
Abstract
Cardiovascular disease is the leading cause of mortality and morbidity following renal transplantation (RT), accounting for 40–50% of all deaths. After renal transplantation, an adverse cardiovascular event occurs in nearly 40% of patients; given the dialysis vintage and the average wait time, the likelihood of receiving coronary revascularization is very high. There is a significant gap in the literature in terms of the outcomes of prophylactic coronary revascularization in renal transplantation candidates. Current guidelines on myocardial revascularization stipulate that renal transplant patients with significant coronary artery disease (CAD) should not be excluded from the potential benefit of revascularization. Compared with percutaneous coronary intervention (PCI), however, coronary artery bypass grafting is associated with higher early and 30-day mortality. About one-third of renal transplant patients with CAD have to be treated invasively and so PCI is currently the most popular mode of revascularization in these fragile and compromised patients. A newer generation drug-eluting stent (DES) should be preferred over a bare metal stent (BMS) because of its lower risk of restenosis and improved safety concerns (stent thrombosis) compared with first generation DES and BMS. Among DES, despite no significant differences being reported in terms of efficacy, the newer everolimus and zotarolimus eluting stents should be preferred given the possibility of discontinuing, if necessary, dual antiplatelet therapy before 12 months. Since there is a lack of randomized controlled trials, the current guidelines are inadequate to provide a specifically tailored antiplatelet therapeutic approach for renal transplant patients. At present, clopidogrel is the most used agent, confirming its central role in the therapeutic management of renal transplant patients undergoing PCI. While progress in malignancy-related mortality seems a more distant target, a slow but steady reduction in cardiovascular deaths, improving pharmacological and interventional therapy, is nowadays an achievable medium-term target in renal transplant patients.
Keywords
Introduction
Cardiovascular disease is the leading cause of mortality and morbidity following renal transplantation, accounting for 40–50% of all deaths. Although the survival and quality of life of patients who undergo renal transplantation has improved considerably in past decades, life expectancy beyond 10 years is worse than in the general population, though higher than hemodialysis patients placed on the transplant waiting list [Wolfe et al. 1999; Ojo et al. 2000; US Renal Data System, 2007].
In a 3 years’ follow up after renal transplantation, an adverse cardiovascular event occurs in nearly 40% of patients. Congestive heart failure is the more common cardiovascular event, though in the elderly and among diabetics, larger represented subgroups, acute myocardial infarction is predominant [Arend et al. 1997; Coresh et al. 2007].
After transplantation, the preexisting cardiovascular risk factors are accompanied by transplant-related risk factors such as allograft dysfunction and/or unintended effects of immunosuppression [Boots et al. 2004]. The occurrence of allograft dysfunction, especially when associated with proteinuria, can contribute to the development or worsening of coronary artery disease (CAD) [Fernandez-Fresnedo et al. 2002]. Death with a functioning graft is a major reason for graft loss particularly after the first post-transplantation year. Given the leading role of CAD, pharmacological and percutaneous strategies have become an important issue in this high-risk subset of end stage renal disease (ESRD). Since research on percutaneous coronary intervention (PCI) and antiplatelet therapy in kidney transplant recipients is lacking, as hemodialysis patients are excluded from randomized clinical trials (RCTs), cardiovascular assessment and treatment are largely based on data from chronic kidney disease (CKD) or ESRD (when available) or, more frequently, from the general population.
Method
The scope of this review is to provide an overview of the current evidence on the use of myocardial revascularization and antiplatelet agent in transplant recipient patients, its current and potential use, reviewing the indications, the safety and the efficacy data. The starting point was the current guidelines on myocardial revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS), the American Heart Association (AHA)/American College of Cardiology (ACC) guidelines for the management of patients with non-ST-elevation acute coronary syndromes and the US Renal Data System. A systematic search on MEDLINE, EMBASE and the Cochrane Central Register of Controlled Trials was then performed. Details of RCTs, observational studies, case series, systematic reviews and expert opinions were collected, analyzed and discussed.
Diagnostic approaches
Initial screening and diagnostic confirmation
Given the dialysis vintage of patients and that the average waiting time for renal transplantation is about 4–6 years, the likelihood of receiving a coronary revascularization is very high. Due to the combined risk of ischemic and bleeding complications, the screening of potential candidates for myocardial revascularization with an established net clinical benefit is crucial. Specifically tailored strategies aimed at screening transplant recipient candidates have been proposed worldwide.
