
Abstract
Nitric oxide (NO) has a significant role in modulating the respiratory system and is being exploited therapeutically. Neonatal respiratory failure can affect around 2% of all live births and is responsible for over one third of all neonatal mortality. Current treatment method with inhaled NO (iNO) has demonstrated great benefits to patients with persistent pulmonary hypertension, bronchopulmonary dysplasia and neonatal respiratory distress syndrome. However, it is not without its drawbacks, which include the need for patients to be attached to mechanical ventilators. Notably, there is also a lack of identification of subgroups amongst abovementioned patients, and homogeneity in powered studies associated with iNO, which is one of the limitations. There are significant developments in drug delivery methods and there is a need to look at alternative or supplementary methods of NO delivery that could reduce current concerns. The addition of NO-independent activators and stimulators, or drugs such as prostaglandins to work in synergy with NO donors might be beneficial. It is of interest to consider such delivery methods within the respiratory system, where controlled release of NO can be introduced whilst minimizing the production of harmful byproducts. This article reviews current therapeutic application of iNO and the state-of-the-art technology methods for sustained delivery of NO that may be adapted and developed to address respiratory disorders. We envisage this perspective would prompt active investigation of such systems for their potential clinical benefit.
Introduction
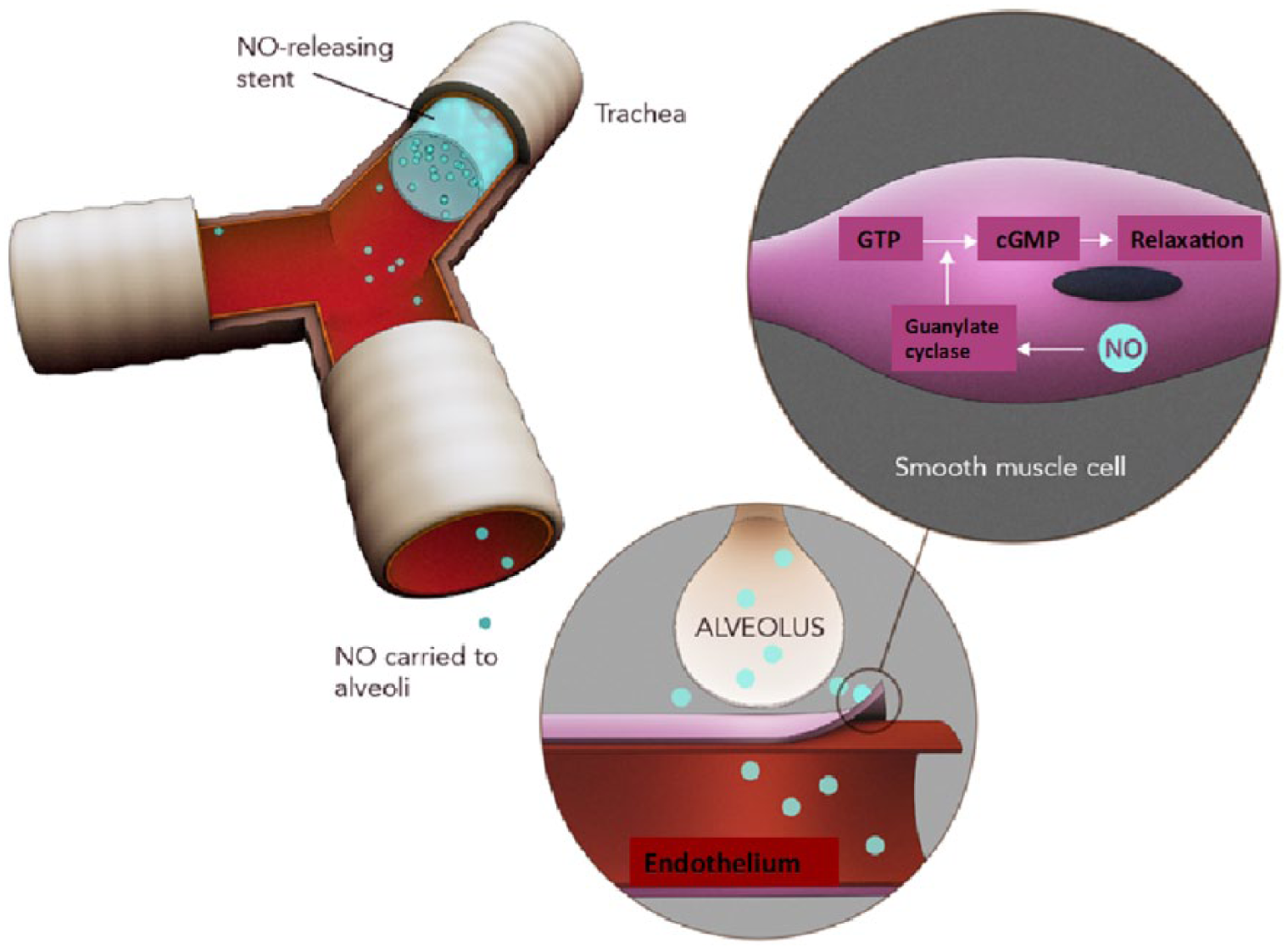
Nitric oxide (NO) has a significant role in modulating the respiratory system and is being exploited therapeutically [Bloch et al. 2007]. Neonatal respiratory failure can affect around 2% of all live births and is responsible for over one third of all neonatal mortality [Steinhorn, 2010]. Inhaled NO (iNO) can help ease breathing difficulties in neonates by reducing pulmonary vascular resistance, pulmonary edema, severe hypoxia and lung inflammation [Ghanta et al. 2013; Love and Bradshaw, 2012]. iNO also improves pulmonary angiogenesis and lung alveolarization, as well as protecting against infection with no significant adverse effects on growth or neurodevelopmental status [Walsh et al. 2010]. iNO, at concentrations of 5 to 80 ppm has been shown to reverse ventilation perfusion mismatching caused by lung injury, decrease pulmonary artery pressure and improve oxygenation and cardiac output [Frostell et al. 1991] without causing systemic hypotension [Kinsella et al. 1992] (Figure 1).

Schematic of the action of inhaled nitric oxide (iNO) in the lung leading to improved ventilation–perfusion matching (central image) and the mechanism underlying vasodilatation (top right).
