
Abstract
Objective
This meta-analysis was performed to evaluate the optimal discontinuation of dual antiplatelet therapy (DAPT) after drug-eluting stent (DES) implantation in acute coronary syndrome (ACS) patients.
Methods
A systematic search was conducted without language restrictions using PubMed, the Cochrane Library, and Clinical Trials.gov from January 2008 to July 2019. Studies that met the following criteria were included: (1) randomized trials that compared DAPT durations of <12 months (“short DAPT”) or ≥12 months (“long DAPT”); (2) studies that included data on patients with ACS; and (3) studies that included data on outcomes. The outcomes were pooled using the Mantel–Haenszel model, generating relative risk (RR) and 95% confidence intervals (CI). Statistical heterogeneity was evaluated using the Cochrane Q statistic P-value and I2 value. Publication bias was assessed by visually inspecting the funnel plots.
Results
Eight studies comprising 10,537 participants were included in the analysis. The primary endpoint was not different between short-term and long-term DAPT (RR, 1.11; 95% CI, 0.92–1.34).
Conclusion
A meta-analysis of the available evidence suggests that DAPT can be reduced to 3 or 6 months without increasing the risk of cardiovascular and cerebrovascular events in patients with ACS who are undergoing DES implantation.
Keywords
Introduction
Millions of patients worldwide with coronary artery disease receive percutaneous coronary intervention (PCI) yearly to treat ischemic events. 1 In contrast to bare metal stents, drug-eluting stents (DESs) have been shown to cause a remarkable reduction in repeated revascularization. 2 However, several observational studies have confirmed that the risk of death or myocardial infarction (MI) remains after DES implantation. 3 Dual antiplatelet therapy (DAPT), which is a P2Y12 inhibitor, has been perceived as a way to prevent thrombus formation. Current guidelines suggest that the DAPT duration in patients with stable coronary artery disease is 6 months or less. 4 ESC/EACTS Guidelines on Myocardial Revascularization 5 recommend that in patients with ACS who are treated with coronary stent implantation, DAPT with a P2Y12 inhibitor in addition to aspirin should be used for 12 months unless there are contraindications such as an excessive risk of bleeding. In patients with ACS and stent implantation who have a high risk of bleeding, discontinuation of P2Y12 inhibitor therapy after 6 months should be considered. The guidance is based on the conclusions of the SMART-DATE trial. 6 However, the optimal discontinuation of DAPT after DES implantation for ACS patients remains controversial.7–9
Methods
A systematic search was conducted without language restriction in PubMed, the Cochrane Library, and Clinical Trials.gov from January 2008 to July 2019. Search keywords were “dual antiplatelet therapy, drug-eluting stents.” These studies were included when the following criteria were met: (1) randomized trials that compared DAPT durations of <12 months (“short DAPT”) or ≥12 months (“long DAPT”); (2) studies that included data on patients with ACS; and (3) studies that included data on outcomes. The quality of the involved studies and assessment of trial bias risk were determined for the domains suggested by the Cochrane collaboration,10,11 emphasizing sequence generation, allocation concealment, blinding, outcomes assessment, and selectivity. The optimal time of dual antiplatelet therapy was determined by comparing the statistical differences based on the primary endpoint. The relative risk (RR) with 95% confidence interval (CI) for the outcome in each study was determined. Fixed- or random-effects models were with the Mantel–Haenszel method to incorporate the RR from the trials involved, when appropriate. A test of heterogeneity was conducted, and the Q statistic was acquired. The I2 index was used to summarize the proportion of the total variability in the estimates. Publication bias was assessed by visually inspecting the funnel plots. A two-tailed P ≤ 0.05 was considered to be statistically significant. Data were analyzed using Review Manager (RevMan) 5 (Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014).
Results
As shown in Figure 1, nine randomized controlled trials6,12–19 that comprised 10,537 enrolled patients were factored into the final analysis.10,11 The major characteristics of the included trials are presented in Table 1. All trials were rated as 5 to 7, or high quality studies, according to the Jadad score standard.
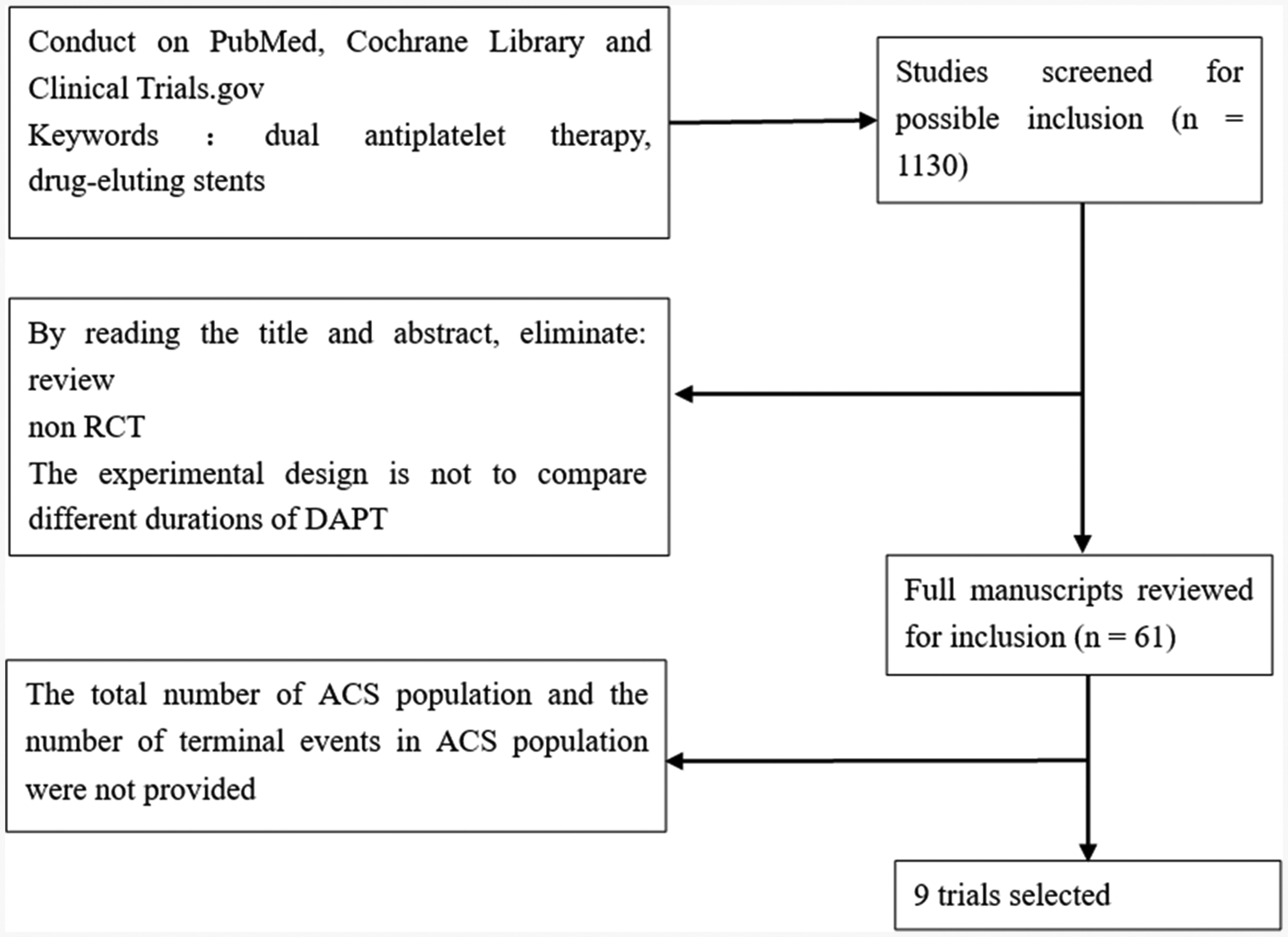
Study flow diagram.
Characteristics of included trials.

DES, drug eluting coronary stents; S-DAPT, dual antiplatelet therapy durations of <12 months; L-DAPT, dual antiplatelet therapy durations of ≥12 months; TVR, target vessel revascularization; PCI, percutaneous coronary intervention; MI, myocardial infarction; TIMI, thrombolysis in myocardial infarction.
All studies6,12–19 provided data for the primary endpoint. The test of heterogeneity indicated that the homogeneity was good. The RR was incorporated in the fixed-effects model. The visual inspection of the funnel plot did not indicate publication bias. The short-term and long-term DAPT were not different based on the primary endpoint (RR, 1.11; 95% CI, 0.92–1.34; Figure 2).

Meta-analysis results of the primary endpoint for patients with ACS.
The sensitivity analysis using the random-effects model yielded significantly similar results. The exclusion of any trial yielded similar results for the short-term DAPT group compared with the long-term DAPT group (Table 2).
Sensitivity analysis.

Given the different definition of the end event for each test, the greatest risk of double antiplatelet therapy was bleeding. 20 The increased risk of bleeding was associated with prolonged DAPT. 21 This may mask the benefits of dual antiplatelet therapy in reducing the incidence of redevelopment and cardiac infarction. Thus, a subgroup analysis was performed. The end event of subgroup 16,13,14 did not include bleeding events, while the end event of subgroup 212,15–19 included bleeding events. Neither subgroup 1 (RR, 1.07; 95% CI, 0.84–1.36) nor subgroup 2 (RR, 1.17; 95% CI, 0.87–1.57) was markedly different based on the primary endpoint (Table 3).
Subgroup analysis.

Each trial had a different definition for a short course of antiplatelet therapy, which might have affected the outcome. Two trials had a short-term DAPT of 3 months, while six other trials had a short-term DAPT of 6 months. A subgroup analysis was performed based on the short duration of antiplatelet therapy. Subgroup 318,19 had a 3-month short course of antiplatelet therapy, while subgroup 46,12–17 had a 6-month short course of antiplatelet therapy. Neither subgroup 3 (RR, 1.13; 95% CI, 0.76–1.68) nor subgroup 4 (RR, 1.10; 95% CI, 0.89–1.36) was significantly different based on the primary endpoint (Table 3).
Discussion
Currently, the optimal discontinuation of DAPT after DES implantation for ACS patients remains controversial.7,8 Most guidelines recommend that ACS patients with PCI should undergo postoperative double antiplatelet therapy for at least 1 year. 4 As indicated in the meta-analysis, the difference in endpoint events between ≤6-month DAPT and ≥12-month DAPT was not statistically significant. However, the increased risk of bleeding with DAPT remains controversial.20–22 This may mask the benefits of DAPT in reducing the incidence of redevelopment and cardiac infarction. 22 However, the meta-analysis revealed that the difference in endpoint events (prognosis and bleeding) between ≤6-month DAPT and ≥12-month DAPT was not statistically significant. It was also indicated by the subgroup analysis that both 6-month and 3-month DAPT were not markedly different compared with ≥12-month DAPT in terms of a statistical benefit. For ACS patients with drug-coated stent implantation, this can shorten the duration of DAPT for 6 months or even 3 months without increasing the risk of cardiovascular and cerebrovascular events in patients.
The meta-analyses performed by Bavishi 7 also had similar conclusions. However, the risk of cerebrovascular disease and shorter antiplatelet therapy sessions were not considered. Fewer tests were also conducted. The meta-analyses performed by Palmerini 9 also had similar conclusions. However, this article is a network meta-analysis. It is uncertain whether the results were obtained from a direct comparison or indirect comparison. The sample size of ACS patients and the credibility of the results are also uncertain.
The present meta-analysis had some limitations. The sample size was small, and the inclusion test did not describe the criteria for evaluating ACS patients. However, this study provides comprehensive evidence for a future study on DAPT in patients with ACS who are undergoing DES implantation. All involved trials were rated as high quality studies based on the Jadad score standard. The heterogeneity test revealed high homogeneity, and the sensitivity analysis and subgroup analysis revealed good stability. Thus, the meta-analysis was highly reliable.
Conclusion
Overall, the ≤6-month and ≥12-month DAPT were not different among patients with ACS based on the primary endpoint. DAPT could be reduced to 6 months or even 3 months without increasing the risk of cardiovascular and cerebrovascular events in patients with ACS who are undergoing DES implantation.