
Abstract
Background:
Coronary artery disease (CAD) is one of the leading causes of mortality and morbidity worldwide. We thereby sought to investigate whether the biomarkers, angiopoietin-like 4 (ANGPTL-4) and galectin-3, reflect the severity of CAD.
Methods:
Patients were screened based on inclusion/exclusion criteria and written informed consent was obtained from the patients. Serum ANGPTL-4 and galectin-3 was quantified using enzyme-linked immunosorbent assay (ELISA) and correlated with the Global Registry of Acute Coronary Events (GRACE) and GENSINI score using Spearman’s rank correlation coefficient and multivariate analysis.
Results:
A total of 226 patients consisting of ST-segment elevation myocardial infarction (STEMI), non-STEMI/unstable angina (USA), chronic stable angina (CSA) and normal controls (NCs) participated in the study. ANGPTL-4 and galectin-3 were significantly higher in CAD than the NC group. ANGPTL-4 showed significant negative correlation with GRACE score in acute coronary syndrome (ACS) (r = −0.211, p = 0.03) patients. ANGPTL-4 showed significant positive correlation with serum creatinine (r = 0.304, p = 0.056) and body mass index (BMI) (r = 0.424, p = 0.009) in CSA patients. A modest positive correlation was observed between the serum galectin-3 levels and GRACE score (r = 0.187, p = 0.055) in ACS patients. However, on multivariate analysis the positive correlation relationship between ANGPTL-4 and galectin-3 with the severity of CAD was not sustained.
Conclusion:
In conclusion, ANGPTL-4 and galectin-3 do not appear to have a promising role for assessing the severity of CAD. Nevertheless these biomarkers do warrant further exploration in improving the management of CAD.
Introduction
Despite the significant improvement and development in the diagnosis and treatment, coronary artery disease (CAD) is one of the leading causes of mortality and morbidity worldwide. According to the report by the World Health Organization in 2012 about 7.4 million (31%) deaths occurred worldwide due to coronary heart disease (CHD). 1 In a recent systematic review done on 288 observational studies conducted in the Indian population, it was observed that the prevalence of CAD in urban and rural areas was 2.5–12.6% and 1.4–4.6% respectively. 2 The overall prevalence rate of CAD in Chennai, South India was about 11% while the age standardized prevalence was 9.0%. 3 Many traditional scoring systems like the Global Registry of Acute Coronary Events (GRACE) risk score, SYNTAX score and thrombolysis in myocardial infarction (TIMI) risk score have been used to measure the severity of CAD. However, these scoring systems have not been incorporated into routine clinical practice.4–6 Several cardiac markers like creatine kinase-MB (CK-MB) and cardiac troponins are being utilized in daily clinical practice for the early diagnosis and risk stratification in CAD patients. Circulatory biomarkers such as angiopoietin-like 4 (ANGPLT-4) and galectin-3 are newly emerging biomarkers for CAD. ANGPTL-4 is a multifunctional protein that is involved in lipid regulation, energy metabolism, angiogenesis and inflammation.7–9 Galectin-3 is a β-galactoside-binding lectin expressed by activated macrophages that regulates inflammation, ventricular remodeling and fibrosis.10–12 However, it is still not known if these biomarkers could be used to assess the severity of CAD in the clinical setting. The present study aimed to evaluate the concentration of ANGPTL-4 and galectin-3 levels in patients with CAD and determine the relation of galectin-3 and ANGPTL-4 with the severity of CAD. Since there are insufficient data to establish a link between ANGPTL-4 and CAD, we also attempted to assess the relationship between ANGPTL-4, and other routine clinical and demographic variables. The value of these biomarkers in predicting the need for angioplasty was also evaluated.
Methods
Study population
This was a cross-sectional study performed in the Department of Cardiology and Clinical Pharmacology of SRM Medical College Hospital and Research Centre, India, between January and August 2016. Patients who were diagnosed with ST-segment elevation myocardial infarction (STEMI), non-ST-segment myocardial infarction (NSTEMI)/unstable angina (UA) and chronic stable angina (CSA) were considered eligible for inclusion into the study as case patients. STEMI was defined as a clinical syndrome, with the presence of clinical symptoms of myocardial ischemia, with constant ST elevation and successive release of biomarkers associated with myocardial necrosis. 13 NSTEMI/UA is defined as a clinical syndrome with the absence of persistent ST elevation and presence of cardiac biomarkers of myocardial necrosis. 14 Angina is defined as a clinical syndrome with discomfort in the chest, jaw, shoulder, back, or arm. It is a substernal chest discomfort enraged by exertion or emotional stress and relieved by rest or nitroglycerin. 15 Coronary angiography (CAG) was performed on these patients to determine the presence of blockage in the coronary vessels. Patients who showed no evidence of CAD or CAD equivalents with respect to their symptoms with normal echocardiography (ECG) were considered eligible for inclusion as normal controls (NCs). We excluded patients with other inflammatory diseases such as infections, cancer, heart failure (HF) and autoimmune diseases.