The essential role of NO in the pulmonary circulation has been demonstrated in animal models where postnatal adaptation of the pulmonary circulation is enhanced with NO inhalation [Duong-Quy et al. 2014]. Oxygen tension increases NO production in foetal pulmonary artery endothelial cells [Balasubramaniam et al. 2006] and can thus lead to pulmonary vasodilation. Normal basal pulmonary resistance and low pulmonary pressures are maintained by complex haemodynamic effects of NO produced at physiological concentrations of 100 pmol–5 nmol [Hall and Garthwaite, 2009]. NO has a short half-life of 2–5 seconds [Peliowski, 2012]. It is readily soluble in water with 4.7 per 100 parts volume at 20 degrees (1 atm) [Tawashi, 1997]. NO is also lipid soluble and thus freely traverses cell membranes and rapidly diffuses into the target area, over distances of 150–500µm [Saraiva et al. 2011].
NO is predominantly synthesized in vascular endothelial cells from the amino acid L-arginine via the action of an enzyme nitric oxide synthase (NOS). In the mammalian lung, NO is synthesized by three NO synthases: neuronal (nNOS), inducible (iNOS) and endothelial (eNOS)]. Endothelial NOS appears to play a role in maintaining low pulmonary vascular tone [Bloch et al. 2007].
In the airways, NOS is present in a number of cells, including vascular endothelial cells, airway epithelial cells, macrophages and neurons. NO reacts with oxygen to form nitrogen dioxide and nitrite resulting in pulmonary vasodilatation; it then diffuses into the bloodstream and interacts with oxyhaemoglobin to produce methaemoglobin (metHb) and nitrate [Soll, 2009]. It was traditionally thought this would lead to the loss of NO’s vasodilating properties in the systemic circulation. However, nitrosylation of a cysteine residue of the haemoglobin β subunit leads to formation of a stable derivative that retains vasodilatory properties that can increase blood flow and oxygen delivery to the system vasculature [Creagh-Brown et al. 2009].
NO acts via both cyclic guanosine monophosphate (cGMP)-dependent and -independent mechanisms. NO regulates vascular tone by activating soluble guanylate cyclase (sGC). It also plays a role in reducing inflammation via signal-transduction events independent of cGMP [de Mel et al. 2011; Chester et al. 2011]. When inhaled, NO diffuses from the alveolar space to vascular smooth muscle cells and causes vasorelaxation via the same mechanism as endogenous NO. It activates sGC that catalyzes the dephosphorylation of GTP to cGMP-dependent protein kinase (Figure 1). cGMP inhibits calcium entry into the cells. The reduction of calcium reduces the ability of myosin light-chain kinase (MLCK) to phosphorylate the myosin molecule, preventing cross-bridging and thus causing vasorelaxation. It also activates potassium channels leading to hyperpolarization and relaxation (Figure 1) [Berkelhamer et al. 2013; Soll, 2009]. NO also acts via cGMP-independent mechanisms, including interaction with haem-containing molecules, proteins with reactive thiol groups and superoxide radicals [Bloch et al. 2007].
