillation (AF) and the need for PCI expose patients to a higher risk of developing thrombotic complications, and a multitargeted antithrombotic treatment strategy, addressing both platelet- and coagulation-mediated triggering mechanisms of thrombosis, is necessary for ensuring full protection from ischemic hazards. The increased bleeding risk identified with triple antithrombotic therapy has driven the search for alternative treatment modalities and pharmacological combination strategies aimed at achieving an optimal balance between safety and efficacy in this complex clinical scenario. Over a short time period, the paradigms surrounding the management of patients undergoing PCI who require OAC have substantially evolved. In this review, we summarize and critically evaluate the results of recent randomized clinical trials investigating the pharmacological management of patients who, in addition to antiplatelet therapy, have an indication for OAC treatment before or at the time of a PCI procedure.
Keywords
Introduction
A sizable proportion of coronary artery disease (CAD) patients undergoing percutaneous coronary intervention (PCI) with stent implantation have an indication for treatment with oral anticoagulant (OAC) therapy.1,2 The most common indication for OAC therapy in this group of patients, ranging approximately from 5% to 8% of all PCI candidates, 3 is represented by the prevention of stroke and thromboembolism due to atrial fibrillation (AF). In addition to OAC treatment, coronary stenting requires antiplatelet therapy to prevent the clinical sequelae of stent thrombosis (ST) and to reduce the burden of ischemic recurrences (i.e. myocardial infarction). 4 In combination, the coexistence of AF and the need for PCI expose patients to a higher risk of developing thrombotic complications, and a multitargeted antithrombotic treatment strategy, addressing both platelet- and coagulation-mediated triggering mechanisms of thrombosis, is necessary to ensure full protection from ischemic hazards. Importantly, global epidemiological trends, characterized by the progressive aging of the general population, 5 are expected to increase the frequency of managing antithrombotic therapy among the elderly. 6 Indeed, the burden of AF prevalence in the general population is expected to increase, partly as a consequence of the trends toward an aging population.7,8
AF and CAD share a number of pathophysiological mechanisms, that are reflected in the coexistence of CAD and AF in approximately 20–30% of patients. 1 With PCI being preferentially offered as a revascularization strategy in patients with CAD, in particular, the elderly, 9 the challenging therapeutic clinical context of coronary stenting in anticoagulated patients will be increasingly encountered by physicians. Triple antithrombotic therapy (TT), consisting of OAC, aspirin, and a P2Y12 inhibitor, has been advocated and endorsed by international guidelines as a strategy that provides full protection from ischemic risk (class IIa, level of evidence B). 10 However, TT, especially with prolonged use, has been associated with an increased risk of bleeding which, similarly to the risk of experiencing an ischemic recurrence, places patients at risk, worsens clinical outcomes, and increases the risk of death.11,12 The growing awareness of bleeding as an important determinant of prognosis has driven the search for alternative treatment modalities and pharmacological combination strategies aimed at achieving an optimal balance between safety and efficacy (also known as a net clinical benefit) in this complex clinical scenario.
Recently, the clinical advent of nonvitamin K antagonists [novel oral anticoagulants (NOACs)] has represented a major step forward toward safety. 13 In addition, lowering the intensity of antiplatelet treatment by removing aspirin has been demonstrated to be safe. 14 Over a short time period, the paradigms surrounding the management of patients undergoing PCI who require OAC have substantially evolved. A critical overview of this rapidly evolving landscape is useful to acknowledge the potential incremental clinical benefits conveyed by the newer treatment strategies while avoiding the caveats of a ‘tout court’ interpretation of the newly generated evidence which might result in the dangerous pharmacological undertreatment of patients. Based on this information, in this review we summarize and critically evaluate the evolving paradigms in the management of patients who have an indication for OAC treatment before or at the time of a PCI procedure. The management of patients who develop an indication for OAC treatment after PCI has been addressed elsewhere 1 and is beyond the scope of this review.
Pathophysiology and temporal evolution of thromboembolic risk in AF patients undergoing PCI
In anticoagulated patients undergoing coronary stenting, activation of the coagulation system and platelets influences the risk of thrombotic complications, including stroke and ST. 4 Although the two pathways have different points of interconnection and cannot be considered independent, 15 each respective mechanism plays a more important role in the processes that leads to thrombus formation. Low shear-stress and blood stasis in the left atrial appendage promotes thrombus formation via activation of the coagulation cascade. 16 The intrinsic pathway as initiated by the Von Willebrand factor/factor VIII interaction, has been identified as central in this process. 17 In contrast, ST occurs in high shear-stress conditions where platelet activation is of the highest importance. Other factors, including the endothelialization and thickness of the stent struts, the stent implantation technique (i.e. stent malapposition, edge dissection), the biocompatibility/integrity of the polymer, and the characteristics of the underlying plaque, are important in modulating the risk of ST. 18 Stent-specific factors influencing the risk of ST have been largely addressed by the newer generations of drug-eluting stents (DES) which, in contrast to bare metal stents and first-generation DES, have robustly demonstrated improved safety and efficacy with low rates of ST and in-stent restenosis. 19 Today, the concept of improved safety with the use of bare metal stents is outdated and, therefore, current guidelines recommend the implantation of newer generation DES as a default approach.20,21
Data from landmark trials have demonstrated the superiority of OAC treatment versus antiplatelet therapy for stroke prevention 22 and the superiority of dual antiplatelet therapy (DAPT), consisting of aspirin and a P2Y12 inhibitor, over OAC treatment for ST prevention. 23 By tackling the specific pathways involved in thrombus generation, OAC therapy is, therefore, required to prevent stroke while antiplatelet therapy is required to reduce the risk of ST.
Thromboembolic risk dynamically evolves over time in anticoagulated patients undergoing PCI. While stroke risk in patients with AF with an indication for OAC therapy potentially increases over time, the risk of ST with newer DES follows a more predictable temporal pattern characterized by the higher risk of ST mostly in the early weeks or months following stent deployment. 24 Data from the real-world registries have corroborated this understanding by highlighting a temporal clustering of ST cases in a vulnerable time window which spans the time just after stent implantation. 25 In a large cohort of patients from the Swedish Coronary Angiography and Angioplasty Registry, combining 882 cases of definite ST among 73,798 implanted stents (including both bare metal stent and DES), the majority of ST events (49%) occurred in the first 30 days after PCI. 26 A similar temporal pattern for ST incidence has been reported in the Dutch ST Registry with 320 out of 437 ST cases encountered in the first 30 days after stent implantation. 27 Of interest, in this latter analysis, the lack of clopidogrel therapy in the first 30 days after PCI was associated with a markedly increased risk of ST [hazard ratio (HR) 36.5, 95% confidence interval (CI): 8.0–167.8].