Clinical collection of data
Clinical and demographic data were collected on patient age, sex, waist and hip circumference and other cardiovascular risk factors such as diabetes mellitus, hypertension, current/previous smoker, dyslipidemia, renal disease, family history of cardiac disease and sedentary lifestyle. Vital signs including blood pressure, heart rate and body mass index (BMI) were obtained. A 12-lead ECG, including assessment of left ventricular ejection fraction (LVEF) (%) and regional wall motion abnormality (RWMA) was done. GENSINI score was calculated using coronary angiographic scoring systems and GRACE score was calculated to predict the risk of death in myocardial infarction (MI) patients. Blood sampling was done to determine the level of hemoglobin (Hb), serum creatinine (SCr), glucose and cardiac enzymes (troponin-T, CK-MB).
Ethical approval
The study was approved by the SRM Medical College Institutional Ethics Committee (IEC), India (664/IEC/2014) and all study procedures were performed in accordance with the provisions of the Declaration of Helsinki.
Laboratory analysis
After obtaining the written informed consent from all patients, 4 ml of blood sample was collected from the vein in the forearm prior to CAG. After adequate centrifugation at 2500 rpm for 10 min, the serum samples were extracted and were stored in −80°C deep freezer. The serum which was centrifuged from the blood sample was subjected to enzyme-linked immunosorbent assay (ELISA) for measurement of biomarkers galectin-3 and ANGPTL-4 with a commercially available (Ray Biotech Human ANGPTL-4 and galectin-3 ELISA, GA, USA) kit. The inter-assay coefficient of variation was 7.6% and 8.8% for galectin-3 and ANGPTL-4 respectively. The measurements of ANGPTL-4 and galectin-3 were done in a blinded fashion as the investigators who performed the ELISA analysis were not informed about the patient’s diagnosis.
Statistical analysis
Continuous variables were summarized as mean ± standard deviation and categorical data were expressed as frequency and percentages. Differences in categorical variables between groups were evaluated with the Chi-square test and differences in continuous variables between groups were analyzed with one-way analysis of variance test. We assessed the correlation between ANGPTL-4, galectin-3 and clinical and biochemical parameters using the Spearman’s rank correlation coefficient. The optimal cutoff level of ANGPTL-4 and galectin-3 to predict the need for coronary angioplasty in CAD patients was evaluated using the area under the receiver operating characteristic (ROC) curve. We performed a multivariate linear regression using galectin-3/ANGPTL-4 as dependent variables and other parameters such as BMI, GRACE, GENSINI score, age, total count and blood glucose as independent variables. All statistical analyses were performed with SPSS software version 16.0 (SPSS Inc., Chicago, IL, USA). All p-values were two-sided with a value of <0.05 considered significant.
Results
The baseline characteristics of the study patients are shown in Table 1. Patients were divided into four groups namely STEMI (n = 57), NSTEMI/UA (n = 63), CSA (n = 42) and NC (n = 64) (Supplementary Figure 1). As expected, there was a significant reduction in age in NC versus other groups. Patients with STEMI and NSTEMI/UA had a significant increase in GENSINI score compared with CSA. Significant correlations were observed between the galectin-3 and age, urea, total leukocyte count, GRACE score, GENSINI score and ANGPTL-4 (Table 2). Significant correlations were also seen between ANGPTL-4 and age, serum creatinine, packed cell volume and waist to hip ratio (Table 3).
Baseline characteristics including demographics, risk factors and laboratory findings of study participants.

BMI, body mass index; CSA, chronic stable angina; CVD, cardiovascular disease; DVD, double vessel disease; F/h/o, family history of; GRACE, Global Registry of Acute Coronary Events; LVEF, left ventricular ejection fraction; NC, normal controls; NSTEMI, non-ST-segment elevation myocardial infarction; RWMA, regional wall motion abnormalities; STEMI, ST-segment elevation myocardial infarction; SVD, single vessel disease; TVD, triple vessel disease; WHR, waist–hip ratio.