The 2005 National Kidney Foundation Kidney Disease Outcomes Quality Initiative guidelines for CAD recommend a cautious approach for renal transplant candidates based on a cardiac stress test: annually in diabetics; every 2 years in those with coronary or peripheral vascular disease; and every 3 years for others [K/DOQI Workgroup, 2005]. The European Best Practice Guideline (ERBP) on the management and evaluation of the kidney donor and recipient [European Renal Best Practice Transplantation Guideline Development Group, 2013] stresses the need to screen asymptomatic high risk patients (older age, diabetic, history of CAD) only with a noninvasive test. Further cardiac investigation with noninvasive stress imaging should be performed only in cases of a positive or inconclusive exercise tolerance test. However, all these recommendations are still evidence level C, while coronary angiography is level D (namely, expert opinion), so the decision to perform angiography and possible revascularization should be made by the heart team including an interventional cardiologist and a cardiac surgeon. The Kidney Health Australia (KHA)/Caring for Australians with Renal Impairment (CARI) guideline on recipient assessment for transplantation [Campbell et al. 2013] broadens the high risk features for cardiovascular screening (older age, diabetes, abnormal echocardiogram, previous ischemic heart disease or congestive heart failure, long duration of dialysis, and smoking status), recommending coronary angiography only in cases with a positive screening test and suggesting that the benefit of revascularization before transplantation should be reviewed on an individual basis.
Available treatments
There is a significant gap in the literature in terms of outcomes of prophylactic coronary revascularization in renal transplant candidates. Especially during acute coronary syndrome (ACS), observational studies have shown better short- and long-term survival in patients with multivessel disease undergoing revascularization than those who received medical therapy alone [Chertow et al. 2004; Hemmelgarn et al. 2004; Reddan et al. 2003]. However, hemodialysis patients, having an increased risk of periprocedural ischemic and bleeding complications, are frequently excluded from most RCTs on revascularization and hence current treatment strategies are based on retrospective analyses of RCTs and on registry data.
In 1992, the results of an RCT published in The Lancet showed that revascularization decreased the frequency of cardiac events in diabetic patients with CKD and symptomless coronary artery stenosis, suggesting that all diabetic candidates for renal transplantation should be screened for silent ischemia [Manske et al. 1992]. Several observational studies have reported outcomes after coronary revascularization in selected cohorts of potential renal transplant candidates from nonsignificant, through survival benefit only in patients with 3-vessel CAD, to excellent survival in transplant recipients who received preemptive revascularization [Herzog et al. 2004; Kumar et al. 2011; Garcia et al. 2008]. However, Patel and colleagues found no apparent survival difference after transplantation between patients who underwent PCI or coronary artery bypass surgery (CABG) compared with those who underwent angiography alone or no angiography, suggesting that cardiac testing represented a barrier to being placed on the waiting list [Patel et al. 2008]. Current guidelines on myocardial revascularization stipulate that renal transplant recipients with significant CAD should not be excluded from the potential benefit of myocardial revascularization [Windecker et al. 2014].
Type of myocardial revascularization
The type of coronary revascularization in patients with ESRD is still controversial. In the overall ESRD population, the results from US Renal Data System (covering 21,981 patients) suggest that CABG should be preferred over PCI but only for multivessel coronary disease and in appropriately selected non-ACS patients [Chang et al. 2012]. Moreover, no difference between CABG and PCI was found in 2272 renal transplant recipients from the US Renal Data System between 1997 and 2009 in terms of survival or the composite of death and myocardial infarction [Lenihan et al. 2013]. Herzog and colleagues had previously confirmed these data, reporting superior 1 month unadjusted survival after revascularization in hemodialysis patients who received drug-eluting stents (DES) compared with CABG (first generation DES = 69.7% versus CABG = 66.6%) or PCI with bare metal stents (BMS) (BMS = 3.6%). However, unadjusted 36 months’ survival favored CABG over DES (42.0% versus 38.1%), especially among patients receiving an arterial graft [Herzog et al. 2008]. A recent meta-analysis confirmed the effectiveness of the PCI strategy in lowering short-term mortality and the superiority of CABG for long-term target vessel revascularization reduction but with similar long term mortality [Ren et al. 2014].