Applications of iNO include diseases such as pulmonary hypertension, bronchopulmonary dysplasia (BPD) and hypoxaemic respiratory failure. iNO has been considered an advantage over traditional treatment measures for the above diseases due to its ability to improve oxygenation by selectively vasodilating the pulmonary vasculature [Steinhorn, 2010]. Currently, iNO is used successfully in the late preterm and term population of patients with persistent pulmonary hypertension (PPHN) [Keszler, 2012]. However, its use in other paediatric respiratory diseases has been associated with differential outcomes. iNO is administered via mechanical ventilation, which, when prolonged, can lead to ventilator-induced diaphragmatic dysfunction and respiratory muscle atrophy [Powers et al. 2009; Jubran, 2006]. iNO administration often requires prolonged hospital stay, use of intensive care services and trained staff, hence is also a relatively expensive treatment [Peliowski, 2012].
This article reviews current therapeutic application of iNO and the state-of-the-art technology methods for sustained delivery of NO, which may be adapted and developed to address respiratory disorders. One of the limitations of current studies is the lack of identification of subgroups [BPD, PPHN, acute respiratory distress syndrome (RDS)] and homogeneity in powered studies to derive a conclusion; this is discussed further in the relevant sections. Development of novel methods of NO delivery is warranted to improve outcomes and overcome limitations in current treatment of paediatric respiratory diseases such as the use of mechanical ventilation, which can acquire high costs. We believe this review will stimulate research that would lead to overcoming such limitations associated with current methods of NO administration to the respiratory system and eventually offer greater socio-economic benefits.
Clinical indications for use of inhaled nitric oxide
Persistent pulmonary hypertension
PPHN is a syndrome characterized by extrapulmonary left-to-right shunting of blood across the ductus arteriosus and possibly the foramen ovale. It affects 1–2 infants per 1000 live births [Steinhorn, 2010]. Infants often present with severe cyanosis despite receiving high levels of oxygenation, and mortality for the condition remains between 5–10%. PPHN is generally categorized into one of three types: abnormally constricted pulmonary vasculature due to lung parenchymal diseases (e.g. meconium aspiration syndrome, the most common cause of PPHN), RDS, or pneumonia; or idiopathic PPHN (seen in 10%), with normal lung parenchyma but remodelled pulmonary vasculature [Nair et al. 2012] or underdeveloped vasculature, as seen in conditions such as congenital diaphragmatic hernia. The pathophysiological conditions that lead to overall constricted airflow to the lungs may be associated with a low density of vasculature as well as thickened smooth muscle with a resulting increase in pulmonary arterial pressure greater than 25mmHg [Steinhorn, 2010].
PPHN is responsible for complications in approximately 10% of infants with respiratory failure and even with appropriate therapy, approximately 25% of infants with moderate or severe PPHN exhibit significant neurodevelopmental impairment at 12–24 months and seizures that result from the underlying hypoxaemia and aggressive treatments of PPHN [Steinhorn, 2010]. Initial therapeutic options for PPHN include a combination of treatments such as high-frequency ventilation, surfactant, blood pressure optimization, correction of electrolyte imbalance and iNO. The use of intravenous vasodilators can be problematic due to its tendency to cause systemic vasodilatation. When infants do not respond to conventional treatment they are treated with extracorporeal membranous oxygenation (ECMO). Various studies have shown that iNO improves arterial oxygen levels and is able to reduce the use of ECMO by up to 40% [Bloch et al. 2007]. ECMO is an invasive procedure that requires cannulation of large vessels, anticoagulation and high levels of intensive care support. The Neonatal Inhaled Nitric Oxide Study Group showed an 18% reduction in the need for ECMO in term infants with PPHN [Neonatal Inhaled Nitric Oxide Study Group, 1997]. The Clinical Inhaled Nitric Oxide Research Group showed a 26% reduction in the need for ECMO with the use of iNO [Clark et al. 2000]. These findings led to the approval of iNO by the US Food and Drug Administration in 2000 to treat term and near-term infants (born after the 34th week of pregnancy) with hypoxic respiratory failure and pulmonary hypertension [Raffay et al. 2012].
Although iNO does reduce the use of ECMO, it has not been shown to reduce mortality [Soll, 2009]. Furthermore, the initiating dose of iNO for PPHN by neonatologists varies considerably with the most common effective dose being 20ppm [Shivananda et al. 2012]. Patients who do not respond can be treated with higher doses of up to 80 ppm, however, this increases the risk of methaemoglobinaemia [Puthiyachirakkal and Mhanna, 2013].