Correlation between galectin-3, and clinical/demographic variables in CAD patients.

ANGPTL-4, angiopoietin-like 4; CAD, coronary artery disease; GRACE, Global Registry of Acute Coronary Events; TLC, total leukocyte count.
Correlation between ANGPTL-4, and clinical/demographic variables in CAD patients.

ANGPTL-4, angiopoietin-like 4; CAD, coronary artery disease; pcv, packed cell volume; WHR, waist-hip ratio.
The serum ANGPTL-4 and galectin-3 concentrations were significantly higher among patients with STEMI, NSTEMI/UA and CSA than the NC group (p = 0.0001). There was also a significant difference in the galectin-3 concentrations between STEMI and NSTEMI/UA (p = 0.04; Figure 1). Based on correlation analysis, significant negative correlations were observed between serum ANGPTL-4 levels and GRACE risk score in ACS (r = −0.211, p = 0.030; Figure 2(a)) and STEMI patients (r = −0.324, p = 0.022; Figure 2(b)). The serum ANGPTL-4 levels also showed positive correlation with serum creatinine (r = 0.304, p = 0.056; Figure 3(a)) and BMI (r = 0.424, p = 0.009; Figure 3(b)) in CSA patients. In addition, a modest positive correlation was determined between the serum galectin-3 levels and GRACE risk score (r = 0.187, p = 0.055) in ACS patients (Figure 4). In contrast, no significant association was observed between GENSINI score and serum ANGPTL-4 (r = 0.100, p = 0.287) and galectin-3 (r = 0.144, p = 0.126).

(a) Mean concentration of ANGPTL-4, ng/ml among the study groups. (b) Mean concentration of galectin-3, ng/ml among the study groups.
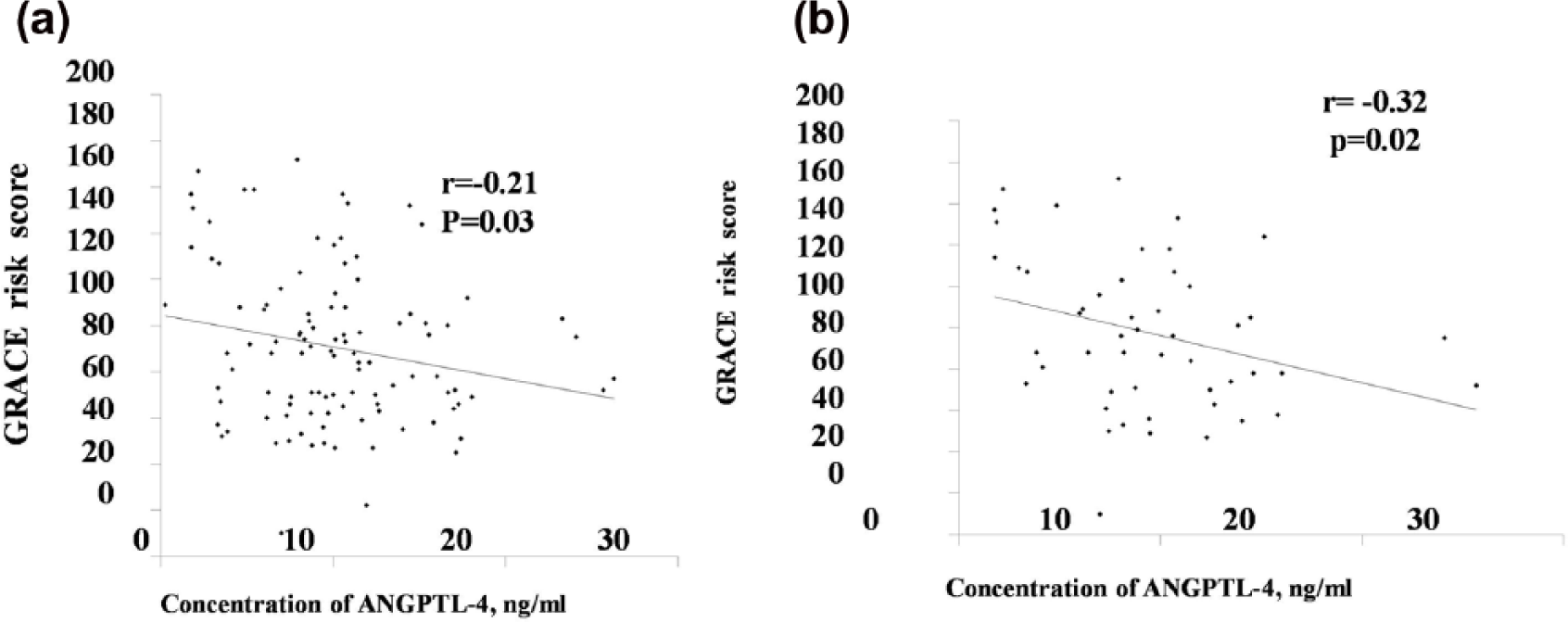
(a) ANGPTL-4 versus GRACE risk score in ACS patients. (b) ANGPTL-4 versus GRACE Risk Score in STEMI patients.