In renal transplant recipients, the absolute rate of return to permanent dialysis after CABG is not negligible (about 20%) and was similar after on-pump and off-pump revascularization [Shayan et al. 2011]. Conversely a lower rate of about 6% of PCI-related contrast-induced nephropathy has been recently reported [Haider et al. 2015]. However, compared with PCI, CABG is associated with higher early and 30-day mortality. Considering that about one-third of renal transplant patients with CAD have to be treated invasively, PCI is therefore currently the most popular mode of revascularization.
To date, no definitive conclusions can be drawn on the best type of coronary revascularization principally because a head-to-head randomized comparison is lacking. However, the ESC guidelines on myocardial revascularization for ESRD stress the importance of the selection of the most appropriate revascularization strategy taking into account the general condition and life expectancy, the least invasive approach being more appropriate in the most fragile and compromised patients [Windecker et al. 2014]. This suggests PCI as a more suitable coronary revascularization strategy.
Choice of coronary stent
Although PCI has significantly improved long-term survival in patients with CKD and ACS [Keeley et al. 2003], CKD represents an independent negative predictive factor of adverse events, regardless of the treatment strategy (CABG versus PCI, DES versus BMS). Compared with BMS, implantation of a first generation DES reduced the 1-year major adverse coronary events (MACE) rate (i.e. cardiac death, nonfatal myocardial infarction or target vessel revascularization) [Jeong et al. 2008]. Approximately 25% (1108) of patients with CKD enrolled on the US National Heart, Lung, and Blood Institute (NHLBI) Dynamic Registry had A higher incidence of myocardial infarction and mortality, and the use of DES did not reduce the incidence of target lesion revascularization compared with BMS [Green et al. 2011]. Conversely in the multicenter BASKET-PROVE trial, a lower rate of MACE was found with DES use compared with BMS use [Wanitschek et al. 2013]. In the Guthrie PCI Registry, 436 patients with CKD treated with DES had a lower risk of all-cause death, target vessel revascularization and MACE with a similar risk of myocardial infarction and stent thrombosis compared with BMS [Shenoy et al. 2010]. Among CKD patients, the hemodialysis subgroup experienced higher in-segment restenosis rate and a higher MACE rate, principally driven by higher mortality and target lesion revascularization after sirolimus eluting stent implantation [Ota et al. 2009]. Also coronary stent thrombosis (definite or probable) appeared negatively influenced by the presence of CKD (1.8% in CKD patients versus 0.,6% in non-CKD patients, p = 0.014) in patients undergoing PCI with DES but specifically after first generation DES implantation [Miao et al. 2012].
In a retrospective analysis, first and second generation DES (320 and 128 patients, respectively) showed a similar safety and efficacy profile in CKD patients for the outcomes of deaths, repeat revascularization and MACE [Chan et al. 2014]. A Korean registry found a similar risk of 12-month MACE in ST segment elevation myocardial infarction (STEMI) patients with CKD undergoing primary PCI with different type of stents, although the incidence of 12-month all-cause death was higher in the BMS group than in the everolimus eluting stent group (p = 0.002) [Ahmed et al. 2012].
In conclusion, when PCI is indicated, newer generation DES (Class I level of evidence B) [Windecker et al. 2014] should be preferred over BMS because of its lower risk of restenosis and improved safety concerns (stent thrombosis) compared with first generation DES and BMS [Sood et al. 2013; Saltzman et al. 2011]. Among DES, despite no significant differences being reported in MACE and target lesion revascularization [Kamoi et al. 2013; Sardi et al. 2014], the newer everolimus and zotarolimus eluting stent should be preferred because of the lower rates of stent thrombosis and given the possibility of discontinuing, if necessary, dual antiplatelet therapy (DAPT) before 12 months [Valgimigli et al. 2013; Silber et al. 2014]. Table 1 summarizes device characteristics, and the indication and potential use of currently available stents in hemodialysis patients.
Device characteristics, indication and potential use of currently available stent in hemodialysis.

CE mark (European Commission product conformity mark).
HD, hemodialysis; DAPT, dual antiplatelet therapy; RCT, randomized clinical trial.
Antiplatelet therapy
DAPT is the cornerstone treatment after stent implantation. In renal transplant patients, the clinical setting is also the principal determinant of the type, onset, combination and duration of antiplatelet therapy (Table 2).
Evidence, duration of dual antiplatelet therapy (DAPT) and type of antiplatelet related to clinical setting.

150–300 mg oral loading dose in treatment-naïve patients, followed by 75–100 mg daily.
