
Abstract
Objective
The aim of this study was to determine the protein expression and prognostic value of epidermal growth factor receptor (EGFR), p53 and galectin-3 in papillary thyroid carcinoma (PTC).
Methods
A retrospective analysis was performed using tumour specimens from patients with PTC who underwent thyroidectomy between July 2007 and December 2008. The percentages of tumour cells staining positively for EGFR, galectin-3 and p53 were determined by immunohistochemistry. Associations between protein expression and age, sex, extrathyroidal extension and lymph node metastasis were assessed, together with the total Metastasis, Age, Completeness of resection, Invasion, Size (MACIS) score (a marker of prognosis). MACIS prognostic scores were categorized into four groups.
Results
Data from 168 patients with PTC (mean follow-up, 35 months) were included. EGFR expression was significantly associated with male sex and lymph node metastasis; p53 expression was higher in males than in females; galectin-3 expression was not significantly associated with age, sex, extrathyroidal extension, lymph node metastasis or total MACIS score category, however.
Conclusion
Immunohistochemical evaluation of EGFR and p53 expression in patients with PTC may be useful for determining prognosis, in PTC patients.
Introduction
Thyroid cancer is the most common malignant tumour of the endocrine system. Because of improvements in living standards and the development of diagnostic techniques, the incidence of thyroid cancer is rapidly increasing. 1 Papillary thyroid cancer (PTC) is the most common form of differentiated thyroid cancer, accounting for 70% of thyroid cancers originating from thyroid follicular cells.2,3
Generally, PTC is associated with a favourable prognosis.2–4 However, up to 10% of patients with PTC die as a direct consequence of this carcinoma, and 22–30% have recurrent disease.2,4 It is therefore important to be able to identify which PTC patients have a poor prognosis, in order to be able to select appropriate treatment. There are no reported predictors of recurrence in thyroid cancer other than clinical risk factors such as old age, male sex and extrathyroidal extension. 5 At the time of thyroid cancer diagnosis, immunohistochemical examination is routinely performed to discriminate between benign and malignant thyroid nodules, but without a great deal of confidence. More specifically, galectin-3 expression is used for the clinical diagnosis of PTC and follicular thyroid cancer. 6 This lectin is frequently overexpressed in PTC tissue but not in normal thyroid tissue, and is involved in the formation and progression of thyroid follicular tumours. 7 Immunohistochemical examination is typically performed not to diagnose follicular tumours of the thyroid gland, but rather to distinguish between types of follicular tumour;6,7 such analysis is more helpful in predicting the patient’s prognosis, rather than in confirming the diagnosis. Epidermal growth factor (EGFR) expression 8 and p53 expression 9 have been found to be significant independent prognostic factors for thyroid cancer.10,11The extent of surgery is generally chosen by analysis of risk factors (such as age, sex, extrathyroidal extension and radiation history), and total thyroidectomy is usually performed in those patients classified as high risk. Histological characteristics (such as immunohistochemical staining) are not used to determine the extent of surgery. Recurrence is frequently found in cervical lymph nodes and is related more to the presence of risk factors than to the type of surgery. Recurrence necessitates another operation (or additional radioiodine ablation) and therefore needs close examination after surgery.
In the present study, the possible usefulness of galectin-3, EGFR and p53 proteins as prognostic predictors in PTC was investigated. A retrospective analysis of the associations between clinical and pathological features of PTC with the expression of these proteins was undertaken.
Patients and methods
This study was approved by the Korea University Guro Hospital Institutional Review Board, 2009. Written informed consent for the use of surgical specimens was obtained from each patient, preoperatively.