The potential accrual pattern of stroke risk over time represents the rationale for long-term OAC administration in AF patients. In a large cohort of patients with newly-diagnosed AF (n = 14,606) who were followed for a mean time of 3.24 years, the CHA2DS2-VASc score, a marker of stroke risk, progressively increased over time. 28 The well-known axiom ‘AF begets AF’ summarizes the consequences of the structural remodeling process of the left atrium frequently seen in AF patients. 29 Indeed, over time the left atrium undergoes progressive enlargement and loss of the atrial contractile function, finally resulting in an increased burden of AF, local blood stasis, and a higher risk of developing local thrombosis. 30
The time-varying patterns of thromboembolic risk (Figure 1) open the window for temporally tailored antithrombotic treatment strategies based on the expected dynamics of risk evolution after the index procedure. Indeed, the first phases after coronary stenting remain a particularly vulnerable period of high thrombotic risk requiring, when feasible and safe, a higher intensity of antiplatelet treatment. Subsequently, when the cumulative thrombotic risk is lower, modulation of the intensity of therapy should be preferentially directed toward safety prioritization and bleeding avoidance.
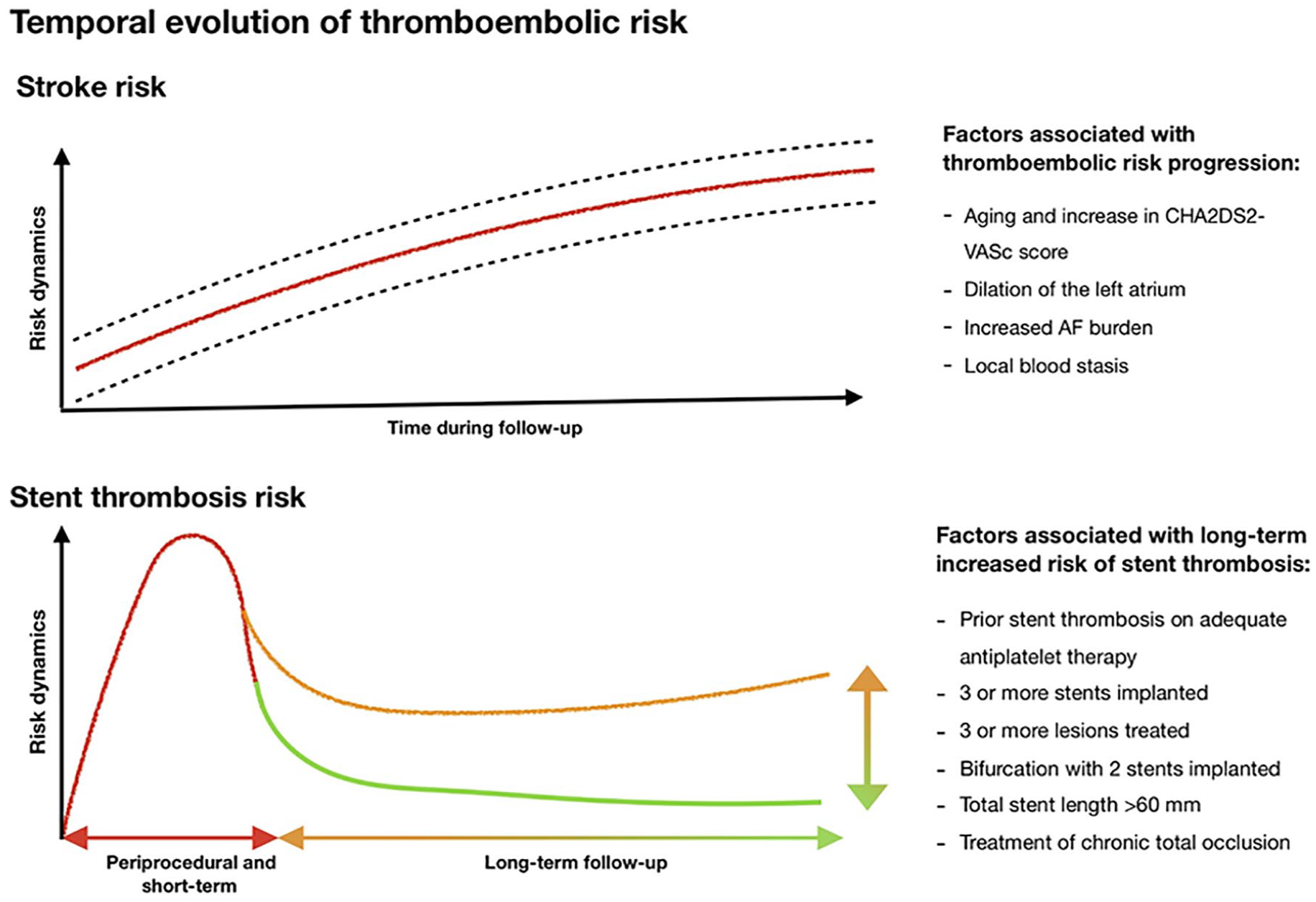
Evolution of thromboembolic risk and stent thrombosis in patients with atrial fibrillation and coronary artery disease requiring stent implantation.