Maintaining adequate oxygenation is the mainstay of PPHN therapy. Hypoxia contributes to the pathophysiology of PPHN, however hyperoxia can cause free-radical damage, increase contractility of pulmonary arteries and reduce response to iNO. The oxygen saturation levels in infants with PPHN must be maintained around 95% or higher with Pa O2 levels between 55 and 80 mmHg [Steinhorn, 2010]. Up to 40% of patients fail to respond to iNO [Steinhorn, 2010]. This may be due to changes in downstream signalling mechanisms in pulmonary vascular smooth muscle cells such as abnormal expression and reduced activity of sGC [Steinhorn, 2010; Steinhorn et al. 1995], which would reduce responses to iNO. In these situations, direct sGC stimulators that are NO- independent might offer a way forward [Chester et al. 2011]. Alternative methods of iNO administration, for example, via nasal cannula without requiring mechanical ventilation, have been reported [Wilkinson et al. 2011], however, long-term data regarding efficacy are warranted.
Bronchopulmonary dysplasia
BPD is a chronic lung disease that commonly occurs in premature infants born before 32 weeks, weighing less than 1250 g, who have received positive pressure ventilation during the first 2 weeks of life and are still requiring supplemental oxygen to maintain oxygen saturations at 28 days of age [Strueby and Thebaud, 2014]. The use of mechanical ventilation interferes with alveolar and pulmonary vasculature development. This accounts for a substantial proportion of the admissions to the UK neonatal intensive care units. The overall incidence of BPD is reported at about 20% of ventilated newborns. These infants are also substantially more likely to be re-admitted to the intensive therapy unit and require further mechanical ventilation at a later date, increasing costs further [Mourani et al. 2014]. Premature birth disrupts pulmonary vascular growth, causing abnormal pulmonary vascular remodelling, which may lead to pulmonary hypertension [Baker et al. 2014]. It is also associated with reduction in levels of endothelial progenitor cells and vascular endothelial growth factor (VEGF) leading to endothelial dysfunction [Qi et al. 2013].
iNO therapy has been shown to improve lung growth and reduce pulmonary hypertension in animal BPD models [Cole et al. 2011] with increased levels of EPCs and VEGF [Baker et al. 2014]. One large multicentre study demonstrated that iNO significantly improved survival rates of BPD at 36 weeks, decreased the duration of hospitalization, and reduced the need for respiratory support [Ballard et al. 2006]. iNO therapy delivered to premature infants between 7 and 21 days of age has been shown to improve the pulmonary outcome in these patients, with no short-term adverse effects [Hibbs et al. 2008]. Long-term studies have shown that iNO therapy does not cause adverse neurodevelopmental effects [Walsh et al. 2010] and patients make fewer outpatient visits to receive respiratory medications after discharge from the intensive care unit [Mercier et al. 2010].
However, early use of low-dose iNO in premature babies does not reduce the incidence of BPD [Mercier et al. 2010], suggesting that using iNO as a preventative treatment strategy may be ineffective. Moreover, in premature infants, iNO has several risks, such as increasing bleeding time and decreasing platelet aggregation, resulting in an increased risk for intraventricular haemorrhage [Love and Bradshaw, 201]. Furthermore, a meta-analysis of 11 randomized controlled trials revealed no benefit in decreasing mortality, neurodevelopmental delay, or development of BPD with the use of iNO in preterm infants less than 34 weeks [Donohue et al. 2011]. However, the robustness of the meta-analysis regarding the use of iNO in BPD lacks credibility, due to the lack of homogeneity between the studies, with variable subject ages, different methods of iNO administration and inhomogeneous study timelines. It is therefore important for clinicians to analyse individual studies to decide how to use iNO and whether it may be suitable for their group of patients. Subgroups of preterm infants who might benefit from iNO include infants with less severe respiratory disease, those treated with higher iNO dose and African patients. However, subgroup analyses must be interpreted cautiously and require validation in prospective studies [Jensen and Kirpalani, 2014].