150–300 mg oral loading dose or 80–150 mg i.v. in treatment-naïve patients, followed by 75–100mg daily.
300 mg loading dose, if the procedure is performed from 3 to 6 hours after load, or 600 mg loading dose, if performed before 3 hours after load, followed by 75 mg daily [Silber et al. 2005], [Bellemain-Appaix et al. 2010], [Windecker et al. 2014].
600 mg loading dose, followed by 75 mg daily [Amsterdam et al. 2014].
600 mg loading dose, followed by 75 mg daily [Windecker et al. 2014].
60 mg p.o. loading dose; 10 mg maintenance dose [Windecker et al. 2014].
180 mg p.o. loading dose; 90 mg maintenance dose b.i.d. [Amsterdam et al. 2014].
180 mg p.o. loading dose; 90 mg maintenance dose b.i.d. [Windecker et al. 2014].
ASA, acetylsalicylic acid; b.i.d., twice daily; BMS, bare metal stent; DES, drug-eluting stent; i.v., intravenously; NSTEMI, non-ST segment elevation myocardial infarction; p.o., by mouth; STEMI; ST segment elevation myocardial infarction.
Since RCTs are lacking, the current guidelines on percutaneous coronary revascularization are inadequate to provide a specifically tailored antiplatelet therapeutic approach for patients undergoing renal transplantation. Although many differences have been found principally related to comorbidities and bleeding, the recommendations for the general population have very often been translated to ESRD. ESRD both influences platelet function and coagulation cascade, resulting together in hemorrhagic tendencies and a prothrombotic state. An abnormal platelet function seems to play a pivotal role in bleeding complications principally related to defective subendothelial adhesion, mediated either by impaired expression of membrane glycoprotein receptor or by intrinsic defects in the synthesis, storage and release of platelets mediators. In addition, immunosuppressive therapy by itself can increase bleeding risk. Moreover, uremic platelets show enhanced procoagulant activity [Moal et al. 2003; Bonomini et al. 2004; Kaw and Malhotra, 2006] and platelet-derived microparticles [Ando et al. 2002], exerting a procoagulant activity by overexpressed membrane receptors for factor Va that accelerate thrombin generation.
In addition, an increased risk of site and non-site access-related bleeding complications is reported. Considering the impact of bleeding on adverse outcome after PCI [Rao et al. 2005; Eikelboom et al. 2006; Ndrepepa et al. 2008; Mehran et al. 2009; Romagnoli et al. 2012; Summaria et al. 2012], the safety/efficacy balance of antiplatelet therapy affects the poor prognosis, contributing to explaining the general underutilization of antithrombotic medications.
Aspirin therapy has been found to be beneficial after acute coronary syndromes (ACS) and/or myocardial revascularization in all spectrum of renal dysfunction [Wright et al. 2002]. In renal transplant recipients in a single retrospective study, a multivariate analysis also found that aspirin therapy is associated with improved allograft function and survival [Grotz et al. 2004]. Despite current guidelines which recommend the use of aspirin for primary and secondary prevention of CAD, diabetes or other high risk factors for CVD [Kasiske et al. 2000], it remains to be proven whether all renal transplant recipients should take aspirin. As bleeding hazards might be increased, aspirin and other antiplatelet agents should be used cautiously in a stable setting with low annual risks of cardiovascular events and a medically-alone managed conservative strategy. Nevertheless, when an ischemia driven coronary intervention is performed, DAPT is strongly recommended to avoid stent thrombosis and adverse coronary events. Considering the linear correlation between higher dose and bleeding risk [Matsumoto et al. 2003], when indicated, a daily longlife maintenance dose of aspirin of 75–100 mg/day seems to be the safer option.
Among P2Y12 receptor inhibitors, clopidogrel, a second generation oral thienopyridine, is a pro-drug converted into active metabolites through a two-step reaction involving cytochrome P450 enzymes, leading to an irreversible blockade of the P2Y12 receptor. Compared with prasugrel and ticagrelor, this conversion results in a slower onset of action and a larger variability in bioavailability.
Prasugrel is a third generation oral thienopyridine that is a specific, irreversible antagonist of the platelet adenosine 5′-diphosphate P2Y12 receptor, with more potent antiplatelet activity, faster onset of action, and less interpatient variability compared with clopidogrel. In ESRD, exposure to the active metabolite of prasugrel is lower than in healthy controls, but this does not affect platelet aggregation [Small et al. 2009]. Hence during prasugrel therapy, a dose adjustment based on renal function is not recommended but the drug label reminded the limited experience in stage 5 CKD considering that a subgroup analysis of TRITON -TIMI 38 trial could be performed only for patients until stage 3 to 4 CKD [Montalescot et al. 2009].