Beyond TT: the rationale and initial evidence
The increased risk of bleeding with TT has been well characterized in the literature. Data from the Danish national registries, including a total of 40,812 patients with first-time myocardial infarction (MI) from 2000 to 2005, have demonstrated an almost fourfold increased risk of fatal and nonfatal bleeding with TT when compared with treatment with aspirin alone. 12 The increased risk of bleeding with TT, although more sizable in the first period of treatment, was continually elevated during 1 year of follow-up when compared with less-intensive treatment strategies. 11 In addition, a pooled analysis of observational studies, encompassing 10 studies and a total of 1349 patients receiving TT, confirmed the high absolute rates of bleeding with TT by reporting a weighted mean incidence of major bleeding at 30 days of 2.2%. 31
In addition, the prognostic effect of bleeding has been the subject of extensive investigation. While traditionally clinicians were mostly afraid of ischemic recurrences, bleeding and its prognostic consequences have gained increasing importance over time. 32 Today, bleeding and ischemic events are thought to be substantially equivalent in terms of prognosis. Indeed, data from the Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation trial (ARISTOTLE) have shown a 12-fold increased risk of death, ischemic stroke, or MI within 30 days after a major (nonintracranial) bleeding. 33 In addition, a pooled analysis of the RE-LY and ACTIVE trials showed that experiencing an extracranial bleeding was associated with an adjusted HR for mortality of 4.60 (95% CI 4.16–5.09). 34 Such risk estimates for subsequent mortality is not dissimilar to those seen after MI or an ischemic stroke (HR 6.19 and 6.46, respectively). Ultimately, a benefit in mortality has been observed when anticoagulation strategies that lower the risk of bleeding are implemented in patients with AF. 35 Bleeding associated with antiplatelet therapy carries a substantially increased risk of death. In the Acute Catheterization and Urgent Intervention Triage Strategy (ACUITY) trial, which included 13,819 patients with moderate and high-risk acute coronary syndrome (ACS) undergoing invasive management, experiencing either recurrent MI or major bleeding resulted in a similar risk for subsequent mortality at 1 year (approximately a threefold increased risk). 36 While the timing of a recurrent MI was more important in influencing the subsequent risk of death (with recurrent MI within the first days after the index event carrying a higher risk of death), the prognostic impact of bleeding was stable during the first year after the initial event. These findings were substantiated by the results of the Assessment of Dual Antiplatelet Therapy With Drug-Eluting Stents (ADAPT-DES) registry which showed an even higher risk of 2-year mortality in patients with postdischarge bleeding (adjusted HR 5.03) when compared with patients experiencing postdischarge MI (adjusted HR 1.92). 37
The identification of prolonged TT as a driver of bleeding and the understanding of bleeding as a driver of poor prognosis have paved the way for investigating the safety and efficacy of alternative treatment strategies in anticoagulated patients undergoing PCI.38,39 The What is the Optimal antiplatElet and anticoagulant therapy in patients with oral anticoagulation and coronary StenTing (WOEST) trial was the first randomized clinical trial (RCT) putting into question one of the central principles in cardiovascular pharmacotherapy, namely, the use of aspirin after stenting. 14 WOEST was an open-label, multicenter trial enrolling a total of 573 patients who were randomized in a 1:1 ratio to TT [consisting of vitamin K antagonists (VKA), aspirin and clopidorel)] or DT (consisting of clopidogrel and VKA). The primary endpoint of WOEST was any bleeding (including major and minor bleeding) at 1 year. By the end of the study observation period, VKA was being used in more than 90% of patients in both groups and clopidogrel was being used by 80.6% of patients in the DT group. Aspirin and clopidogrel were being used by 66.5% and 78.9% of patients in the TT group, respectively. WOEST demonstrated a remarkable reduction of bleeding in patients randomized to DT versus TT (19.4% versus 44.4%; HR 0.36, 95% CI 0.26–0.50, p < 0.0001). However, the treatment effect on bleeding was mostly driven by a reduction in the rate of minor bleedings. The risk of ischemic complications was even reduced in the DT group when compared with patients treated with TT, although the study was underpowered for efficacy endpoints.
Building on the concept of minimizing the exposure to TT to limit the risk of bleeding, the Triple Therapy in Patients on Oral Anticoagulation After Drug Eluting Stent Implantation (ISAR-TRIPLE) trial compared a regimen of 6 weeks versus 6 months TT in patients undergoing PCI and coronary stenting. 40 The primary endpoint of the trial was a composite of death, MI, definite ST, stroke, or thrombolysis in MI (TIMI) major bleeding at 9 months after randomization and 614 patients were randomized in a 1:1 ratio to the two TT temporal regimens. No differences in the rate of the primary endpoint were seen between the two groups. Of interest, a landmark analysis from 6 weeks to 9 months (when the treatment strategies actually differed between the two groups) showed an increased risk of bleeding in patients randomized to the prolonged TT arm versus patients who, after 6 weeks, dropped clopidogrel and were treated with warfarin and aspirin.
Although the WOEST and ISAR-TRIPLE trials had important limitations including the limited sample size and the lack of power for assessing differences in low-frequency ischemic events, they provided evidence of enhanced safety with less intense antithrombotic treatment strategies in patients who required combined treatment with OAC and antiplatelet agents. No conclusions, however, could be drawn from these trials regarding efficacy endpoints.
The clinical advent of non-VKAs (NOACs)
A major breakthrough in the pharmacological management of AF patients requiring OAC therapy has been represented by the introduction of NOACs into clinical practice. The family of NOACs today includes several drugs (e.g. dabigatran, apixaban, rivaroxaban, edoxaban) that have been clinically tested versus VKAs in a series of large, multicenter RCTs.41–44 The characteristics of RCTs investigating the safety and efficacy of NOACs are summarized in Table 1. In aggregate, trials of NOACs have demonstrated at least comparable efficacy versus conventional VKA therapy for the prevention of thromboembolic events and improved safety with a significantly lowered risk of bleeding. A meta-analysis of RCTs comparing NOACs and warfarin therapy in AF patients requiring OAC therapy (12 studies, 77,011 patients) demonstrated a significantly lower risk of major bleeding [odds ratio (OR) random effects 0.76, 95% CI 0.62–0.93] and intracranial hemorrhage (OR fixed effects 0.48, 95% CI 0.40–0.57) with NOACs use. 45 No difference in the risk of experiencing ischemic stroke was seen between patients treated with warfarin and NOACs (OR random effects 0.98, 95% CI 0.82–1.16). Of interest, a lower risk of death was seen in patients receiving NOACs (OR fixed effects 0.86, 95% CI 0.82–0.91). Lower bleeding rates have been clearly identified as the causal mechanism leading to reduced mortality with NOACs use. 46 These results further reinforce the importance of implementing a series of bleeding avoidance strategies to improve clinical outcomes in anticoagulated patients. Results of NOAC trials have been rapidly incorporated into clinical guidelines with a class I, level of evidence A recommendation for NOACs preference over VKA use in patients with nonvalvular AF and no mechanical heart valves. 10 Obviously, the safety profile of NOACs has fostered the interest in the use of these agents in patients who, in addition to OAC treatment, require antiplatelet therapy.
Characteristics of pivotal trials of non-VKAs in patients with AF.