Neonatal respiratory distress syndrome associated pulmonary hypertension
Neonatal RDS is a disease characterized by reduced surfactant secretion from type III alveolar cells leading to atelectasis and subsequent ventilation–perfusion (V/Q) mismatching. Premature infants in respiratory failure may exhibit dramatic improvements after treatment with exogenous surfactant [Bahadue and Soll, 2012]. iNO is safe to use in patients with RDS to transiently improve oxygenation [Dzierba et al. 2014]. iNO may benefit such infants by selectively dilating the pulmonary vasculature, improving V/Q matching, and decreasing the pulmonary inflammatory response. iNO’s greatest advantage appears to be in reducing incidence of chronic lung disease in premature infants with RDS [Schreiber et al. 2003].
iNO therapy alone has been shown to reduce mortality rates in preterm infants [Dzierba et al. 2014]. Some preterm patients may also have other respiratory problems in addition to pulmonary hypertension, such as suboptimal responses to surfactant. In these patients, iNO therapy may be used in combination with exogenous surfactant. The iNO can be used to dilate the pulmonary vasculature and exogenous surfactant to recruit and stabilize the alveoli. The combination therapies may be complementary to one another and result in measurable clinical benefits in RDS [Uy et al. 2000].
Term infants with RDS do not appear to benefit greatly from iNO, with no apparent reduction in length of stay in the intensive care unit [Afshari et al. 2011] or mortality rates [Adhikari et al. 2014].
Interestingly, although increased pulmonary arterial pressures is a prominent feature of RDS, current treatment focus doesn’t address improving pulmonary haemodynamics but instead focuses on improving oxygenation. The effect of iNO on pulmonary hypertension and right-ventricular function, and whether targeting these will reduce mortality rates has not, to date, been addressed.
Limitations of inhaled nitric oxide application as a therapy
The molecular mechanisms of NO in modulating vascular resistance suggest it should have an immediate positive effect in restoring pulmonary circulation and maintaining physiological function of the respiratory system. Studies in animal models consistently confirm this positive effect of iNO [Maruyama et al. 2013]. However, clinical trials seeking to replicate these results in preterm infants are far less conclusive. In 2011, a consensus panel reviewed the published evidence on the efficacy and safety of iNO in preterm infants. They concluded that current evidence did not support the routine use of iNO in the care of premature infants less than 34 weeks gestation who require respiratory support [Cole et al. 2011]. However, as noted by the consensus, previous randomized controlled trials did not prospectively identify subgroups of respiratory failure. Therefore, the inconclusive results of the trials may be due to the variability in patient populations and differences in the underlying pathophysiology of their respiratory failure. Smaller studies in targeted populations suggest that iNO significantly improves oxygenation [Dzierba et al. 2014], improves survival and lowers incidence of BPD [Ballard et al. 2006; Walsh et al. 2010] and reduces need for ECMO in patients with PPHN [Soll, 2009]. This demonstrates the importance of identifying and targeting therapy to appropriate patient subgroups that are most likely to have a response to iNO and performing adequately powered trials in homogenous populations. For example, PPHN is characterized as being one of three types and it may be paramount of significance to identify the underlying condition that results in PPHN as not all underlying conditions may uniformly respond to NO. Another example is associated with acute respiratory distress syndrome (ARDS) where the current consensus is that iNO does not positively improve outcome parameters. However, NO may improve lung functionality via various mechanisms such as increasing levels of lung surfactant [Sun et al. 2003]. Therefore, there is currently a need for an ideal study that looks at all the outcome parameters of iNO to determine its true value in ARDS.
NO can rapidly oxidize haemoglobin to metHb, which reduces the oxygen carrying capacity of haemoglobin. This can cause tissue hypoxia if concentrations are substantially elevated. It is important to measure metHb levels within 1 hour after initiating the iNO therapy using an analyser, and subsequently, every few days. However, highly localized NO delivery methods may, in principle, minimize these limitations [Puthiyachirakkal and Mhanna, 2013]; iNO may interact with other drugs and thus the use of other vasodilators must be undertaken with caution. In addition, any drugs that have a known tendency to increase metHb concentrations, for example, prilocaine, can lead to toxicity. NO also may form peroxynitrite with superoxide, which can cause tissue damage through further redox reaction [Pacher et al. 2003].
NO forms nitrogen dioxide (NO2) in the presence of oxygen and could lead to pulmonary oedema and lung injury at high doses. iNO at maximum dose of 80 ppm (which represents the maximum rate of NO formation likely to be encountered) can be delivered safely in a well designed, continuous-flow neonatal ventilatory circuit. However, other sources of NO that could lead to the formation of NOx species within the conductive airways and at the alveolus need to be considered when estimating the total NO2 delivery to the patient [Sokol et al. 1999]. Therefore, it is recommended that the starting dose of iNO should be 20 ppm in adults and 10 ppm children [Tworetzky et al. 2001]. The dose should then be weaned down to 5 ppm providing the arterial oxygenation is adequate. However, whether this will be adequate in a ventilated patient depends on the type of ventilator circuit, the response time of the analyzer, the ventilatory pattern and the NO analysis in the circuit.
