
Abstract
Background:
There is still much controversy about whether meteorological conditions influence the occurrence of acute aortic dissection (AAD). The aim of the present study was to investigate the possible correlation between atmospheric pressure, temperature, lunar cycle and the event of aortic dissection in our patient population.
Methods:
The clinical data for 348 patients with AAD (73% type Stanford A) were confronted with the meteorological data provided by the Cologne weather station over the same period.
Results:
There were no statistically significant differences between meteorological parameters on days of AAD events compared with control days. A logistic regression model showed that air pressure (odds ratio [OR] 1.004, 95% confidence interval [CI] 0.991–1.017, p = 0.542), air temperature (OR 0.978, 95% CI 0.949–1.008, p = 0.145), season (p = 0.918) and month of the event (p = 0.175) as well as presence of full moon (OR 1.579, 95% CI 0.763–3.270, p = 0.219) were not able to predict AAD events. Also, no predictive power of meteorological data and season was found on analysing their impact on different types of AAD events.
Conclusions:
Our study did not reveal any dependence of atmospheric pressure, air temperature or the presence of full moon on the incidence of different types of AAD.
Introduction
Acute aortic dissection (AAD) is a medical emergency and should be treated as soon as possible. The International Registry of Acute Aortic Dissection reported in 2015 a total mortality of 24.4% in type Stanford A dissection and 10.7% in Stanford B type dissection. 1 Some studies reported a relationship between meteorological factors and AAD.2–6 Nevertheless, the results of the studies are different and one study did not find any relationship between weather conditions and AAD. 7 The aim of the present study was to investigate the possible correlation between atmospheric pressure, temperature, lunar cycle and the event of AAD.
Materials and methods
The study design was a retrospective review of prospectively collected data. The Institutional Review Board of Cologne University approved this study and waived the need for individual patient consent. Cologne, located in Germany, has its highest point at 118 m above sea level and lowest point at 37.5 m above sea level. The required meteorological information was extracted from the Cologne weather station. All consecutive patients admitted to our institution with the diagnosis of AAD Stanford A and Stanford B during the time period from January 2006 to July 2015 were included and analysed with regard to chronobiological variations in the timing of occurrence of aortic dissections. Surgery for AAD was indicated according to the preoperatively performed computed tomography. An intra-operative transoesophageal echocardiography was performed in all patients. Meteorological data, such as air pressure and air temperature, seasonal differences as well as the presence of full moon, were documented for each day within the study period and evaluated for potential predictive power of clinical events of interest. A total of 3499 days were analysed in terms of association of meteorological and seasonal factors with the incidence of AAD. Together with the analysis of AAD in general, subgroup analyses of Stanford A and Stanford B AAD was performed in order to evaluate the potential influence of factors of interest on various types of dissections.
Statistical analysis
All data were analysed using IBM SPSS Statistics for Windows, Version 21 (Released 2012. IBM Corp., Armonk, NY, USA) and are presented as continuous or categorical variables. Continuous data were evaluated for normality using one sample Kolmogorov–Smirnov test and confirmed by histograms. Continuous variables were expressed as the mean ± standard deviation in cases of normally distributed variables or median (interquartile range) in cases of non-normally distributed variables. Categorical variables are presented as total numbers and percentages. Continuous data potentially associated with clinical events of interest were analysed using the unpaired Student’s t test for normally distributed variables and Mann–Whitney U test for non-normally distributed variables. Pearson’s chi-square test or Fisher exact test were used for categorical data dependent on the minimum expected count in each cross tab. A binary logistic regression model was applied for the analysis of potential predictors of clinical events of interest. p values < 0.05 were considered statistically significant.
Results
A total of 348 patients diagnosed with an AAD were admitted during the time period from January 2006 to July 2015 to our institution. Of them, 255 had Stanford A AAD, whereas 87 were diagnosed with Stanford B AAD. Table 1 shows the seasonal and monthly distribution of AAD events.
Seasonal and monthly distribution of acute aortic dissection.