Clinical manifestation and histopathology
A retrospective analysis was performed in patients with PTC who underwent surgery between July 2007 and December 2008 at Korea University Guro Hospital. Patients were included in the present analysis if samples of their tumour tissue underwent immunohistochemical evaluation. Histopathological evaluations were performed by the hospital’s pathology department, according to World Health Organization criteria. 12 Clinical presentation was evaluated with regard to age, sex, surgery and distant metastases. Male patients ≥45 years old, with tumours >1 cm in diameter, with evidence of tumour infiltration in the surrounding thyroid tissue, were classified as high-risk patients. Total thyroidectomy or subtotal thyroidectomy was performed in these high-risk patients. Subtotal thyroidectomy was performed on the basis of findings of intraoperative infiltration (which was identified in frozen samples of tissue, excised from around the thyroid gland). Central neck lymph node dissection was also performed in high-risk patients. For other cervical compartments, lateral neck dissection was performed when evidence of lymph node metastasis was found during surgery. Selective neck node radical dissection, including the central neck lymph node, was performed in the low-risk group if lateral neck lymph node metastasis was suspected before surgery, or lymphadenopathy was suspected during surgery. Tumour size, multiplicity, bilaterality, extrathyroidal extension, lymph vessel infiltration and lymph node metastasis were identified evaluation. Extrathyroidal extension was defined as penetration of the thyroid capsule and was classified as pT3 or pT4, according to the 7th American Joint Committee on Cancer (AJCC) staging manual. 13 Although a relationship between lymph node metastasis and thyroid cancer prognosis has not been established, it is generally considered to be an important factor in treatment planning and decision making. The relationship between lymph node metastasis and immunohistochemical factors was therefore investigated.
Patients’ total scores on the Metastasis, Age, Complete resection, Invasion, Size (MACIS) scale
14
were calculated using the following formula:

Immunohistochemistry
Paraffin wax-embedded tumour tissues, which included a region of the surrounding tissue, between 0.5 and 1 mm thick, were fixed in 10% neutral formalin, cut into 4-mm thick sections and placed on silane-coated slides. Slides were deparaffinized in xylene and rehydrated in descending grades of ethanol, beginning with 70% ethanol. The slides were then washed in distilled water and immersed in diluted hydrogen peroxide solution for 10 min, to block intrinsic peroxidase activity. Slides were incubated with dilutions of primary antibodies to galectin-3 (Oncogene, Boston, MA, USA) 1 : 25, p53 (Biogenex, San Ramon, CA) 1 : 50, and EGFR (Dako, Glostrup, Denmark) 1 : 10, for 90 min at room temperature. Slides were then incubated with secondary antibodies (such as rabbit antimouse biotinylated immunoglobulingG for galectin-3, biotinylated goat antimouse antibody for p53 and rabbit antirat antibody for EGFR) for 40 min, and were processed with Tris buffer (pH, 7.6) for 10 min. Following this stage, a streptavidin–biotin universal detection system was used to detect primary antibo dy staining, and immunostaining was developed using a diaminobenzidine chromogen kit (Immunotech, Marseille, France). Slides were then washed with distilled water and counterstained with Mayer’s haematoxylin. The percentage of positively stained tumour cells in tissue samples was used to determine positive staining, according to the following parameters: samples in which ≥5% of cells exhibited p53 nuclear staining; samples in which ≥10% of cells exhibited EGFR staining; samples in which ≥10% of cells exhibited galectin-3 staining. Macrophages obtained from the normal tissue surrounding each tumour sample were used as positive controls for all three expression analyses.
Additional analyses
The associations between EGFR, p53 or galectin-3 expression and age, sex, thyroid involvement, lymph node metastasis and MACIS group were determined, using <45 years and ≥45 years for the age comparison, and the tumour, node, metastasis (TNM) classification 15 to describe the tumour stage.
Statistical analyses
Statistical analyses were performed using SPSS® software, version 13 (SPSS Inc., Chicago, IL, USA). Values were expressed as mean ± SD. The associations between EGFR, p53 or gaclectin-3 expression and age, sex, thyroid involvement, lymph node metastasis and MACIS group 14 were analysed using χ2-test and Student’s t-test. P values <0.05 were considered statistically significant.