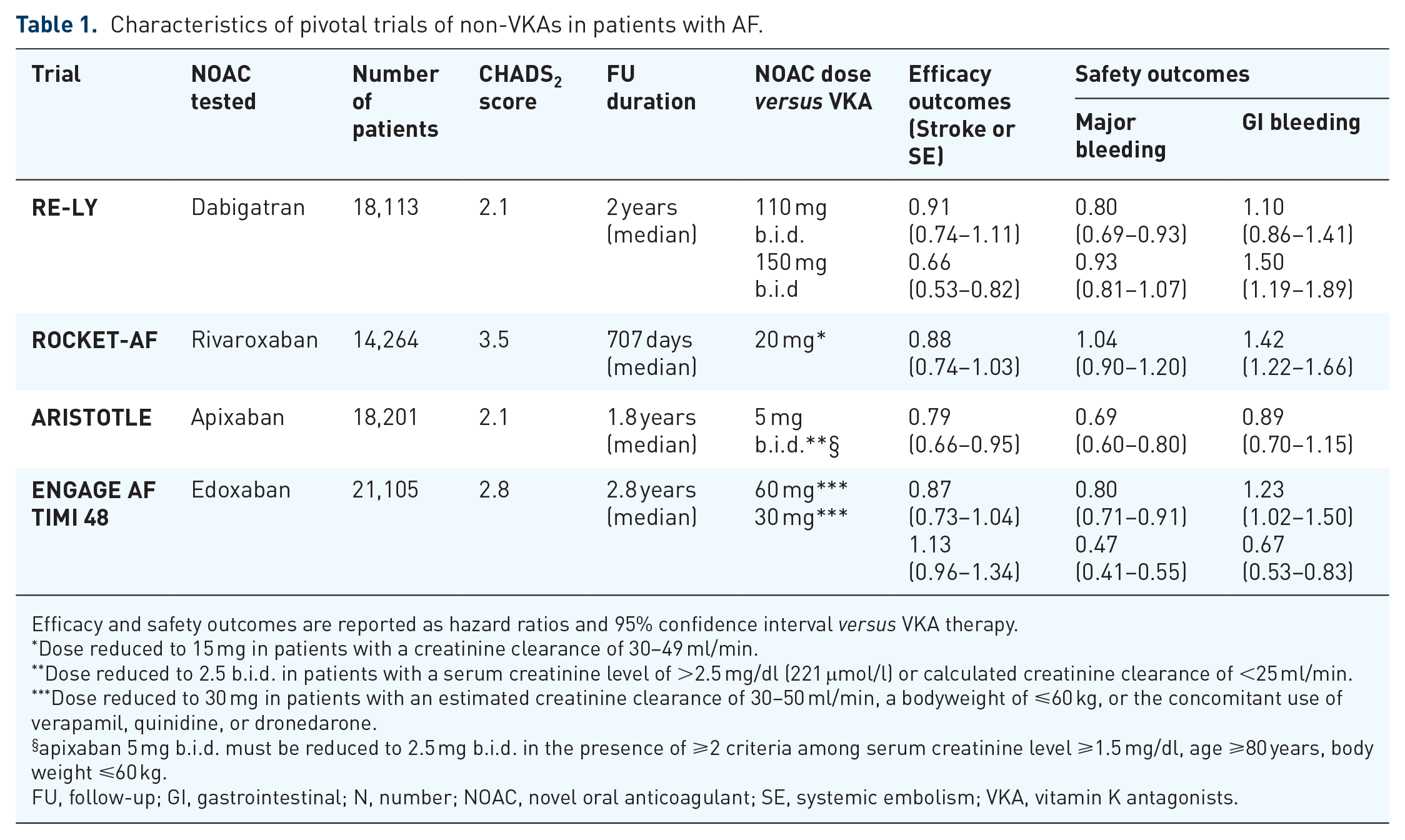
Efficacy and safety outcomes are reported as hazard ratios and 95% confidence interval versus VKA therapy.
Dose reduced to 15 mg in patients with a creatinine clearance of 30–49 ml/min.
Dose reduced to 2.5 b.i.d. in patients with a serum creatinine level of >2.5 mg/dl (221 μmol/l) or calculated creatinine clearance of <25 ml/min.
Dose reduced to 30 mg in patients with an estimated creatinine clearance of 30–50 ml/min, a bodyweight of ⩽60 kg, or the concomitant use of verapamil, quinidine, or dronedarone.
apixaban 5 mg b.i.d. must be reduced to 2.5 mg b.i.d. in the presence of ⩾2 criteria among serum creatinine level ⩾1.5 mg/dl, age ⩾80 years, body weight ⩽60 kg.
FU, follow-up; GI, gastrointestinal; N, number; NOAC, novel oral anticoagulant; SE, systemic embolism; VKA, vitamin K antagonists.
Entering the NOAC era for oral anticoagulation in patients undergoing PCI
Evidence on NOACs use in AF patients undergoing PCI has been recently generated. Four large randomized trials have yielded univocal results on the improved safety profile with NOACs use. The overall randomization scheme of these trials is summarized in Figure 2.
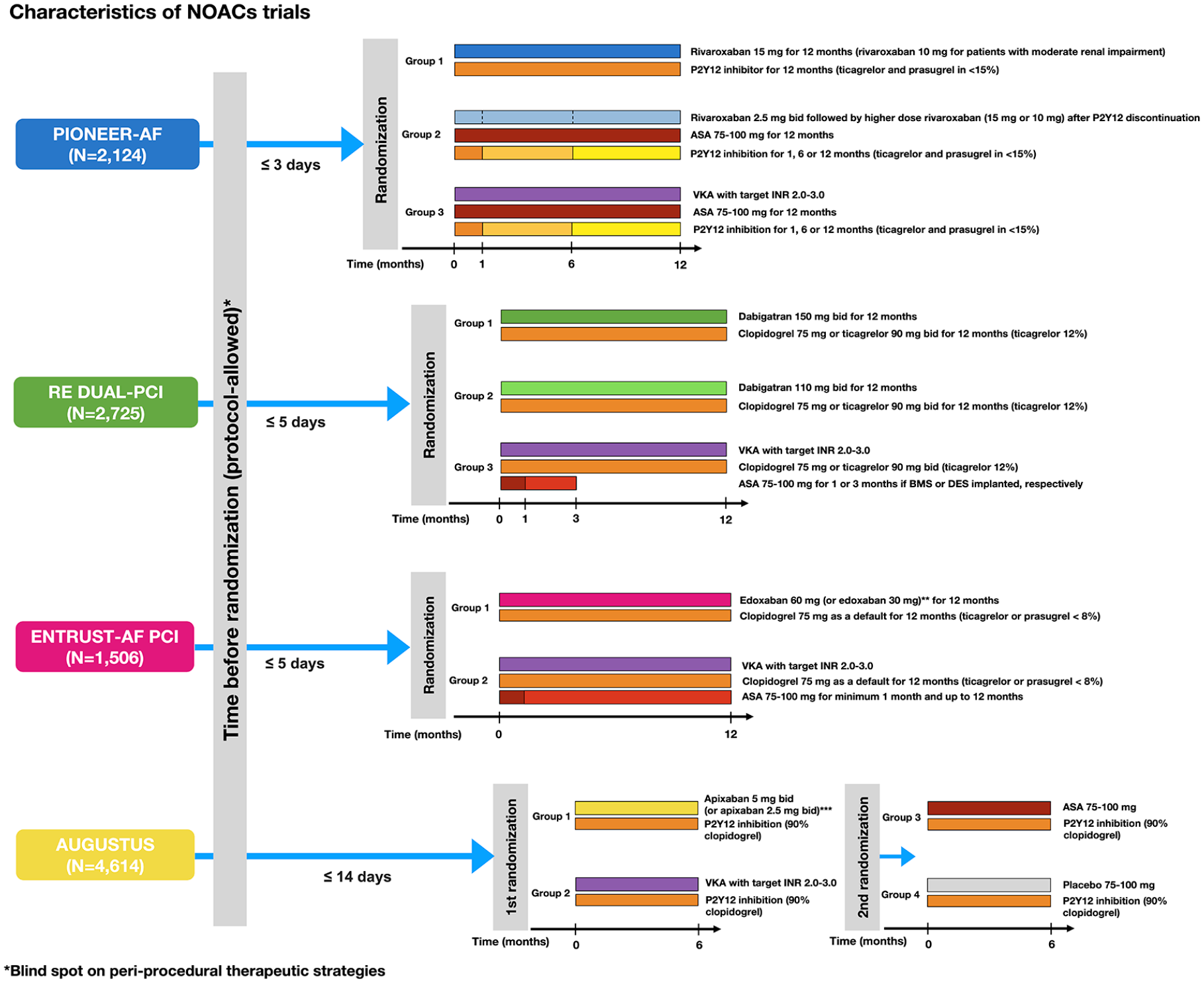
Design of trials investigating nonvitamin K antagonists in patients with atrial fibrillation undergoing PCI.