Ticagrelor is a cyclopentyltriazolopyrimidine, with a plasma halflife of approximately 6–12 hours, and unlike clopidogrel and prasugrel, requires dual daily administration and binds reversibly to the P2Y12 receptor. Ticagrelor is metabolized minimally from the kidneys. Its effectiveness in ACS was tested in the PLATO trial in which the CKD subgroup is well represented, consisting of almost 21% of the overall study population [James et al. 2010]. Similarly to clopidogrel and prasugrel, ticagrelor requires no dose adjustment based on renal function, but its use in patients with ESRD is not recommended because of the lack of data in this specific subpopulation.
Choice of therapy
Stable CAD
In a stable clinical setting, DAPT includes an oral loading dose of acetylsalicylic acid (ASA) plus clopidogrel (Table 2). Despite newer, more potent, P2Y12-receptor antagonists being available, as stated in the guidelines, only clopidogrel is recommended in the stable non-ACS clinical setting. After PCI with stent implantation, a single antiplatelet therapy with ASA is followed lifelong after the first month (if BMS are used) or after the sixth month (if new generation DES are used) [Silber et al. 2005].
ACS
In ACS, renal function is significantly correlated with MACE. Compared with patients with normal function, hemodialysis patients have a 30 and 10 times higher inhospital mortality during STEMI and non-ST segment elevation myocardial infarction (NSTEMI), respectively. This worse clinical outcome seems to be related to different mechanisms: (a) more severe coronary involvement; (b) a higher comorbidity rate; (c) underutilization of cardiac medication with possible and/or suspected suboptimal response; (d) disease and/or drug related excessive bleeding; and (e) a high risk of restenosis and stent thrombosis.
The American National Kidney Foundation Guidelines state that all hemodialysis patients with ACS should be managed in the same way as nonhemodialysis patients, including use of DAPT and PCI. To balance the efficacy/safety ratio, a systematic approach based on an individual integrated ischemic and bleeding risk assessment should be used in all ACS patients undergoing PCI in order to individualize DAPT and to guide the time of revascularization. Many risk calculators have been proposed but, at present, none are specifically calibrated for hemodialysis patients.
NSTEMI
In hemodialysis patients, there is less consensus on the management of NSTEMI than for STEMI and stable angina. The 2014 ACC/AHA guidelines on the management of NSTEMI provide no specific recommendations for antiplatelet use in hemodialysis patients [Amsterdam et al. 2014]. The main reason of this gap must be sought in the wider spectrum of risk along with different timing and type of revascularization.
In particular, the guidelines stipulate that, in addition to aspirin, clopidogrel and ticagrelor (Class I level of evidence B) are the first treatment choice in the general population [Amsterdam et al. 2014].
Principally related to bleeding concerns with unfavorable net clinical benefit, prasugrel is not recommended for ‘upfront’ therapy in patients with NSTEMI on the basis of the TRITON study design and the results of TRILOGY-ACS and ACCOAST studies.
In the PLATO trial, patients with moderate- to-high-risk NSTEMI undergoing PCI had significantly lower primary endpoint occurrence with ticagrelor than with clopidogrel (11.4% versus 13.9%). The rate of thrombolysis in myocardial infarction (TIMI) major non-CABG-related bleeding was higher in the ticagrelor (2.8%) group than in the clopidogrel group (2.2%), but TIMI major CABG-related bleeding was less frequent than with clopidogrel. There was no difference in the overall rates of fatal hemorrhage despite a higher rate of fatal intracranial hemorrhage in the ticagrelor group (0.1% versus 0.001%; p <0.02).
In the CURRENT-OASIS 7 trial, a double-dose regimen of clopidogrel (600 mg loading dose followed by 150 mg daily dose for 7 days, then 75 mg daily) conferred similar MACE results than the standard dose at the cost of increased TIMI major bleedings and the need for blood transfusion, resulting in a negative way especially with the high risk of bleeding in hemodialysis patients [Mehta et al. 2010].
STEMI
Due to the increased hemorrhagic risk associated with thrombolysis, primary PCI should be considered the preferred reperfusion therapy in hemodialysis patients. Patients undergoing primary PCI should receive a combination of ASA and a P2Y12 receptor blocker as early as possible.