Results
Clinical and pathological characteristics of 168 patients with papillary thyroid carcinoma (PTC), included in a retrospective study investigating prognostic predictors of PTC.

Data presented as n (%) or mean ± SD.
MACIS (Metastasis, Age, Complete resection, Invasion, Size) scores 14 were grouped as follows: group 1 ≤ 5.9; group 2, 6.0–6.99; group 3, 7.0–7.99; group 4, ≥8.0.
Associations between epidermal growth factor receptor (EGFR) protein expression in tumour tissue and clinical or histopathological findings in 168 patients with papillary thyroid carcinoma.
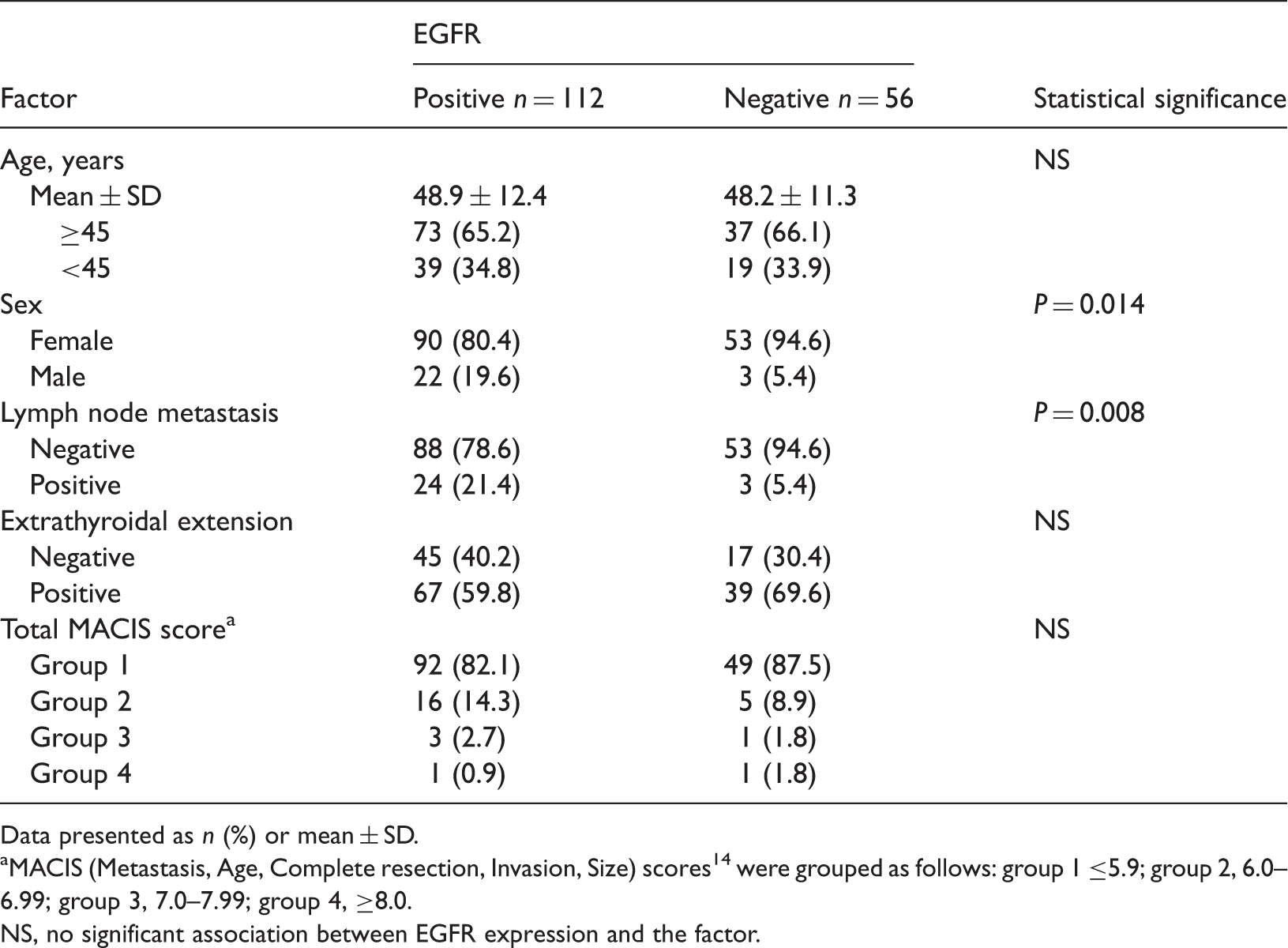
Data presented as n (%) or mean ± SD.