PIONEER-AF-PCI trial
The Open-Label, Randomized, Controlled, Multicenter Study Exploring Two Treatment Strategies of Rivaroxaban and a Dose-Adjusted Oral Vitamin K Antagonist Treatment Strategy in Subjects with Atrial Fibrillation who Undergo Percutaneous Coronary Intervention (PIONEER AF-PCI) trial investigated the use of rivaroxaban in patients with nonvalvular AF who underwent PCI with stent implantation. 47 Three treatment strategies have been compared in the study including standard dose rivaroxaban (15 mg once daily or 10 mg once daily for patients with moderate renal impairment defined as creatinine clearance of 30–50 ml/min) plus clopidogrel (WOEST-like strategy), standard TT consisting of VKA plus aspirin and a P2Y12 inhibitor (standard TT strategy), low-dose rivaroxaban (2.5 mg twice daily) plus aspirin and a P2Y12 inhibitor (low-dose rivaroxaban strategy). Both rivaroxaban doses investigated in the trial were lower than the recommended regimen for stroke and systemic embolism prevention in AF patients not undergoing PCI (recommended dose of 20 mg once daily, or 15 mg once daily in patients with creatinine clearance ⩽50 ml/min). The 2.5 mg twice-daily treatment strategy was based on the positive results (e.g. significant reduction of the composite endpoint of death from cardiovascular causes, MI, and stroke) seen with low-dose rivaroxaban therapy, in addition to antiplatelet treatment, in the Anti-Xa Therapy to Lower Cardiovascular Events in Addition to Standard Therapy in Subjects with Acute Coronary Syndrome–Thrombolysis in Myocardial Infarction 51 (ATLAS ACS 2–TIMI 51) trial. 48 DAPT duration in the two TT treatment arms of the study was left at the investigator’s discretion who could have opted for 1, 6, or 12 months. After a DAPT regimen of 1 or 6 months, single antiplatelet therapy with aspirin was administered. In addition, patients in the low-dose rivaroxaban arm received higher dose rivaroxaban after discontinuing DAPT (rivaroxaban 15 mg once daily or 10 mg for patients with moderate renal impairment). The primary endpoint of the study was clinically significant bleeding defined as the composite of TIMI major or minor bleeding and bleeding events requiring medical attention. Patients were randomized within 3 days after sheath removal. Before randomization, investigators were required to provide information on the intended duration of DAPT (1, 6, or 12 months) and the type of P2Y12 inhibitor (clopidogrel, prasugrel, and ticagrelor). Randomization was then performed in a 1:1:1 ratio and was stratified according to the intended duration of DAPT and the selected P2Y12 agent. A total of 2124 patients were included in the study. Clopidogrel was selected as a P2Y12 inhibitor in the majority of patients in the three groups (>93%). At 1 year, the rate of the primary safety endpoint was significantly higher in the standard TT strategy arm when compared with the WOEST-like and low-dose rivaroxaban arms (26.7% versus 16.8% and 18.0%, respectively; HR for WOEST-like versus standard TT of 0.59; 95% CI 0.47–0.76; p < 0.001 and HR for low-dose rivaroxaban versus standard TT of 0.63; 95% CI 0.50–0.80; p < 0.001). The difference in bleeding was driven by a significant reduction of bleeding requiring medical attention. There were no differences in the rate of major cardiovascular events (a composite of death from cardiovascular causes, MI, or stroke) between the three treatment strategies. Similarly, the rate of ST did not differ between the three randomization arms. A post hoc analysis looking at the combined efficacy endpoint of all-cause mortality or recurrent hospitalization (with hospitalizations classified as bleeding-related, secondary to a cardiovascular cause or due to other reasons) demonstrated that the two rivaroxaban doses significantly reduced the combined risk of death or rehospitalization when compared with TT with VKA. 49 The difference in the rate of the composite endpoint was driven by a reduction of bleeding and cardiovascular-related hospitalizations while no differences in mortality were seen among the three treatment strategies. However, as in the WOEST and ISAR-TRIPLE trials, the statistical power of PIONEER AF PCI for other endpoints other than bleeding was limited.
RE-DUAL PCI trial
The Randomized Evaluation of Dual Antithrombotic Therapy with Dabigatran versus Triple Therapy with Warfarin in Patients with Nonvalvular Atrial Fibrillation Undergoing Percutaneous Coronary Intervention (RE-DUAL PCI) trials assessed the safety of dabigatran in patients who underwent successful PCI with coronary stenting, using two drug regimens (110 mg and 150 mg twice daily) which in the RE-LY trial demonstrated superior safety versus warfarin, with the 150 mg dose providing additional signals of improved efficacy for stroke and systemic embolism reduction.41,50 RE-DUAL PCI compared two DT regimens (dabigatran 110 mg or 150 mg twice daily plus clopidogrel or ticagrelor) versus TT consisting of aspirin, clopidogrel or ticagrelor, and warfarin. Aspirin in the TT arm was administered for 1 month in patients treated with bare metal stent(s) or 3 months in patients who received DES. Clopidogrel was the P2Y12 inhibitor used in most patients, with only 12% of patients receiving ticagrelor. Outside of the United States, patients older than 80 years (or patients older than 70 years in Japan) were not randomized to the 150 mg dose. The primary endpoint of the study was major or clinically relevant nonmajor bleeding in keeping with the definitions of the International Society on Thrombosis and Hemostasis. The trial had a noninferiority design with respect to the two dabigatran doses versus warfarin (noninferiority was demonstrated if the upper confidence interval of the HR with the two dabigatran doses versus warfarin did not exceed 1.38). In addition, the initial study protocol aimed at demonstrating the noninferiority of dabigatran versus warfarin (using the same noninferiority margin of 1.38 for the HR) for a composite coprimary efficacy endpoint of ischemic events, including MI, stroke, or systemic embolism, death, or unplanned revascularization by PCI or coronary artery bypass grafting. However, the projected number of patients required to demonstrate the noninferiority for the coprimary efficacy endpoint (n = 8520) was deemed to be unrealistic to be reached in a timely fashion. The coprimary efficacy endpoint was, therefore, downgraded into a secondary endpoint.