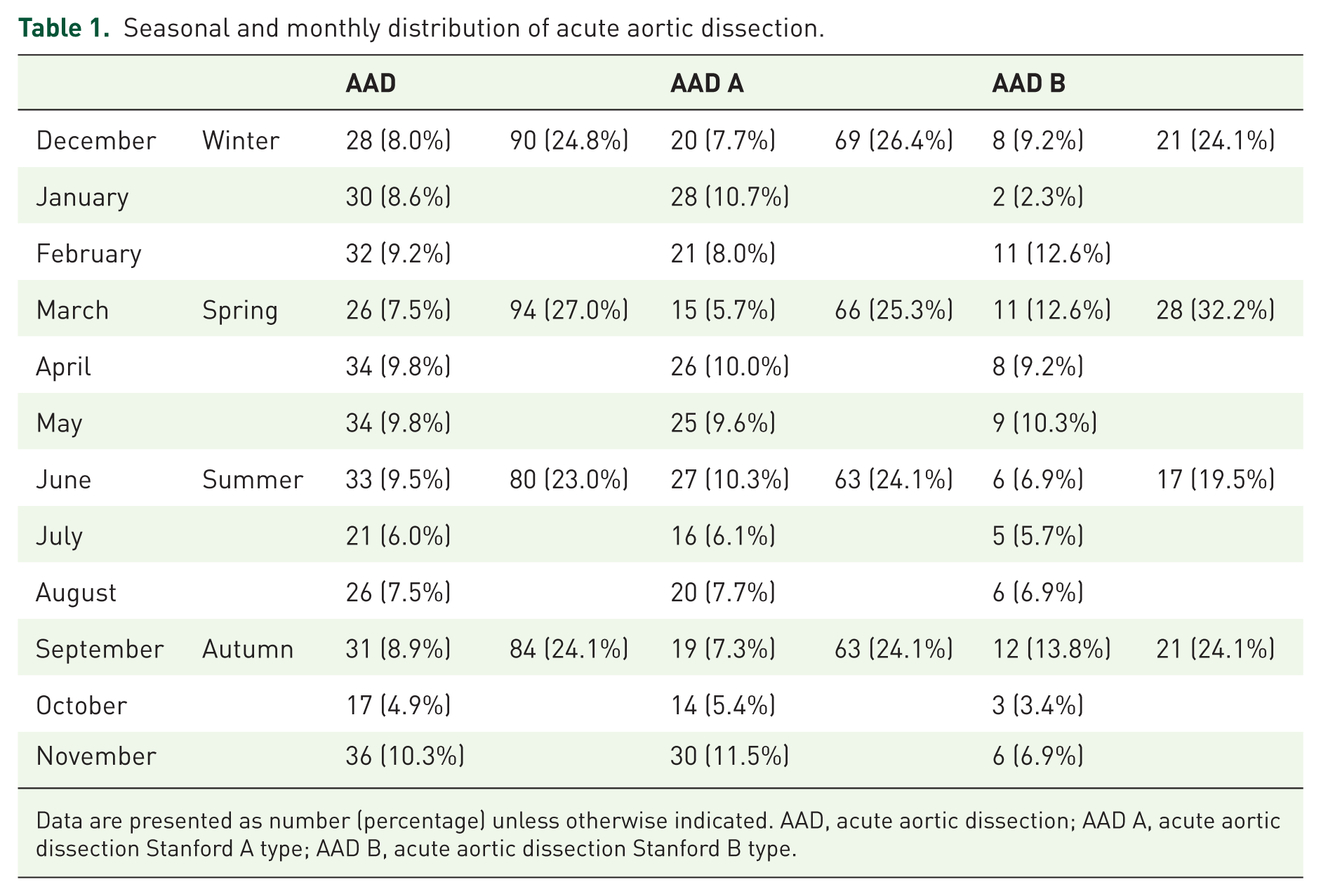
Data are presented as number (percentage) unless otherwise indicated. AAD, acute aortic dissection; AAD A, acute aortic dissection Stanford A type; AAD B, acute aortic dissection Stanford B type.
In the univariate analysis, there were no statistically significant differences between meteorological parameters on days of AAD events compared with control days. Air temperature (10.20 ± 6.67°C versus 10.80 ± 6.89°C, p = 0.124) and air pressure (1004.28 ± 8.27 mmHg versus 1003.95 ± 8.86 mmHg, p = 0.512) were equally distributed between days of AAD events and control days. Also, there were no statistically significant differences in terms of the distribution of months (p = 0.171) and seasons (p = 0.753) between days on which an AAD occurred and control days. The presence of full moon also did not influence the incidence of AAD while full moon was present on 2.3% (n = 8) versus 3.5% (n = 111) of event versus control days (p = 0.232). A logistic regression model showed that air pressure (odds ratio [OR] 1.004, 95% confidence interval [CI] 0.991–1.017, p = 0.542), air temperature (OR 0.978, 95% CI 0.949–1.008, p = 0.145), season (p = 0.918) and month of the event (p = 0.175) as well as presence of full moon (OR 1.579, 95% CI 0.763–3.270, p = 0.219) were not able to predict AAD events (see Table 2).
Logistic regression model of potential predictors associated with the incidence of acute aortic dissection.

Figures 1 and 2 demonstrate the seasonal and monthly event of ADD and mean atmospheric pressure during the study period.