Nitric oxide delivery systems
One of the problems with NO is developing a delivery system that can deliver a reliable concentration of the gas during mechanical ventilation. To optimize the accuracy of NO delivery, inspired gas should be premixed proximal to the ventilator to maintain constant NO delivery regardless of ventilatory pattern [Imanaka et al. 1997]. The INOvent delivery system (Siemens and Dragger, Wisconsin, USA) is an iNO system that controls delivery by mass rather than volume or velocity, and attempts to address delivery of reliable and controlled concentrations of NO with the aid of ventilators. The INOvent provides a constant NO concentration independent of the ventilatory pattern, and NO2 formation is minimal [Kirmse et al. 1998].
Methods of analysis must also be selected carefully; chemiluminescence analysers that are typically used to monitor the concentration of NO are slow and only reliable when NO is injected at a constant rate into the inspiratory limb of a ventilator circuit. When inspiratory flow is not constant, NO delivery is variable and unpredictable and this cannot be accurately measured using the analysers due to their slow response time [Sydow et al. 1997].
Prolonged mechanical ventilation can cause barotrauma, subglottal stenosis, chronic pulmonary injury, and psychological alterations. Furthermore, abrupt discontinuation of iNO may lead to rebound pulmonary hypertension, causing decreased cardiac output and systemic hypotension [Bloch et al. 2007]. This may occur due to downregulation of endogenous NO synthase, reduced guanylyl cyclase activity and reduced cGMP levels during iNO administration. Stopping iNO is thus associated with pulmonary vasoconstriction until levels become replete [Namachivayam et al. 2006].
Weaning failure can also lead to the common complication of ventilator-induced diaphragmatic dysfunction [Heunks and Van Der Hoeven, 2010], in which there is muscle fibre injury and atrophy within the diaphragm [Kallet, 2011]. This results in increased intensive care stay and healthcare costs [Petrof et al. 2010].
Novel interventions for addressing associated vascular phenomenon?
The above limitations lead us to envisage potential improvements or alternatives to current methods of NO delivery. NO diffuses over distances of only 150–500µm [Saraiva et al. 2011]. The targeted delivery of NO with a controlled sustained-release rate is thus difficult, and an intervention that could potentially allow NO to reach the target site in a more controlled manner, as a trigger response, whilst being able to bypass a long distance through the upper airway, might be desirable. One of the primary aims would be to avoid systemic symptoms, thus systemic routes of administration are not an obvious choice.
Encapsulation of NO donors with various platforms such as nanoparticles, microparticles and polymers is a promising field for enabling pulmonary absorption. Various encapsulation methods of these platforms with NO and other drugs have shown sustained release of the drug in the pulmonary system. These are summarized in Figure 2 and Table 1. As indicated with the respective studies included in the table, NO can be encapsulated with biodegradable polymers [Jeh et al. 2004], with microspheres [Verma et al. 2013] and liposomes [Huang et al. 2009] which can be subsequently inhaled for a controlled NO release. Dendrimers have been successfully conjugated with drugs such as low-molecular-weight heparin, which can be delivered to the pulmonary system [Bai and Ahsan, 2009]. We speculate that NO could be similarly conjugated with dendrimers for delivery to the lung. In-vitro studies have shown that lung-targeted peptide-micelle conjugates can deliver therapy for pulmonary artery hypertension (PAH). In-vitro studies in rat pulmonary arterial smooth muscle cells, have shown that fasudil (an anti-PAH drug) which, has been loaded in micelles and subsequently inhaled leads to a more sustained release in the lung and greater cellular uptake compared with the free unloaded fasudil [Gupta et al. 2014]. The inner core of micelles are hydrophobic, have good drug-loading capacity and are able to evade breakdown by the reticuloendothelial system, thereby prolonging drug release in the lung [Jo et al. 2009]. Combining NO with micelles may therefore be a promising therapy for PAH. Combining NO with other drugs such as prostaglandin-based drugs to act in synergy is also promising [Mollace et al. 2005].

Nitric oxide release systems.
Examples of nitric oxide delivery systems to the pulmonary system.

DVT, deep vein thrombosis; HBE, human bronchial epithelial cells; LMWH, low-molecular-weight heparin; MP, microsphere; NO, nitric oxide.