Oral or intravenous (i.v.) loading dose of ASA should be associated with the preferred P2Y12 inhibitors, prasugrel or ticagrelor (Table 2) [Wallentin et al. 2009; Wiviott et al. 2007] because of the more rapid onset of action and greater potency and superiority to clopidogrel in large outcome trials (Class I level of evidence B) [Montalescot et al. 2009; Steg et al. 2010; Bellemain-Appaix et al. 2010]. Clopidogrel should be used preferably when prasugrel or ticagrelor are either not available or contraindicated (Class I level of evidence C).
In the prespecified subgroups of patients with STEMI undergoing PCI in the TRITON–TIMI38 trial, the benefit of prasugrel was consistent for the primary endpoint (prasugrel 10.0% versus clopidogrel 12.4%; HR 0.79; 95% CI 0.65–0.97; p = 0.02), without a significant increase in non-CABG related bleeding risk (2.4% versus 2.1%; HR 1.11; 95% CI 0.70–1.77; p = 0.65). There was a lower risk of stent thrombosis (1.6% versus 2.8%; HR 0.58; 95% CI 0.36–0.93; p = 0.02), as well as of cardiovascular mortality [Montalescot et al. 2009] in favor of prasugrel at 30-day and 15-month follow up (2.4% versus 3.4%; HR 0.74; 95% CI 0.50–1.09; p = 0.129).
In the subset of patients with STEMI randomized in the PLATO trial, the benefit of ticagrelor over clopidogrel for the primary endpoint (9.4% versus 10.8%; HR 0.87) [Steg et al. 2010] was consistent with the overall results, without increased bleeding (TIMI non-CABG major bleedings 2.5% versus 2.2%; HR 1.09; 95% CI 0.80–1.48; p = 0.60) but with a trend towards a lower risk of cardiovascular mortality at 1 year. In a pooled analysis of 48,599 patients, of whom 94% presented with ACS and 84% had PCI, prasugrel and ticagrelor have been associated with a lower mortality and no significant excess of major bleeding among STEMI patients [Bellemain-Appaix et al. 2010].
Summary
Table 3 summarizes the recommendations for clinical practice.
Pros and cons of different antiplatelet agents.
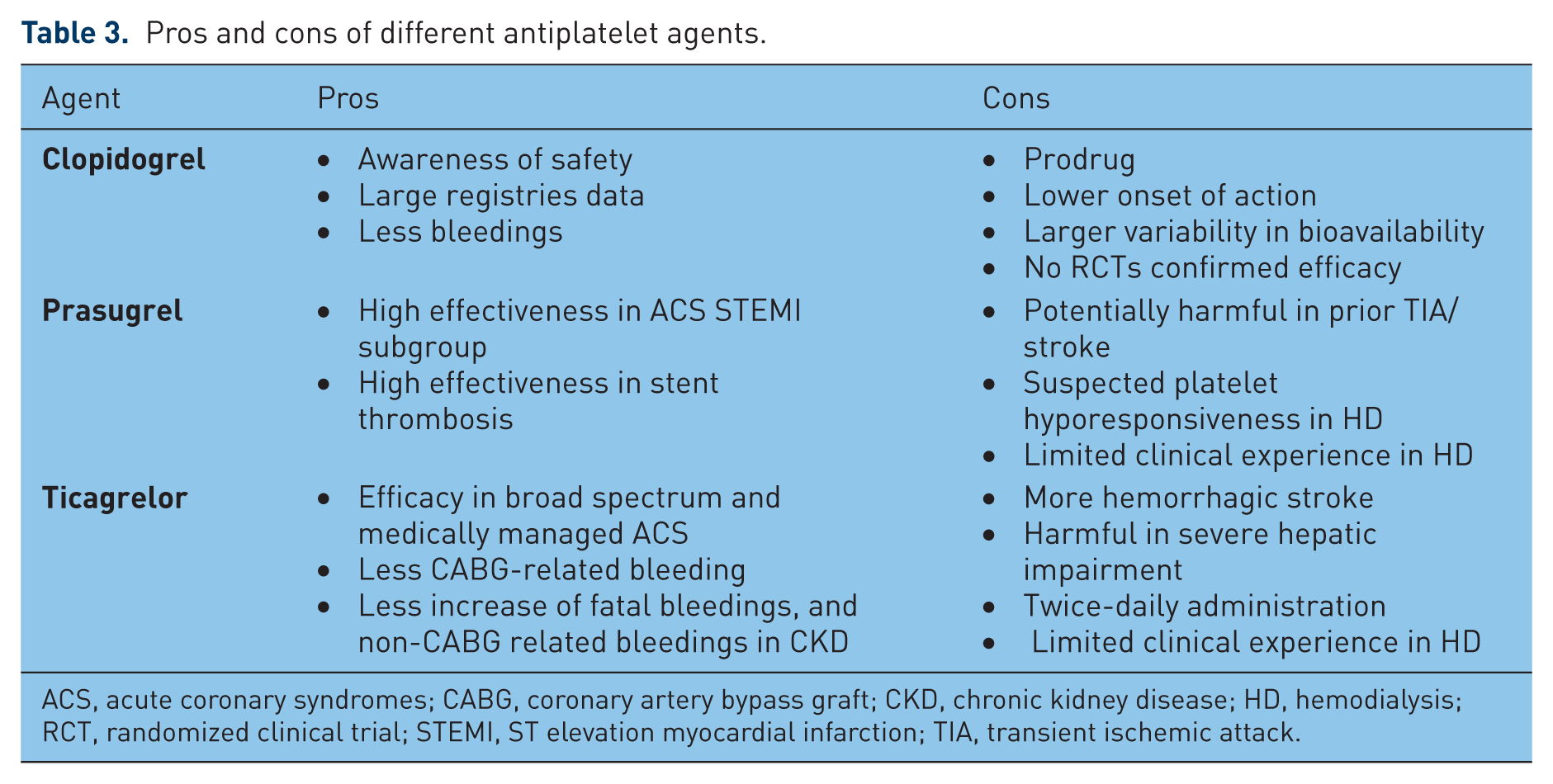
ACS, acute coronary syndromes; CABG, coronary artery bypass graft; CKD, chronic kidney disease; HD, hemodialysis; RCT, randomized clinical trial; STEMI, ST elevation myocardial infarction; TIA, transient ischemic attack.
If after initial screening a diagnostic confirmation of myocardial ischemia is documented, a coronary revascularization should be performed: the least invasive approach being more appropriate in the most fragile and compromised patients.