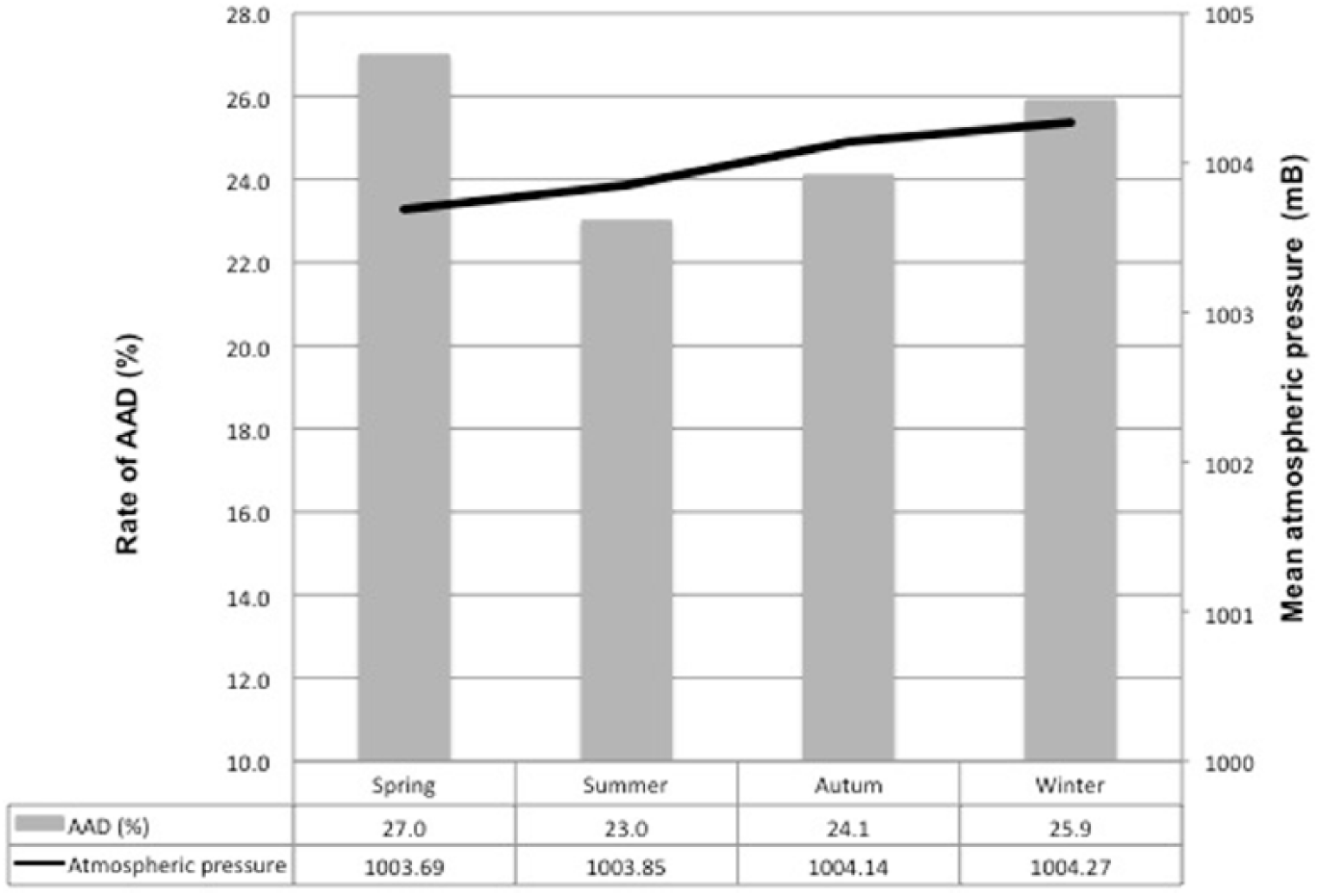
Mean seasonal atmospheric pressure and acute aortic dissection.

Mean monthly atmospheric pressure and acute aortic dissection.
Also, no predictive power of meteorological data and season was found when analysing their impact on different types of AAD events.
An analysis of the subgroup of Stanford A dissection also did not reveal any dependence on meteorological factors and seasonal changes. In the univariate analysis, there were no statistically significant differences between meteorological parameters on days of Stanford A AAD events compared with control days. Air temperature (10.26 ± 6.70°C versus 10.77 ± 6.88°C, p = 0.248) and air pressure (1004.47 ± 8.02 mmHg versus 1003.95 ± 8.86 mmHg, p = 0.354) were similarly distributed between days of Stanford A AAD events and control days. Also, there were no statistically significant differences in terms of the distribution of months (p = 0.135) and seasons (p = 0.891) between days on which Stanford A AAD occurred and control days. The presence of full moon did not influence the incidence of AAD while full moon was present on 1.9% (n = 5) versus 3.5% (n = 114) of event versus control days (p = 0.169). A logistic regression model showed that air pressure (OR 1.007, 95% CI 0.993–1.022, p = 0.329), air temperature (OR 0.985, 95% CI 0.953–1.020, p = 0.398), season (p = 0.956) and month of the event (p = 0.160) as well as full moon (OR 1.895, 95% CI 0.766–4.690, p = 0.167) were not able to predict Stanford A AAD events.