The NO-sGC-cGMP pathway may be disrupted in patients with pulmonary hypertension, which may lead to a decrease in NO bioavailability. Therefore, drugs that can activate sGC (the enzyme that produces cGMP) independently of NO may be of therapeutic benefit. Recently, two classes of compounds that can amplify the action of sGC have been discovered: sGC stimulators and sGC activators [Chester et al. 2011] (Figure 3). sGC can exist in a haem-containing form (stimulators) and haem-independent form (activators). sGC activators are useful in diseased states where resistance to NO has developed by activating oxidized or haem-deficient sGC enzymes. sGC stimulators directly stimulate sGC independent of any action with NO, however, they demonstrate strong synergistic enzyme activation when combined with NO and NO donors, thereby increasing the bioavailability of NO. Recently, riociguat, a novel sGC stimulator, was shown to reduce pulmonary vascular resistance in patients with adult PAH [Ghofrani et al. 2013]. Although these studies have not translated to the paediatric population, studies looking at the NO-sGC-cGMP pathway in paediatric respiratory diseases and the potential benefit of sGC stimulators and activators are warranted.

Classes of nitric oxide (NO) donors and soluble guanylate cyclase (sGC) activators and stimulators.
Airway implants and NO-eluting particles are well established concepts [Naghavi et al. 2013]. NO-eluting particles and implants are predominantly established for cardiovascular-system as well as for wound-healing scaffolds, and it would be potentially desirable to have such platform technologies to present NO within the pulmonary system.
Synergizing airway interventions with vascular therapeutics?
Airway implants have been traditionally employed for relieving obstructing malignant lesions. They have resulted in significant symptomatic improvement in the majority of patients with low risk of complications. In the paediatric population, stents are commonly used for tracheobronchial stenoses and airway malacia that cause weakness of the cartilage in the trachea or bronchus [Bacon et al. 2014]. The use of stents in treating airway malacia has proved efficient in stabilizing the airway and been shown to prevent apnoea and poor feeding. Airway stents have traditionally been made of silicone or expandable metal stents. Silicone stents can be easily repositioned and removed (Figure 4). Tracheal stents face numerous challenges which include: tracheal prosthetic materials eroding into the lumen or nearby structures, infection due to being exposed to unsterile external environment, inflammation, granulation tissue formation and stenosis [Bacon et al. 2014; Delaere and Van Raemdonck, 2016].
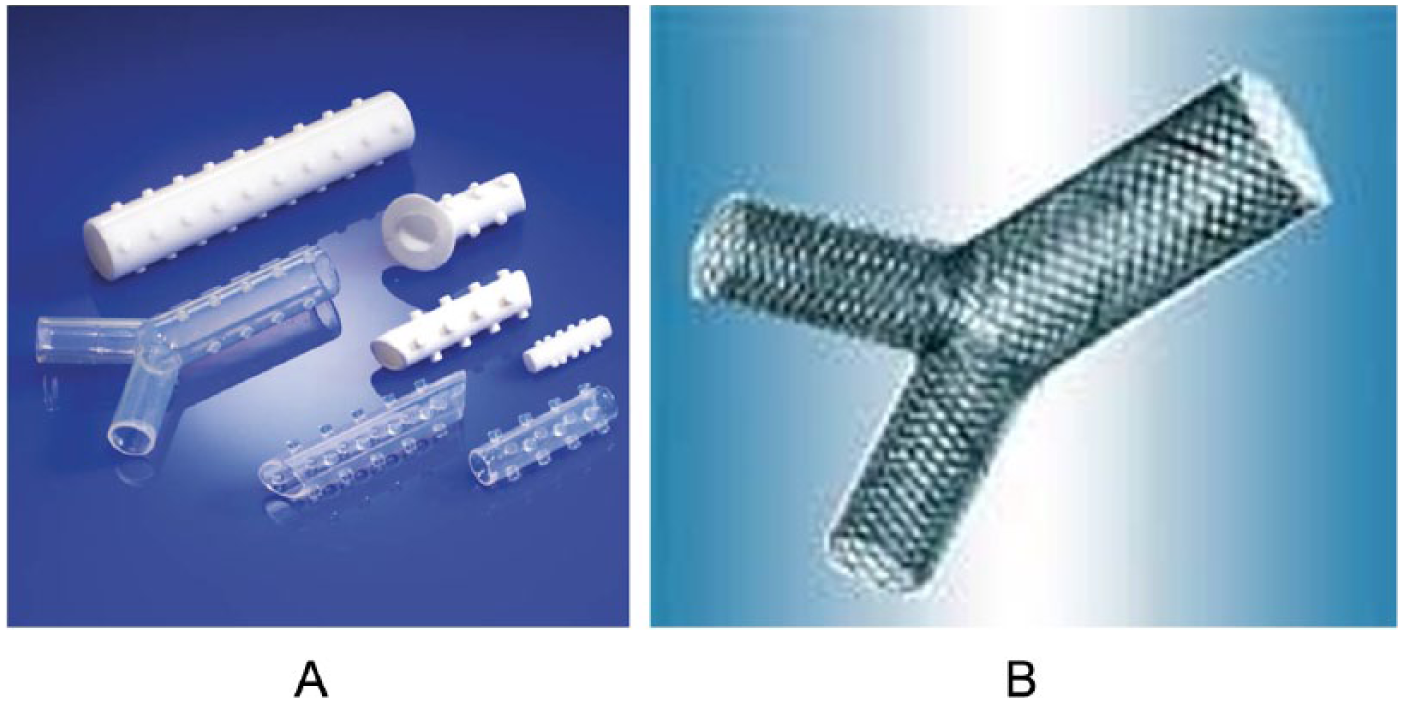
Current commercially available tracheal stents.