When PCI is indicated, a newer generation DES should be preferred over BMS because of its lower risk of restenosis and improved safety compared with first generation DES and BMS. The newer everolimus and zotarolimus eluting stents should be preferred for their lower rates of stent thrombosis and for the possibility of discontinuing, if necessary, DAPT before 12 months.
Aspirin should be administered at low-dose regimen longlife after coronary stenting.
Clopidogrel remains the only choice in case of PCI in a stable clinical setting and, regardless of clinical setting, in patients requiring P2Y12-inhibiting therapy with a basal high risk of bleeding (included patients taking oral anticoagulant therapy).
Prasugrel, even if not recommended, should be considered only in STEMI undergoing primary PCI with an individual ischemic risk and/or thrombotic burden higher than the bleeding risk (i.e. diabetic, STEMI, stent thrombosis during clopidogrel treatment). It should be used with caution in patients with low body weight and in the elderly (>75 years). It is contraindicated in patients with a prior transient ischemic attack/stroke or previous intracranial hemorrhage.
Ticagrelor should be considered carefully in patients with poor compliance given its twice-daily administration. It is contraindicated in patients with prior hemorrhagic stroke and severe hepatic impairment, and should be used cautiously in patients treated with potent inhibitors or inducers of CYP3A due to potential drug interactions.
Conclusion
In the past decade the gradual decline in cardiovascular mortality in hemodialysis patients is principally due to 30-day reduced mortality for STEMI, related either to the large use of antiplatelet agents and statin [Summaria et al. 2011] or to the increased use of coronary revascularization.
Despite its widespread use, no information derived from RCTs is available for clopidogrel in transplant recipient patients. However, due to the great experience accrued in routine clinical practice, the awareness of safety is higher for clopidogrel than for prasugrel or ticagrelor [Chang et al. 2014]. Hence clopidogrel, despite its limitations, plays a central role in the therapeutic management of transplant recipient patients undergoing PCI.
While progress in the malignancy-related mortality seems a more distant target, a slow but steady reduction in cardiovascular deaths, improving pharmacological and interventional therapy, is nowadays an achievable medium-term target in transplant recipient patients.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.