An analysis of the subgroup of Stanford B AAD showed that this event could also not be predicted by or was associated with meteorological factors, season or month of event occurrence. In the univariate analysis, there were no statistically significant differences between meteorological parameters on days of Stanford B AAD events compared with control days. Air temperature (10.00 ± 6.60°C versus 10.75 ± 6.87°C, p = 0.312) and air pressure (1003.70 ± 9.00 mmHg versus 1003.91 ± 8.80 mmHg, p = 0.761) were equally distributed between days of Stanford B AAD events and control days. Also, there were no statistically significant differences in terms of the distribution of months (p = 0.121) and seasons (p = 0.489) between days on which AAD occurred and control days. The presence of full moon did not influence the incidence of AAD while full moon was present on 3.4% (n = 3) versus 3.4% (n = 116) of event versus control days (p = 1.000). A logistic regression model showed that air pressure (OR 0.995, 95% CI 0.971–1.018, p = 0.654), air temperature (OR 0.960, 95% CI 0.907–1.018, p = 0.170), season (p = 0.577) and month of the event (p = 0.190) as well as full moon (OR 1.016, 95% CI 0.315–3.275, p = 0.979) were not able to predict Stanford B AAD events.
Discussion
The influence of weather on AAD has been occasionally postulated in the past; is this assertion a reality or just a myth? The relationship between atmospheric pressure and rupture of abdominal aortic aneurysm has been investigated and some authors have confirmed this thesis.8 –10 We can find only a few articles on the influence of weather on AAD. However, the few articles show conflicting results with regard to AAD and meteorological parameters.1,6,7,11,12
Krdzalic and colleagues 2 and Rabus and colleagues 3 postulated the link between atmospheric pressure and AAD with statistical significance, but their final results are not congruent. Krdzalic and colleagues reported that atmospheric changes (increasing or decreasing) have an influence on the incidence of AAD, but Rabus and colleagues found a high positive correlation between AAD and increasing atmospheric pressure. On the other hand, Verberkmoes and colleagues 4 did not find any correlation between atmospheric pressure and AAD, but they reported a correlation between cold weather and the incidence of AAD. Also Benouaich and colleagues 5 demonstrated a correlation between type A dissection and low atmospheric temperature and Law and colleagues 6 reported that high atmospheric pressure and the absence of thunderstorm warning were associated with increasing AAD in univariant analysis, but the multiple regressions analysis showed that the lower the temperature, the higher the incidence of AAD. We can see that there are different results with respect to this topic.
In the present study, we did not find any statistically significant correlation between atmospheric pressure, ambient temperature, presence of full moon and the frequency of AAD. This result is also congruent with the study of Repanos and Chadha 7 However, the association between AAD and both air temperature and full moon tended to significant, but due to the small number of events does not reach statistical significance or statistical trend.
The different study methods and different geographical zone make a comparison of reported results very difficult.
However, data on the correlation between atmospheric pressure and rate of AAD remain controversial. Currently the mechanism of how atmospheric pressure would influence the rate of dissection remains unclear. One possible mechanism explaining the interaction between meteorological conditions and AAD is that changes in atmospheric pressure and temperature might contribute to sudden changes in blood pressure, which is a known risk factor for AAD. 7 Furthermore, a rise in diastolic blood pressure secondary to exposure to cold has been reported as a physiological response caused by sympathetic reactivity.6,13 Benouaich and colleagues suggested an interaction between high blood pressure, adverse cardiovascular events and cold atmospheric pressure because of an adrenergic-mediated increase of blood pressure due to cold. 5
Also, all the mentioned studies including the present study, are retrospective and therefore the exact time of the event and the exact weather information at that moment remained unknown.
There are several limitations in our study that need to be considered. Firstly, this study is retrospective and this makes it difficult to determine the exact time of the event. Thus, the temperature and air pressure can not be accurately determined. Secondly, we included only the patients who were admitted to our institution. In addition, this study presents a small sample size, as AAD is a rare event. A prospective multicentre study is necessary to capture more patients and the exact moment of the event as well as the exact weather changes.
Conclusion
In conclusion, we could not reveal any dependence of atmospheric pressure, air temperature or the presence of full moon on the incidence of different types of AAD. However, the association between AAD and both air temperature and full moon tended to significant, but did not reach statistical significance due to the small number of events.