Among 2725 patients randomized across the three treatment arms, DT with either the two dabigatran doses had significantly lower rates of bleeding when compared with TT (15.4% in the 110 mg DT group versus 26.9% in the TT group, HR 0.52, 95% CI 0.42–0.63, p < 0.001 for both noninferiority and superiority; 20.2% in the 150 mg DT group versus 25.7% in the TT group, HR 0.72, 95% CI 0.58–0.88, p < 0.001 for noninferiority). The rate of the secondary efficacy endpoint was similar among the pooled dabigatran doses and warfarin (13.7% versus 13.4% for DT with both dabigatran doses and warfarin; HR 1.04, 95% CI 0.84–1.29, p = 0.005 for noninferiority). Noninferiority of DT with either dabigatran doses for ischemic events was not met versus TT when repeat revascularization was not counted in the composite endpoint (9.6% for DT versus 8.5% for TT; HR 1.17, 95% CI 0.90–1.53, p = 0.11 for noninferiority). In addition, patients randomized to the 110 mg dabigatran dose had an excess of thromboembolic events or death when compared with TT (11.0% versus 8.5%, HR 1.30, 95% CI 0.98–1.73, p = 0.07). Importantly, the rate of ST with dabigatran 110 mg, albeit not statistically significant, was almost doubled when compared with TT (15 versus 8 ST events, HR 1.86, 95% CI 0.79–4.40, p = 0.15).
The overall results of the trial were consistent in post hoc analyses comparing the safety and efficacy of DT using dabigatran versus TT in the subgroup of patients who were enrolled with an ACS diagnosis at baseline and in patients who were treated with clopidogrel or ticagrelor (p value for interaction >0.10). 51 In addition, although direct comparisons of patients treated with dabigatran plus ticagrelor or clopidogrel were not investigated due to concerns for allocation bias (the choice among different P2Y12 inhibitors was left to the investigator’s discretion), the rate of bleeding was higher with ticagrelor when compared with clopidogrel when used with either dabigatran 110 mg or 150 mg (21.2% versus 14.5% and 23.1% versus 19.7% with ticagrelor and clopidogrel when used with dabigatran 110 mg and dabigatran 150 mg, respectively).
AUGUSTUS trial
The results of the recently published Open-Label, 2 × 2 Factorial, Randomized, Controlled Clinical Trial to Evaluate the Safety of Apixaban vs. Vitamin K Antagonist and Aspirin vs. Aspirin Placebo in Patients with Atrial Fibrillation and Acute Coronary Syndrome and/or Percutaneous Coronary Intervention (AUGUSTUS) trial has further strengthened the understanding of the safety advantages with NOACs use and aspirin removal when the coagulation and platelet activation are simultaneously targeted. 52 A total of 4614 patients were randomized in the study, and 38.8% underwent elective PCI, 37.3% underwent PCI for ACS and 23.9% were ACS patients who were managed medically. A double sequential randomization scheme (2 × 2 factorial design) was employed to allocate patients to different treatment arms. On a common background of P2Y12 therapy (consisting of clopidogrel >90% of the cases), patients were first randomized to receive apixaban (5 mg twice daily or 2.5 mg twice daily according to the labeling indications) or VKA (first randomization factor) and, subsequently, they were randomized again (second randomization factor) to aspirin or matching placebo. With respect to the primary endpoint of the study that was the incidence of major or clinically relevant nonmajor bleeding as defined by the International Society of Thrombosis and Haemostasis, this study design allows for the obtaining unbiased information on the comparative treatment effect of apixaban versus warfarin and on the effect of removing aspirin. The trial had a noninferiority design, followed by superiority testing in the case of demonstrated noninferiority, for the comparison of apixaban and warfarin, and superiority design for the comparison of aspirin versus placebo. Patients were randomized after a mean time interval of 6.6 days following the index diagnosis of ACS or the index PCI procedure. During 6 months of follow-up, apixaban resulted in significantly lower rates of bleeding versus warfarin (10.5% versus 14.7%, HR 0.69, 95% CI 0.58–0.81, p < 0.001 for both noninferiority and superiority). Aspirin versus placebo resulted in significantly higher rates of bleeding (16.1% versus 9.0%, HR 1.89, 95% CI 1.59–2.24, p < 0.001). In addition, the combined endpoint of death and hospitalization was significantly lower with apixaban (driven by significantly lower rates of new hospitalizations) while no differences for this endpoint were seen with aspirin treatment or placebo. The rate of ischemic events did not differ between the randomized treatment arms although the rate of definite or probable ST almost doubled in patients who did not receive aspirin (21 versus 11 events, HR for aspirin versus placebo 0.52, 95% CI 0.25–1.08).
ENTRUST AF-PCI
The results of the edoxaban-based versus vitamin K antagonist-based antithrombotic regimen after successful coronary stenting in patients with atrial fibrillation (ENTRUST AF-PCI) trial have contributed to further expand the body of evidence on NOAC use in AF patients undergoing PCI. 53 ENTRUST AF-PCI included 1506 patients who, following successful PCI, were randomized in a 1:1 ratio to receive a NOAC-based versus a VKA-based antithrombotic treatment strategy. Patients were eligible for randomization after 4 h and up to a maximum of 5 days after the index PCI (median time to the randomization of 45 h). The NOAC-based strategy consisted of edoxaban 60 mg once daily plus clopidogrel 75 mg once daily (default P2Y12 inhibitor) for 12 months. The edoxaban dose was reduced to 30 mg in case of renal impairment with a creatinine clearance of 15–50 ml/min, body weight ⩽60 kg, or use of potent P-glycoprotein inhibitors including cyclosporine, dronedarone, erythromycin, or ketoconazole. The VKA-based strategy consisted of VKA therapy aimed at achieving an international normalized ratio (INR) between 2.0 and 3.0, plus clopidogrel 75 mg once daily and low-dose aspirin for a minimum of 1 month and up to 12 months after the index procedure. The choice of another P2Y12 inhibitor rather than clopidogrel (e.g. ticagrelor or prasugrel) was left to the discretion of the investigators, as well as, the duration of aspirin administration in the VKA-based strategy after the first month. The primary endpoint of the study was the composite of major or clinically relevant nonmajor bleeding according to the International Society of Thrombosis and Haemostasis definitions. The trial had a noninferiority design (20% excess risk for bleeding as noninferiority margin) with subsequent testing for superiority in case of demonstrated noninferiority. At 12 months, the NOAC-based strategy was noninferior to the VKA-based regimen with respect to the primary composite endpoint (bleeding rate of 17% with edoxaban versus 20% with VKA; HR 0.83,95% CI 0.65–1.05). Despite the numerically lower rates of bleeding in the edoxaban group, edoxaban was not superior to the VKA-based regimen. No differences in the rate of ischemic events were seen between the two treatment groups although the wide confidence interval around the risk estimate (HR 1.06, 95% CI 0.71–1.69) precludes drawing definite conclusions on ischemic efficacy. Pharmacodynamic investigations support the importance of using edoxoban at the stroke prevention dose, as in ENTRUST AF-PCI. 54
Potential caveats in the interpretation of newer evidence
Interest in the positive results of the recently published trials of DT has permeated the medical community. Certainly, safety issues and high rates of bleeding with TT before the release of these trials were an important unmet need in the field of cardiovascular pharmacotherapy. However, enthusiasm should not come at the cost of confusing clinical judgment when deciding between different treatment strategies. A critical overview of these studies can be useful to avoid some potential caveats in the interpretation of the newer evidence.