(a) ANGPTL-4 versus serum creatinine in CSA patients. (b) ANGPTL-4 versus BMI in CSA patients.

Galectin-3 versus GRACE risk score in ACS patients.
The mean concentration of galectin-3 and ANGPTL-4 was comparatively higher among patients (age > 40 years) STEMI, NSTEMI/UA and CSA than in the NC group. There was also a significant difference in galectin-3 concentration between the groups NC and CSA (p = 0.017), NC and STEMI (p = 0.0001), NSTEMI and STEMI (p = 0.018). We also looked at the mean concentration of galectin-3 and ANGPTL-4 among males and females separately. The mean concentration of galectin-3 and ANGPTL-4 was comparatively lower in the control group when compared with STEMI, NSTEMI/UA and CSA group among both males and females. A significant difference was also observed in the concentration of galectin-3 between the groups NC and CSA (p = 0.006), NC and STEMI (p = 0.0001), NSTEMI and STEMI (p = 0.015) and NC and STEMI (p = 0.0001).
We performed a multivariate linear regression using galectin-3/ANGPTL-4 as dependent variables and other parameters such as BMI, GRACE, GENSINI score, age, total count, blood glucose as independent variables. We observed that in the presence of these variables, the relationship between the biomarkers and the variables that showed a correlation on univariate correlation was obfuscated.
The combined ROC curve was plotted to predict the ability of ANGPTL-4 and galectin-3 in assessing the need for coronary angioplasty in CAD patients. The ability of galectin-3 to differentiate whether a person required angioplasty or medical management was marginal [AUC = 0.585; p = 0.04; 95% confidence interval (CI) 0.498–0.672] (Figure 5) Adjustment of age and sex was done to predict the ability of ANGPTL-4 and galectin-3 in assessing the need for coronary angioplasty in MI patients. However, it was found that galectin-3 and ANGPTL-4 could not predict whether a person required angioplasty or medical management.
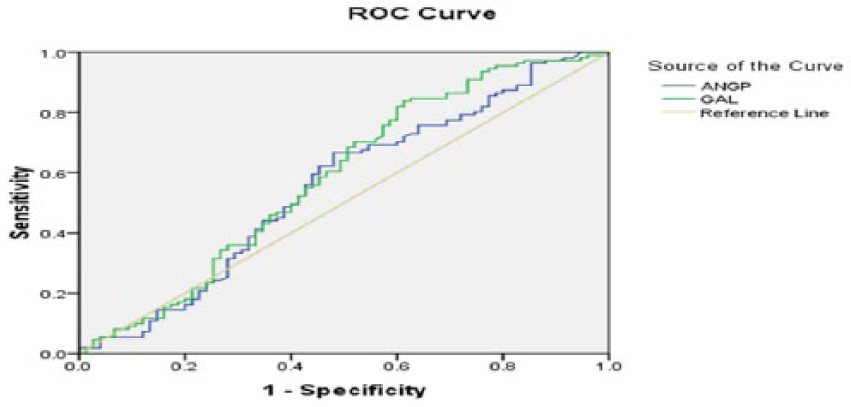
Combined receiver-opening characteristic (ROC) curves of galectin-3 and ANGPTL-4 to predict the need for coronary angioplasty.
Discussion
The main findings of our study were that ANGPTL-4 does not show a significant negative correlation with GRACE risk score in ACS and MI patients. These findings are consistent with an earlier study that showed no significant association between ANGPTL-4 and angiographically characterized coronary atherosclerosis. 16 In contrast a recent study reported that the serum ANGPTL-4 levels at baseline was associated with the occurrence of myocardial no-reflow in acute MI patients treated by primary percutaneous coronary intervention (PCI). Patients with no-reflow had lower levels of ANGPTL-4 and higher levels of vascular endothelial growth factor (VEGF) compared with patients without no-reflow. 17 In MI patients, a condition known as microvascular no-reflow prevails even after successful PCI and its persistence lead to poor outcomes such as mortality and HF. 18 Further, in a preclinical study it was demonstrated that ANGPTL-4 had the ability to inhibit the VEGF-induced vascular permeability; the ANGPTL-4-deficient mice showed increased vascular permeability, hemorrhage, edema, inflammation and increase in infarct size. Hence ANGPTL-4 might be incorporated as a relevant therapeutic target for vascular protection attempting to nullify the effects of VEGF, for prevention of no-reflow and cardio protection during acute myocardial infarction (AMI). 19 Our study could not support the notion that ANGPLT-4 could reflect the severity of CAD. Thus, there is a definite need to understand the role of ANGPTL-4 in the pathogenesis of CAD by well designed, prospective cohort studies where the levels of ANGPLT-4 are measured serially and are correlated with the disease progression.
The present study also reported that the levels of ANGPTL-4 were significantly lower in the control group (7.40 ng/ml) when compared with STEMI (9.42 ng/ml), NSTEMI/UA (10.45 ng/ml) and CSA (10.27 ng/ml) groups. Compared with previous research in the literature where ANGPTL-4 ranged between 7.2–23.3 ng/ml,16,17 we observed lower ANGPTL-4 levels. The deviations in the ANGPTL-4 levels might be due to the digression in the characteristics and race of the study populations. In the studies done by Muendlein and colleagues 16 and Bouleti and colleagues, 17 the race of study population was White whereas in our study the race of the study population was Asian Indian. It may also be due to the heterogeneity in the mean age of the study population; in the current study the mean age was below 60 years whereas in other studies the mean age was above 60 years.16,17 Gender inequality of the study population may also generate contrasting results in the levels of ANGPTL-4; 20 likewise in the Muendlein and colleagues 16 study the number of males in the study population was comparatively lower than the present study. Additionally, the number of diabetic STEMI patients in our study was more when compared with the study done by Bouleti and colleagues 17 Thus, the presence of diabetes could have an influence on the levels of ANGPTL-4. Hence, more well-defined studies with a homogenous population are required to confirm the role of ANGPTL-4 and its correlation with the severity of CAD.
Our study reported a significant positive association between ANGPTL-4 and SCr in CSA patients. Chronic kidney disease (CKD) is defined by the reduction in the estimated glomerular filtration rate (GFR) and patients with CKD have an increased risk of cardiovascular diseases and end-stage renal disease (ESRD).21,22 Our study results matched the results of study done by Baranowski and colleagues 23 where ANGPTL-4 was quantified in patients on chronic hemodialysis (CD) and controls (GFR > 50 ml/min). The ANGPTL-4 levels were five-fold higher in CD patients compared with controls and serum creatinine independently predicted ANGPTL-4 concentrations in control participants. Thus, ANGPTL-4 levels were significantly increased in ESRD and showed an independent association with markers of renal function in control participants. Although the study by Baranowski and colleagues 23 used CD patients, it is worth mentioning that similar findings were observed in our study, highlighting the relationship between ANGPTL-4 and renal function. Diabetic nephropathy (DN) is one of the leading causes of ESRD and albuminuria is an indication of DN which is an independent risk factor for progression of renal and cardiovascular disease. 24 Podocyte injury plays a significant role in the development of DN. 25 In a recent preclinical study done on streptozotocin (STZ), an induced diabetic model, the researchers observed that the upregulation of glomerular ANGPTL-4 occurred earlier than that of albuminuria and podocyte changes in rats. The increase in the glomerular ANGPTL-4 mRNA expression was similar to the albumin-to-creatinine (ACR) ratio and was closely related to albuminuria and podocyte injury. This implied that ANGPTL-4 was primarily secreted from the podocyte; the upregulation of podocyte secreted ANGPTL-4 in DN and its detection in urine indicates that ANGPTL-4 may be used as podocyte injury marker and can be a novel diagnostic and therapeutic marker for DN. 26 Since there are insufficient clinical data on the role of ANGPTL-4 in the pathogenesis of CKD, an independent risk factor of cardiovascular disease; there is definite need to understand the association between ANGPTL-4 and CKD.