MACIS (Metastasis, Age, Complete resection, Invasion, Size) scores 14 were grouped as follows: group 1 ≤5.9; group 2, 6.0–6.99; group 3, 7.0–7.99; group 4, ≥8.0.
NS, no significant association between EGFR expression and the factor.
Associations between p53 protein expression in tumour tissue and clinical or histopathological findings in 168 patients with papillary thyroid carcinoma.
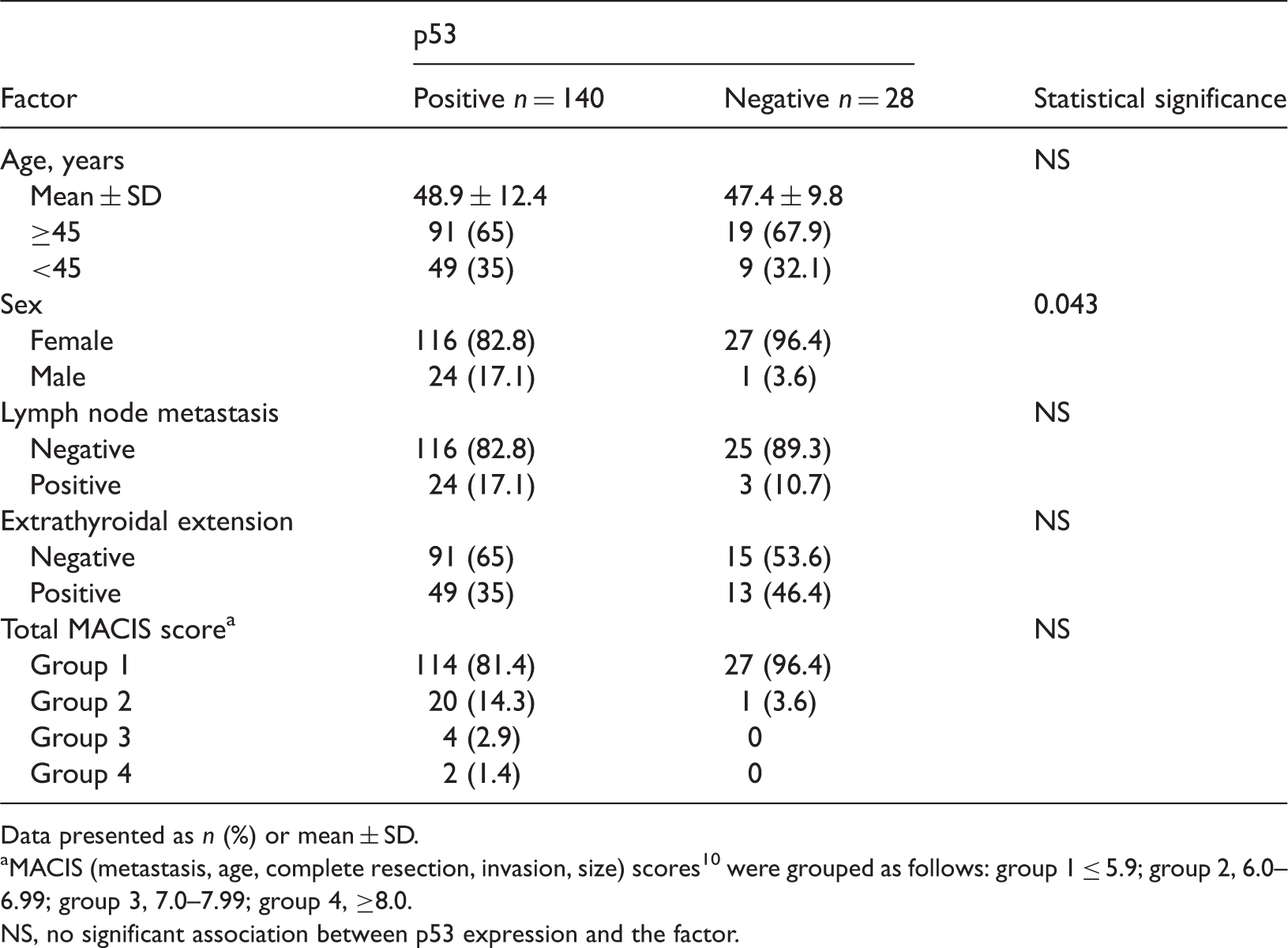
Data presented as n (%) or mean ± SD.
MACIS (metastasis, age, complete resection, invasion, size) scores 10 were grouped as follows: group 1 ≤ 5.9; group 2, 6.0–6.99; group 3, 7.0–7.99; group 4, ≥8.0.
NS, no significant association between p53 expression and the factor.
Associations between galectin-3 protein expression in tumour tissue and clinical or histopathological findings in 168 patients with papillary thyroid carcinoma.
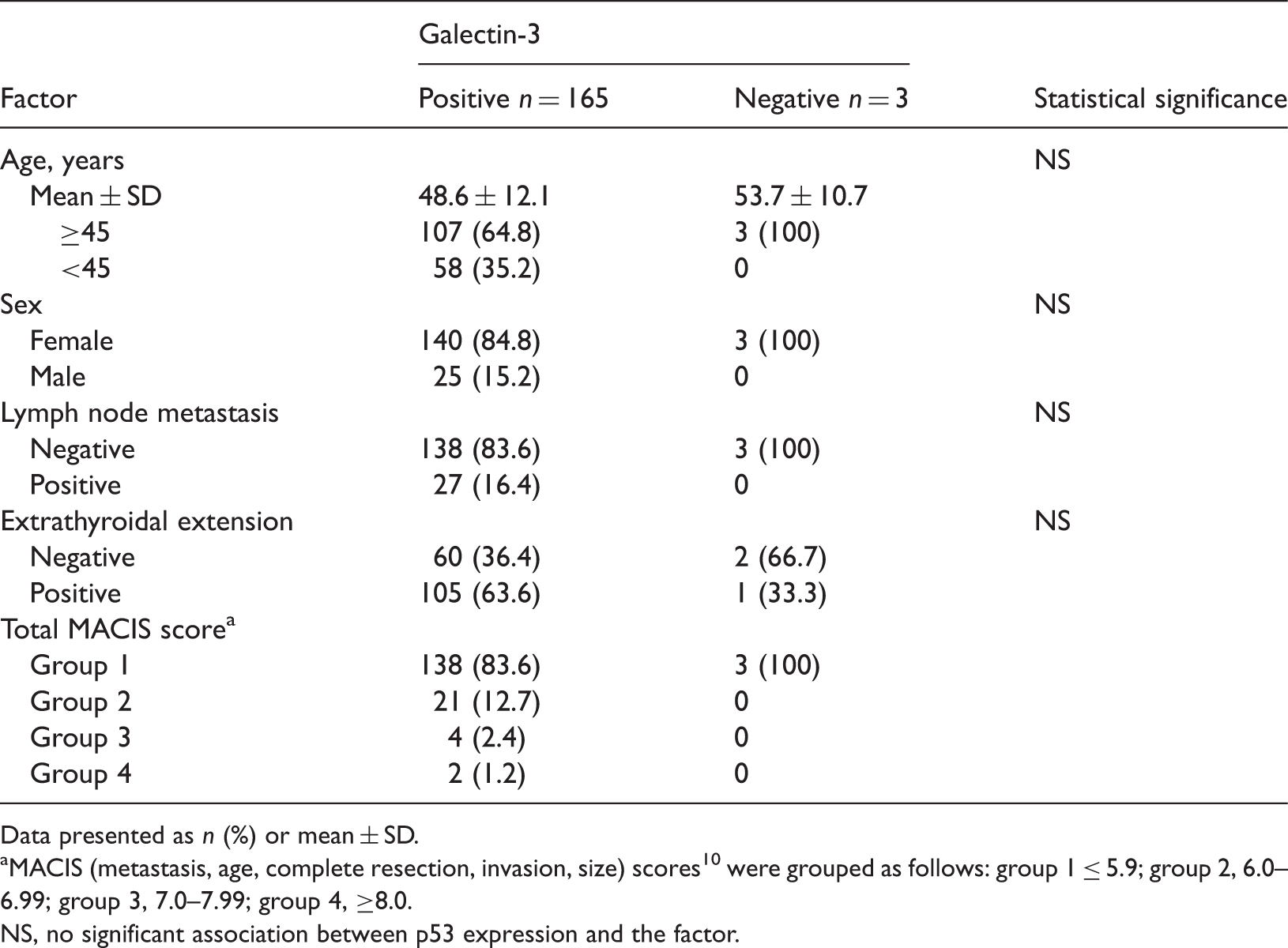
Data presented as n (%) or mean ± SD.