First, none of the current trials can provide robust answers on the comparative efficacy of DT versus TT for ischemic complications. Efficacy was indeed evaluated as a secondary endpoint in all of the trials. This means that, although the indications in these trials were consistent and pointed toward the direction of preserved efficacy with DT, no definitive conclusions can be made at this time regarding the effect of DT versus TT with respect to ischemic outcomes. A meta-analysis of the four RCTs comparing TT versus DT (namely WOEST, ISAR-TRIPLE, RE-DUAL PCI, and PIONEER AF) attempted to overcome the limited statistical power of each individual study for ischemic outcomes. 55 The results of this pooled analysis did not show differences in the trial-defined major adverse cardiac events between DT and TT (10.4% versus 10.0%, HR 0.85, 95% CI 0.48–1.29, I2 = 58.4%), other individual ischemic outcomes, including ST and MI, did not differ between the two strategies. However, the conclusions of this meta-analysis are hampered by differences in the design, drug regimens, and patient’s characteristics compared between the included studies, which eventually resulted in significant degrees of statistical heterogeneity in the pooled analysis. A study-level network meta-analysis encompassing four trials (i.e. WOEST, PIONEER AF-PCI, RE-DUAL PCI, and AUGUSTUS) confirmed the incremental safety, without concerns over an increased ischemic risk, with a NOAC plus a P2Y12 inhibitor antithrombotic strategy when compared with TT. 56 An updated meta-analysis restricted to the four NOAC trials (PIONEER AF-PCI, RE-DUAL PCI, AUGUSTUS, ENTRUST AF-PCI) corroborated the incremental safety of DT consisting of a NOAC plus a P2Y12 inhibitor versus TT, but it showed a numerical excess of ST events which narrowly missed the threshold for statistical significance (p = 0.06).53,57
The timing of aspirin removal is another important aspect that should be carefully evaluated. In all of the recent trials investigating NOAC safety, patients were not immediately randomized to an aspirin-free strategy following the diagnosis of ACS or the index PCI procedure. A time delay of a maximum 3 days after PCI was allowed before randomization in PIONEER AF, while a time delay of up to 5 days was allowed in the RE-DUAL PCI and ENTRUST AF-PCI trials, in AUGUSTUS, the mean time interval elapsed from the diagnosis of ACS or the index PCI procedure to randomization was 6 days. This means that the information on the safety of aspirin removal in these trials is weaker in the time window of higher risk for ST (i.e. immediate and early postprocedural phase). These limitations are even more important because of the almost doubled ST rate seen in AUGUSTUS in patients randomized to placebo instead of aspirin.
These observations suggest that, although a strategy of DT may be considered in many patients based on the trial results, a one-size-fits-all approach cannot apply to all patients when deciding among different treatment strategies in daily clinical practice. The evaluation of the specific factors predisposing to bleeding and ischemic complications, on an individual case-by-case basis, should be used instead for guiding the selection of the most appropriate pharmacological treatment strategy. Unfortunately, to date, there are no supporting tools (i.e. combined risk scores) for the identification of the optimal balance between ischemia and bleeding risks in this complex clinical scenario. A series of risk scores aimed at estimating the risk of stroke and bleeding in AF patients,58–61 in addition to clinical scores to predict bleeding62,63 or balancing bleeding and ischemic risk in patients receiving antiplatelet therapy,64,65 have been developed, but neither these scores, nor their combination, has been prospectively tested for guiding the therapeutic management of patients requiring combined treatment with antiplatelet and OACs. Therefore, rigorous clinical judgment, moving its initial steps from the identification and proper contextualization of the individual factors predisposing to higher bleeding or ischemic risk, should be used for customizing different pharmacological treatment strategies aimed at balancing efficacy and safety. 66
Current recommendations for clinical practice
Waiting for the acceptance of the recent evidence generated on NOACs use and antiplatelet therapy in anticoagulated patients undergoing PCI, two consensus documents by European and North American experts have been recently released for guiding clinicians among the selection of different therapeutic options and treatment strategies.67,68 The suggested recommendations are summarized in Table 2 and graphically displayed in Figure 3. On both sides of the Atlantic, preference is given to NOAC therapy, either in the context of TT or DT, owing to improved safety compared with warfarin. Other bleeding avoidance strategies, including radial access during PCI and the administration of proton pump inhibitors, are recommended. Clopidogrel, as part of a DT strategy, is the preferred antiplatelet agent while ticagrelor (or prasugrel only in Europe) should be considered in patients at high ischemic risk only under special circumstances. Differences between the two consensus documents mainly concern the duration of TT. North American experts suggest DT as a default approach at the time of hospital discharge, with TT administration limited only to the periprocedural phase. In contrast, European recommendations point toward prolongation of TT for up to 1 month with the possibility to prolong TT for up to 6 months in patients at high thrombotic risk, while the use of DT immediately after PCI should be reserved for patients at very high bleeding risk.
Updated international expert consensus documents for managing anticoagulation and antiplatelet therapy in daily clinical practice.

ACS, acute coronary syndrome; CAD, coronary artery disease; DT, dual therapy; NOAC, nonvitamin K oral anticoagulant; OAC, oral anticoagulation; PCI, percutaneous coronary intervention; TT, triple therapy; VKA, vitamin K antagonist.

International consensus documents for the management of antithrombotic therapy in daily clinical practice.
Future areas of research
The lack of evidence on the efficacy of DT consisting of NOACs plus single P2Y12 platelet inhibition (i.e. trials with ischemic outcomes as primary endpoints) represents the largest gap in current knowledge which deserves future specific investigation. Running these type of trials is complicated owing to the larger sample size required to reach adequate statistical power. Continuous improvements in the efficacy profile of newer generation DES, leading to the current standards of performance characterized by low rates of ST incidence and stent failure, represent a challenge from a trialist’s perspective for the design of such a trial. Potentially, the infrastructure of national registries could be used for running trials (e.g. registry-based randomized trial) requiring the inclusion of large cohorts of patients. 69
The optimal combination of NOACs and P2Y12 inhibitor is another important area for future research. A post hoc analysis from the RE-DUAL-PCI trial highlighted similar risk reduction of the primary endpoint of the study, major or clinically relevant nonmajor bleeding event when either clopidogrel or ticagrelor were used in combination with dabigatran doses (p value for interaction >0.10). 51 Different dosing strategies or combinations of NOACs and P2Y12 inhibitors might allow for a more nuanced modulation of the anticoagulation intensity and potency of the antiplatelet effect that can be achieved. Different combinations could be used to better match the patient-specific risk profiles for ischemia and bleeding. The availability of reversal agents for dabigatran, rivaroxaban, apixaban, and, recently, for ticagrelor should be also considered in the threshold risk evaluations favoring the selection of more potent or safer antithrombotic agents.70–72 Rapid reversal of anticoagulation/antiplatelet effects could indeed prompt the use of more-potent antithrombotic strategies in patients who have high ischemic and bleeding risk features. Although the use of platelet function and genetic testing cannot be routinely recommended to assist with the selection of P2Y12 inhibitors, the selective use of these tests in patients with AF undergoing PCI is reasonable. 73 As recently demonstrated in patients undergoing primary PCI, the use of genetic testing for selecting patients who may safely receive clopidogrel (i.e. screening for mutations that may limit the bioactivation of clopidogrel and blunt its antiplatelet effect) might further support the selection of different P2Y12 inhibitors in this clinical scenario. 74 Indeed, identifying antiplatelet therapies with safer profiles (e.g. less gastrointestinal bleeding) while preserving efficacy represents another area of ongoing research. 75
Risk stratification in patients requiring combined antithrombotic treatment strategies is an area that, unfortunately, has been poorly investigated. A thorough identification of the baseline clinical characteristics associated with treatment- and combination-specific determinants of bleeding/ischemic risk would be important for tailoring the selection of the optimal antithrombotic treatment strategies. In addition, results from available RCTs on the characteristics and risk profiles of patients who bled and those who had MI/ST would be of added value.
Finally, the long-term management of OAC treatment in AF patients after PCI deserves more attention. A nationwide, registry-based study comparing different antithrombotic strategies in the chronic phases after an ACS (>1 year) reported an increased risk of bleeding, without additional ischemic protection, with combined VKA and antiplatelet therapy (aspirin or clopidogrel) versus VKA alone. 76 These results represent the evidence basis informing current guidelines and consensus documents on the chronic antithrombotic management of AF patients after PCI.20,67–68,77 The optimizing antithrombotic care in patients with atrial fibrillation and coronary stent (OAC ALONE) study tested the noninferiority of an OAC alone strategy (75% consisting of warfarin) versus OAC plus a single antiplatelet agent for the composite endpoint of all-cause death, MI, stroke, or systemic embolism in patients with stable CAD beyond 1 year after PCI. 78 The study, although being inconclusive due to slow enrollment leading to premature termination, did not establish the noninferiority of OAC therapy alone versus OAC plus a single antiplatelet agent (rate of the primary endpoint of 15.7% and 13.6% in the OAC alone the combined OAC and antiplatelet group, respectively; HR, 1.16, 95% CI 0.79–1.72; p = 0.20 for noninferiority). The recent results of the Atrial Fibrillation and Ischemic Events with Rivaroxaban in Patients With Stable Coronary Artery Disease Study (AFIRE) have contributed to better inform the long-term antithrombotic management strategies in AF patients after PCI. The trial included 2236 patients with stable coronary disease from 294 centers in Japan who, 1 year after coronary revascularization by coronary artery bypass grafting or PCI, were randomized to rivaroxaban therapy alone (rivaroxaban dose of 15 mg daily, 10 mg daily for creatine clearance 15–49 ml/min) versus rivaroxaban plus an antiplatelet agent (aspirin, clopidogrel, or prasugrel). The study was terminated early because of increased mortality in the group of patients who received combined treatment with NOAC and antiplatelets. 79 In addition, NOAC monotherapy was noninferior to the combined treatment strategy for ischemic efficacy. Although these results provide more robust evidence on the safety and efficacy of NOAC monotherapy in the long-term management of AF patients after PCI, 77 lower doses of rivaroxaban used in the study when compared with the recommended dosing regimen in Western countries, and differences in the baseline risk of bleeding among Asian and Western patients, limit the generalizability of these results and warrants additional investigation on this topic.
Conclusion
The pharmacological management of patients requiring combined treatment with OAC and antiplatelet treatment is complex and challenging in daily clinical practice. Although the enhanced safety of DT, consisting of NOACs and single antiplatelet therapy, has been consistently demonstrated, data on the efficacy profile of these newer therapeutic strategies are weaker and require future investigation. Based on the recently accumulated results from RCTs, it is advisable to minimize the exposure to TT and consider a faster transition to DT in patients who are at low ischemic and high bleeding risk. In this complex clinical scenario, the selection of treatment strategies should always be based on an individualized patient-centered approach aiming at pinpointing the optimal balance between the risk of bleeding and ischemia.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
Dominick J. Angiolillo declares that he has received consulting fees or honoraria from Amgen, Aralez, AstraZeneca, Bayer, Biosensors, Boehringer Ingelheim, Bristol-Myers Squibb, Chiesi, Daiichi Sankyo, Eli Lilly, Haemonetics, Janssen, Merck, PhaseBio, PLx Pharma, Pfizer, Sanofi, and The Medicines Company and has received payments for participation in review activities from CeloNova and St Jude Medical. Dominick J. Angiolillo also declares that his institution has received research grants from Amgen, AstraZeneca, Bayer, Biosensors, CeloNova, CSL Behring, Daiichi Sankyo, Eisai, Eli Lilly, Gilead, Idorsia, Janssen, Matsutani Chemical Industry Co., Merck, Novartis, Osprey Medical, and Renal Guard Solutions; in addition, Dominick J. Angiolillo is recipient of a funding from the Scott R. MacKenzie Foundation and the NIH/NCATS Clinical and Translational Science Award to the University of Florida UL1 TR000064 and NIH/NHGRI U01 HG007269, outside the submitted work. DC discloses the following relationships: speakers’ honoraria from Bayer, AstraZeneca, Daiichi Sankyo, Pfizer, Boehringer Ingelheim, and consulting fees from Abbott Vascular, Bayer, and Daiichi Sankyo.
Sergio Buccheri has no conflict of interest to disclose.