Our data showed a significant positive association between ANGPTL-4 and BMI in CSA patients. Besides our study, the Northwick Park Heart Study II (NPHSII) investigated the relationship between plasma ANGPTL-4 and CHD. The results of the (NPHSII) study matched the present study results where plasma ANGPTL-4 levels positively correlated with measures of obesity, such as BMI and body fat mass. 27 However, only middle aged healthy men between (50–63 years) were included in the NPHSII study and the present study comprised of CAD patients. It is known that hypothalamic ANGPTL-4 acts as a downstream mediator of anorexigenic physiological factors. Kim and colleagues 28 have shown that the hypothalamic over-expression of ANGPTL-4 lowered food-intake, body weight gain and increased energy expenditure through regulation of hypothalamic AMP-activated protein kinase (AMPK) pathway and acetyl-CoA carboxylase (ACC) activities. However, this inhibitory effect of hypothalamic ANGPTL-4 was attenuated in obese mice. Thus, the dysregulation of hypothalamic ANGPTL-4 contributed to the pathogenesis of obesity which is one of the risk factors for CAD. 29 Furthermore, the over-expression of ANGPTL-4 suppressed the clearance of triglycerides (TGs) by inhibition of lipoprotein lipase (LPL) and the effect of over-expression of ANGPTL-4 was more pronounced by high fat diet resulting in elevated levels of TGs, free fatty acids and impaired glucose tolerance. Thus, it appears that perturbation in ANGPTL-4 signaling leads to the development of dyslipidemia and obesity. 29 Based on these findings we believe that manipulating the ANGPTL-4 action may serve as therapeutic potential for obesity.
Although several studies have investigated the role of galectin-3 in HF in the past,30,31 there are insufficient data about the role of galectin-3 in CAD. Galectin-3 is a macrophage and endothelium-derived mediator and regulates inflammation that amplifies atherosclerotic plaque progression. 32 We found elevated levels of serum galectin-3 in patients with CAD as compared with the NC group. Previous studies also reported similar findings where galectin-3 levels were significantly higher in CAD patients when compared with non-CAD patients and was an independent predictor of cardiovascular death.33–38 Compared with previous studies36,39 we observed higher concentrations of galectin-3 in CAD patients. Unlike these studies, we used serum instead of plasma to measure the levels of galectin-3 which could possibly affect the concentration of galectin-3. In an earlier study performed by us in MI patients, the median galectin-3 concentration was reported to be much lower (12.3 ng/ml). 40
In the current study, we observed a moderate correlation between galectin-3 and GRACE risk score in ACS patients. Recent studies by Aksan and colleagues 34 and Gucuk Ipek E and colleagues investigated the link between galectin-3 with the severity of CAD and reported that galectin-3 have a significant positive correlation with GENSINI score. This association between galectin-3 and GENSINI score indicates the role of galectin-3 in chronic inflammation and atherogenesis. 41 In the present study a moderate significant positive association was seen between galectin-3 and GRACE risk score which reflected the severity of CAD. However on multivariate analysis this positive correlation was no longer sustained. Thus, galectin-3 may not be useful as an additional assessment in daily clinical practice to detect the severity of CAD and identifying patients with high risk.
Limitations
The main limitation of the current study is that we did not measure the levels of ANGPTL-4 and galectin-3 serially and correlate with the disease progression. Moreover, the duration of symptoms before admission varied from few hours to few days for each patient. Due to logistical reasons, we were unable to perform stress ECG for the 31 control patients. Another limitation of the present study is the small sample size and no follow up was done for the study patients. Thus, future prospective cohort studies with large sample size are needed to confirm our findings.
Conclusion
Our findings revealed that serum ANGPTL-4 and galectin-3 levels are higher in CAD patients than patients with normal coronary arteries. Although circulatory biomarker ANGPTL-4 and galectin-3 significantly correlated with GRACE risk score, these findings were abolished in multivariate analysis. In conclusion, ANGPTL-4 and galectin-3 does not appear to reflect the severity of CAD. Nevertheless these biomarkers do warrant further exploration in improving the management of CAD.
Footnotes
Acknowledgements
We thank Dr A. Kalaiselvi and Ms M. Kamatchi for their assistance in collection of samples. All the authors reviewed and approved the final submitted version of the manuscript.
Funding
We thank the office of the Dean (Medical), SRM Medical College Hospital and Research Centre, Kattankulathur, India for financial support (Ref: CP87/05/2016).
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.