MACIS (metastasis, age, complete resection, invasion, size) scores 10 were grouped as follows: group 1 ≤ 5.9; group 2, 6.0–6.99; group 3, 7.0–7.99; group 4, ≥8.0.
NS, no significant association between p53 expression and the factor.
Discussion
In general, PTC is associated with a favourable prognosis and a low mortality rate.2–4 PTC, like follicular thyroid carcinoma, is classified as a well-differentiated thyroid cancer. However, some PTC cases have a poor prognosis.2,4 It is therefore important to investigate predictors of recurrence and mortality in PTC.
Age, sex and extrathyroidal extension are currently used as predictors of prognosis for PTC.16–18 Tumour stage is often associated with poor prognosis.2,4 The MACIS, TNM and European Organization for Research and Treatment of Cancer tumour staging systems are practical, and are highly accurate in predicting the risk of disease recurrence and survival.19–21 Immunohistochemical factors are commonly used to diagnose thyroid cancer. The present study therefore examined the associations between immunohistochemical factors and age, sex, extrathyroidal extension and MACIS group, in PTC patients.
Since 2006, we have studied the association between thyroid cancer prognosis and immunohistochemical factors including EGFR, p53, galectin-3 and high molecular weight cytokeratin (HMW-CK). Expression of CK19 protein, which is a HMW-CK, is routinely evaluated in postoperative pathology tests because CK19 is typically uniformly expressed in PTC tumours. 22 Such research is important because it can evaluate the efficacy and clinical significance of these routine immunohistochemical tests, and should make it possible to improve the immunohistochemical parameters that are used for pathological examination of the thyroid. In the patient group studied in our present retrospective analysis, we found that HMW-CK and CK19 were uniformly expressed in PTC tumours. However, these data were excluded from the present article because the purpose of the study was to identify predictors of prognosis.