Physiological roles of NO include elimination of bacteria that develops in various surgically implanted devices [Halpenny and Mascharak, 2010]. Therefore, any airway implants encapsulated with NO may not only have its intended effect of vasodilation, for example, in a patient with PPHN, but also a secondary effect of reducing infection. Bioabsorbable stents would also address the issues of local, controlled and potentially ‘pulsed’ delivery as NO-incorporated material can be modified to release NO on physiological cues.
The development of a biodegradable NO-releasing stent for the trachea, placed well above the carina to avoid irritation, could result in adequate NO release over time which would circumvent the need for prolonged hospital stay and mechanical ventilation associated with iNO (Figure 5). NO-releasing biodegradable polymers do exist and have been patented, and can be used for in situ controlled-release delivery of additional bioactive agents [Cheng et al. 2006]. Although they have not been tested in the airway, the design of an appropriate biodegradable stent to be placed in the airways is an exciting and novel concept. Such implants can be combined with suitable vasodilators such as prostaglandins (e.g. iloprost) or prostacyclin analogues with a longer half-life (e.g. treprostinil) to prevent potential withdrawal symptoms that are shown to be associated with NO [Dzierba et al. 2014]. Phosphodiesterase (PDE) causes catabolism of cGMP and thus limits NO-induced vasodilation. Therefore, PDE inhibitors such as sildenafil may augment iNO effects, particularly in patients with prolonged hyperoxic ventilation, as this stimulates PDE activity. It may also prevent rebound pulmonary hypertension after weaning of iNO [Lakshminrusimha, 2012].
Nitric oxide (NO)-releasing implant in the trachea for paediatric respiratory diseases.
Summary and outlook
NO is one of the most researched molecules to restore cardiovascular homeostasis and has led to it been exploited to develop therapeutic treatment in the clinical setting. One of the notable properties of this molecule has been its role in selective pulmonary vasodilatation and in treatment of respiratory airway diseases such as PPHN. PPHN patients traditionally had poor prognosis and were difficult to treat. The use of ECMO was the standard treatment and provided cardiovascular support but does not seem to address the underlying problem of the disease. However, low doses of NO have been shown to allow postnatal adaptation at birth via pulmonary vasodilatation. iNO is now a widely established therapeutic mode of treatment to improve pulmonary haemodynamics, improve oxygenation and symptoms. However, iNO must be currently administered with mechanical ventilation, and it has been found to lead to secondary complications as well as being an expensive mode of treatment. Current research and development in NO has progressed to present a range of novel methods of controlled NO-delivery systems. The addition of NO-independent activators and stimulators, or drugs such as prostaglandins, to work in synergy with NO donors may be beneficial. It is of interest to consider such delivery methods within the respiratory system, where controlled release of NO can be introduced whilst minimizing the production of harmful byproducts. The exploitation of the state-of-the-art smart methods of direct delivery of NO could minimize the chance for reaction with oxygen and reduce infection. The ultimate goal would be to reduce the hospital inpatient time to receive iNO, and instead, following the introduction of the NO-eluting respiratory implant, the patient could be followed up serially to measure metHb levels, expired NO concentrations and monitor oxygenation levels with arterial blood gas. With improved understanding of encapsulation methods of NO for the broncho-tracheal system, physiological-release profile of NO in the pulmonary vasculature, and delivery methods, we envisage this perspective would prompt active investigation of their potential clinical benefit.
Footnotes
Acknowledgements
The authors would like to acknowledge Professors Martin Elliott and George Hamilton for their supportive comments, and Dr Luke Hale for creating the original Figure 5 of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.