Encoded by the c-erb proto-oncogene, EGFR promotes cell growth and differentiation. 23 EGFR is frequently overexpressed in malignant tumours, including breast and bladder cancers. 24 Many studies have reported the overexpression of EGFR in an anaplastic, undifferentiated subtype of PTC that is associated with a high mortality rate.25–28 However, little is known about the value of EGFR expression in predicting the prognosis of thyroid carcinoma. Mizukami et al. 27 reported a significant association between EGFR expression and PTC recurrence. Akslen et al.28–30 demonstrated that EGFR expression is a significant and independent prognostic factor in PTC. In multivariate analysis, cytoplasmic EGFR expression showed a significant correlation with tumour infiltration in surrounding thyroid tissue and recurrence-free survival. 28 In the present study, EGFR was highly expressed in male PTC patients, and in PTC patients with lymph node metastases. Our findings are in agreement with others who demonstrated that EGFR expression is a predictor of poor prognosis,28–30 and suggest that evaluation of EGFR expression as a predictor of prognosis may be applicable in the clinical setting. The present study did not evaluate the relationship between EGFR expression and recurrence-free survival or overall survival rate because of the short follow-up period (35 months).
p53 is a tumour suppressor gene involved in cell-cycle control. Immunohistochemical expression of p53 in thyroid cancer indicates the existence of a p53 variant or an inactive p53 mutation.8,9 Inactive p53 mutations are uncommon in well-differentiated thyroid carcinomas. However, p53 expression was observed in well-differentiated (10–18%) and poorly differentiated (40–80%) thyroid carcinomas, in one study. 31 Mutation and overexpression of p53 were observed more often in PTC when lymph node metastasis was present, 8 or when dedifferentiation to anaplastic carcinoma had occurred.32,33 According to Hosal et al. 8 and Godballe et al., 9 p53 expression is a significant independent prognostic indicator of PTC. The present study showed that p53 expression was significantly higher in PTC tumours found in male patients. Other studies have reported that male PTC patients, and patients with poorly differentiated thyroid carcinomas, have a poor prognosis. 34 These findings support a relationship between PTC prognosis and p53 expression. In the present study, p53 expression was not significantly associated with extrathyroidal extension, lymph node metastasis, or with MACIS group classification. 14 Of the 168 patients studied, 83.9% (n = 141) were low-risk patients (MACIS group 1). However, 81.4% (114/140) of the low-risk patients and 83.3% (140/168) of the entire study population had p53-positive tumours. Therefore, the lack of a significant association between p53 expression and MACIS score was probably the result of the high expression rate of p53 among PTC patients at the hospital. Although not statistically significant, age ≥45 years, extrathyroidal extension, high MACIS score and presence of lymph node metastasis were all associated with increased expression of p53.
Galectin, a carbohydrate-binding protein of the lectin family, is present in the nucleus, cytoplasm, cell membrane and extracellular matrix, and is involved in cell growth, differentiation and adhesion. 35 The expression rate for galectin-3 was 98.2 % in our present series of thyroid cancer specimens, and our findings indicate that the specificity for galectin-3 in thyroid cancer is therefore very high.
Other research has also demonstrated a high rate of galectin-3 expression in thyroid cancers. 6 Thus, the use of galectin-3 to detect papillary and follicular carcinomas has been proposed, and galectin-3 expression is a widely used diagnostic marker for these diseases. 6 However, few studies have investigated the utility of galectin-3 expression in the prognosis of PTC. Although galectin-3 does not appear to be a prognostic factor, it has substantial merit in distinguishing between benign and malignant tumours. 7 In our study, galectin-3 was not significantly associated with lymph node metastasis.
In conclusion, our current study showed that expression of EGFR and p53 was significantly higher in male than in female patients with PTC. Furthermore, a significant association between EGFR expression and lymph node metastasis was observed. These results indicate that EFGR and p53 expression are predictors of prognosis in PTC, and their use as diagnostic tools in the clinical setting is therefore warranted. We suggest that suppression of thyroid stimulating hormone (by levothyroxine administration or radio-iodine ablation treatment), careful examination for recurrences and checking thyroglobulin levels or sophisticated imaging studies should be considered in EGFR- and p53-positive patients with PTC.
Footnotes
Declaration of conflicting interest
The authors had no conflicts of interest to declare in relation to this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors