
Abstract
Background:
Acute coronary syndrome (ACS) continues to be a leading cause of morbidity and mortality worldwide. Galectin-3 and pentraxin-3 are two prognostic biomarkers that have been studied in heart failure (HF). However, there are limited data on these biomarkers in the ACS population. The objective of the study was to determine the variables that are most affected by high concentrations of pentraxin-3 and galectin-3, and the influence they have on outcomes of all-cause mortality in patients with ACS.
Methods:
We included a total of 160 patients [ST elevation myocardial infarction (STEMI),n = 64; non STEMI/unstable angina (NSTEMI/UA), n = 38; and control subjects with chronic stable angina (CSA)/microvascular angina (MVA) n = 58]. Plasma pentraxin-3 and galectin-3 levels were assessed from these patients at the time of hospital admission. Major adverse cardiovascular events including all-cause mortality, rehospitalizations and coronary artery bypass graft surgery (CABG) were assessed at 6 months.
Results:
The median concentration of pentraxin-3 and galectin-3 were significantly higher in STEMI than in NSTEMI patients (p < 0.005) or controls (p < 0.005). Greater numbers of deaths (4 versus 0) were observed in STEMI patients with higher levels of these biomarkers. In addition, ACS patients with high levels of pentraxin-3 and galectin-3 had lower left ventricular ejection fraction (LVEF) (p < 0.005), and a moderate correlation was observed between LVEF and pentraxin-3 levels (r = -0.45, p < 0.005). Patients with higher galectin-3 levels were also observed to have a lower estimated glomerular fraction rate (eGFR), and a moderate correlation was observed between them (r = -0.34, p < 0.005).
Conclusion:
Pentraxin-3 and galectin-3 hold much promise in the ACS population as prognostic biomarkers.
Keywords
Introduction
Acute coronary syndrome (ACS) remains a major public health problem causing significant morbidity and mortality. The spectrum of ACS includes ST segment elevation myocardial infarction (STEMI), non-ST segment elevation myocardial infarction (NSTEMI) and unstable angina (UA). They share common pathophysiological origins related to plaque vulnerability with or without luminal thrombosis and vasospasm. It has been estimated that about a third of STEMI patients die within 24 hours of onset, and 15% of the patients with UA/NSTEMI die or experience reinfarction 30 days post diagnosis. Once diagnosed with ACS, approximately 30% of the patients are rehospitalized within 6 months [Go et al. 2014]. Forecasts covering 10 years in the US, France, Germany, Italy, Spain, the UK and Japan observe that the incidence of hospitalized cases of ACS will increase from 1.29 million cases in 2012 to 1.43 million cases in 2022 at the rate of 1.04% per year [Market Research Reports, 2014]. In India, the mortality attributed to cardiovascular diseases (CVD) alone is expected to rise by 104% in men and 90% in women between 1985 and 2015 [Bulatao and Stephens, 1992]. The data from the CREATE (Treatment and outcomes of acute coronary syndromes in India) registry showed that the percentage of STEMI cases were significantly higher in the Indian population (61%) compared with the Western population (30–40%) despite them being 5–10 years younger [Xavier et al. 2008].
In 1998, the Biomarkers Definitions Working Group at the US National Institutes of Health defined a biomarker as ‘a characteristic that is objectively measured and evaluated as an indicator of normal biological processes, pathogenic processes, or pharmacologic responses to a therapeutic intervention’ [Biomarkers Definitions Working Group, 2001; Atkinson et al. 2001]. Cardiovascular biomarkers have been increasingly used in the past few years to facilitate the screening, diagnosis or prognosis of disease. For instance, troponins and creatine phosphokinases are indicative of the extent of myocardial damage. B-type natriuretic peptide (BNP) and N-terminal pro-brain natriuretic peptide (NT-pro BNP) have been approved by the US Food and Drug Administration (FDA) for the diagnosis and management of congestive heart failure (CHF). A number of biomarkers such as myeloperoxidase, metalloproteinase, soluble CD40 ligand, ischemia modified albumin, pregnancy-associated plasma protein-A, cystatin C, fatty acid binding protein, and placental growth factor (PlGF) are under investigation for diagnostic/prognostic use in different stages of ACS [Nagesh and Roy, 2010]. While a combination of biomarker results and standard testing aids the diagnosis of ACS, predicting the prognosis of ACS patients remains a challenge. Thus there is ample scope for developing biomarkers that can accurately predict cardiovascular outcomes.
Pentraxin-3 is an inflammatory biomarker from the C-reactive protein (CRP) family which has been shown to be expressed at the site of atherosclerotic plaques and cardiac myocytes [Kunes et al. 2012]. A significantly higher level of pentraxin-3 was found in ACS subjects than in healthy controls [Ustündağ et al. 2011]. Complementarily Matsui and colleagues found that a higher level of pentraxin-3 in their cohort of NSTEMI and UA patients efficiently predicted 6-month cardiac events of death or rehospitalization [Matsui et al. 2010].
Galectin-3 has been approved by the FDA as a prognostic biomarker in CHF to be used in conjunction with clinical evaluation [Yin et al. 2014]. Galectin-3 is a soluble β-galactoside binding lectin that mediates profibrotic pathways [Sharma et al. 2004]. A number of studies have evaluated the utility of galectin-3 in heart failure (HF) populations, but only a handful of studies have been conducted in ACS populations. Grandin and colleagues observed that, in patients with acute myocardial infarction (AMI), those with galectin-3 greater than median had a higher risk of new or recurrent HF [Grandin et al. 2012]. Tsai and colleagues found that patients with STEMI had higher circulating levels of galectin-3 than healthy controls, and STEMI patients with high galectin-3 levels experienced a greater rate of 30-day mortality [Tsai et al. 2012].
A number of studies have investigated the role of pentraxin-3 and galectin-3 in HF. However, there is a dearth of data in the ACS population, giving us the impetus to perform this study. We thus sought to determine the variables that are most affected by high concentrations of pentraxin-3 and galectin-3, and the influence they have on outcomes of all-cause mortality in ACS patients.
Methods
The study protocol was approved by the Institution Ethics Committee, SRM Medical College Hospital and Research Centre, Kancheepuram, and was conducted between April 2013 and June 2014. Written informed consent was obtained from all patients who participated in the study. We included a total of 160 patients, of whom 64 were diagnosed with STEMI, 38 with NSTEMI/UA, and 58 were control subjects with chronic stable angina (CSA)/microvascular angina (MVA). Patients with prior HF, severe valvular heart disease, coexisting cancers, connective tissue diseases and cirrhosis were excluded from the study. Demographic characteristics, clinical variables and patient history were obtained from patient interviews and medical records.
A total of 5ml of peripheral blood was collected in ethylenediamine tetraacetic acid (EDTA) coated Vacutainer tubes from each patient within 48 hours of admission to the cardiac intensive care unit (ICU). Plasma galectin-3 and pentraxin-3 levels were assessed using an enzyme linked immunosorbent assay (ELISA) (R&D Systems, USA). Patients were followed up at 6 months through telephonic interview by investigators blinded to the biomarker levels to assess major adverse cardiovascular events that include all-cause mortality, rehospitalizations and coronary artery bypass graft surgery (CABG).
Data were expressed as mean ± standard deviation (SD) or median with interquartile range (IQR). The differences in the patient characteristics between the three study groups were compared using one way analysis of variance (ANOVA) for continuous variables or Pearson’s chi-squared test for variables with frequency distribution. Pearson correlation was used to measure correlation between different variables. Data were log transformed when they did not follow a Gaussian distribution. A p value <0.05 was considered as statistically significant. Statistical analysis was performed using computer software programs such as Statistical Package for Social Scientists, SPSS version.16 (Chicago, IL, USA) and GraphPad Prism version 5.01 for Windows (San Diego, CA, USA).
Results
An ACS cohort consisting of patients with STEMI (n = 64), NSTEMI (n = 38) and non-ACS populations consisting of a small cohort of patients with CSA/MVA (n = 58) were compared for age, sex, body mass index (BMI), left ventricular ejection fraction (LVEF), estimated glomerular filtration rate (eGFR) and risk factors such as diabetes, hypertension and dyslipidemia. Family history of coronary artery disease (CAD) and their smoking status were also recorded and compared between the groups. Between the three groups, LVEF and smoking emerged as being significantly different (Table 1).
Baseline characteristics of study patients.

Data expressed as mean ± standard deviation, percentage or median with interquartile range. *p<0.05;**p<0.005; a compared to STEMI group;
ACS, acute coronary syndrome; BMI, body mass index, CAD, coronary artery disease, eGFR, estimated glomerular filtration rate, LVEF, left ventricular ejection fraction; NA, not applicable; NSTEMI, non-ST segment elevation myocardial infarction; STEMI: ST segment elevation myocardial infarction; UA: unstable angina.
Galectin-3, pentraxin-3 and LVEF
In the cohort of ACS patients, the cutoffs derived from receiver operating characteristic (ROC) curves for galectin-3 and pentraxin-3 were 11.02 ng/ml and 6.45 ng/ml, respectively. Patients were divided into two groups based on galectin-3 and pentraxin-3 levels greater and lesser than the cutoff (Table 2).
Comparison of ACS patient characteristics based on the cutoff derived from ROC curve of the biomarkers.

Data expressed as means ± standard deviation, percentage or median with interquartile range.
p < 0.05;**p < 0.005.
ACS, acute coronary syndrome; BMI, body mass index, CAD, coronary artery disease, eGFR, estimated glomerular filtration rate, LVEF, left ventricular ejection fraction; NSTEMI, non-ST segment elevation myocardial infarction; STEMI: ST segment elevation myocardial infarction; UA: unstable angina.
In patients that had biomarker levels greater than cutoff, LVEF was found to be significantly lower. However, in those that had greater pentraxin-3 levels, a higher percentage of these patients were found to be diabetic and hypertensive.
Consistent with the impact of galectin-3 and pentraxin-3 on LVEF, both the biomarkers were found to be negatively correlated with LVEF in ACS and myocardial infarction (MI) patients. In MI patients, both the biomarkers observed a significant association with ACS patients. In ACS patients, there was a weak association between galectin-3 and LVEF (r = -0.2392, p < 0.05), while a relatively stronger association was detected between pentraxin-3 and LVEF (r = -0.4539, p < 0.005). In the MI subcohort, a weak association between the biomarkers and LVEF was observed (galectin-3: r = -0.3483, p < 0.05, pentraxin-3:r = -0.3232, p < 0.05) (Figure 1).
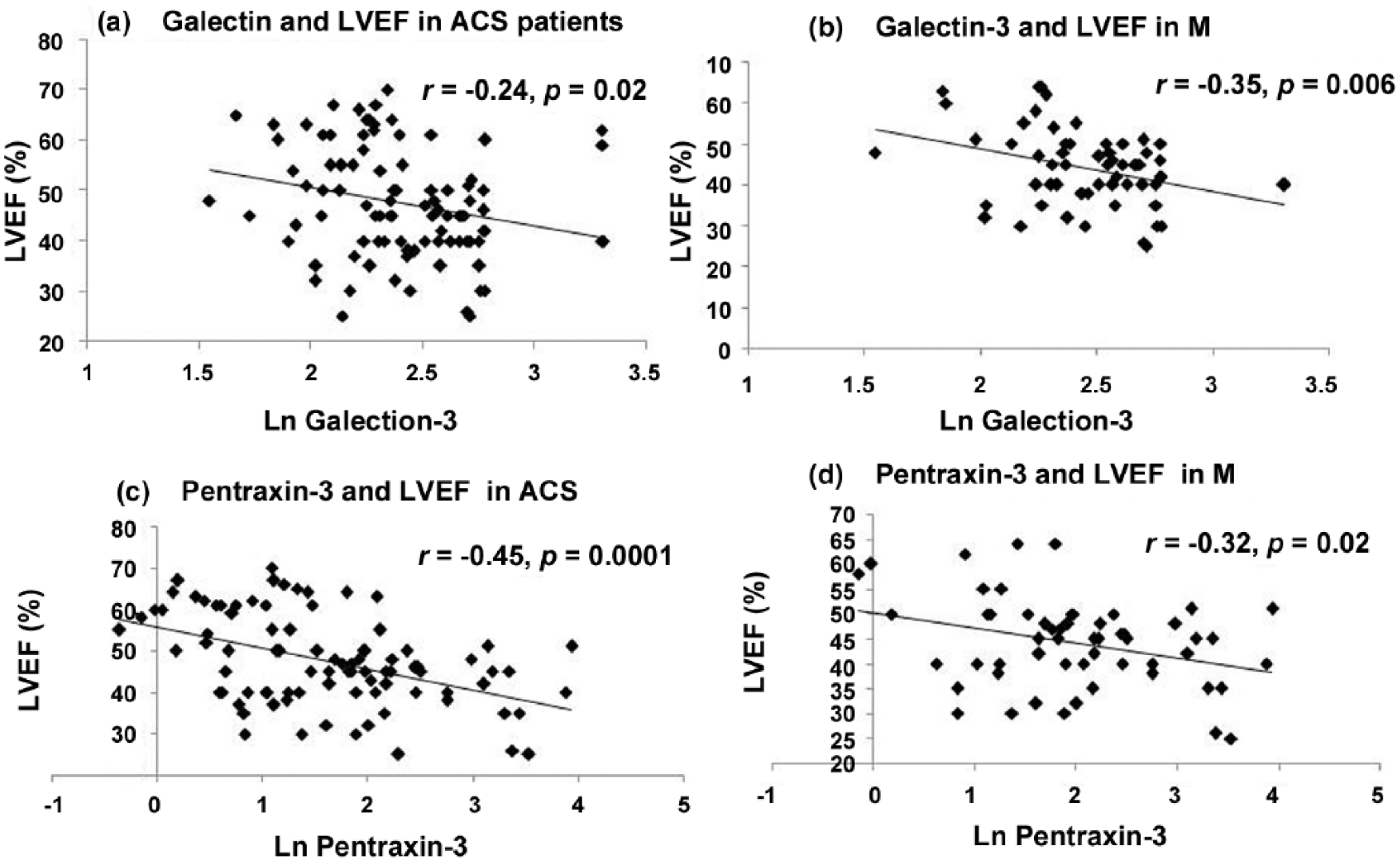
Galectin-3 and LVEF in (a) ACS patients and (b) MI patients. Pentraxin-3 and LVEF in (a) ACS patients and (b) MI patients.
Galectin-3 and eGFR
When the ACS cohort was divided based on galectin-3 levels, a significant difference was observed between the two groups, with the group with higher galectin-3 level having a significantly lower eGFR. eGFR was negatively associated with galectin-3, showing a moderate but significant correlation when analysed in the cohort of ACS patients (r = -0.2881. p < 0.005) (Figure 2).

Galectin-3 and eGFR in ACS patients.
Events
In our study, we defined higher levels of biomarker as concentrations greater than the optimal cutoff value derived from the ROC curve (Figure 3a,b). A total of 24 events occurred during the study, with 17 events occurring in ACS patients. Among the patients that experienced ST-ACS, four of them died, five underwent CABG surgery and three were rehospitalized. Among the non ST-ACS patients, five were rehospitalized for CABG surgery. The four patients that died had higher levels of both pentraxin-3 and galectin-3. It was observed that LVEF was significantly lower and that BMI was higher in those patients who experienced events Table 3.
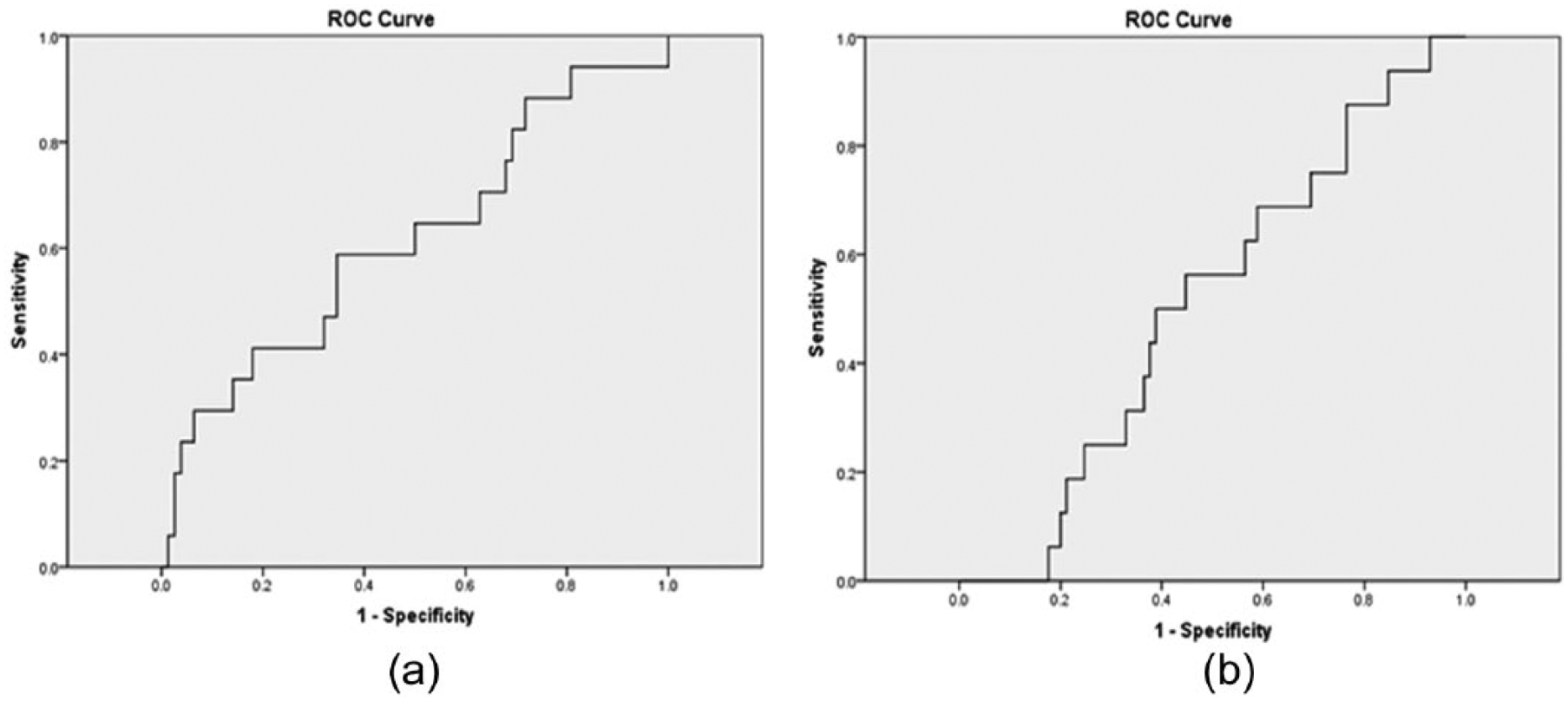
Receiver operating characteristics (ROC) for baseline (a) pentraxin-3 and (b) galectin-3 in prediction of adverse events at 6 months.
Comparison of ACS patient characteristics based on event status.
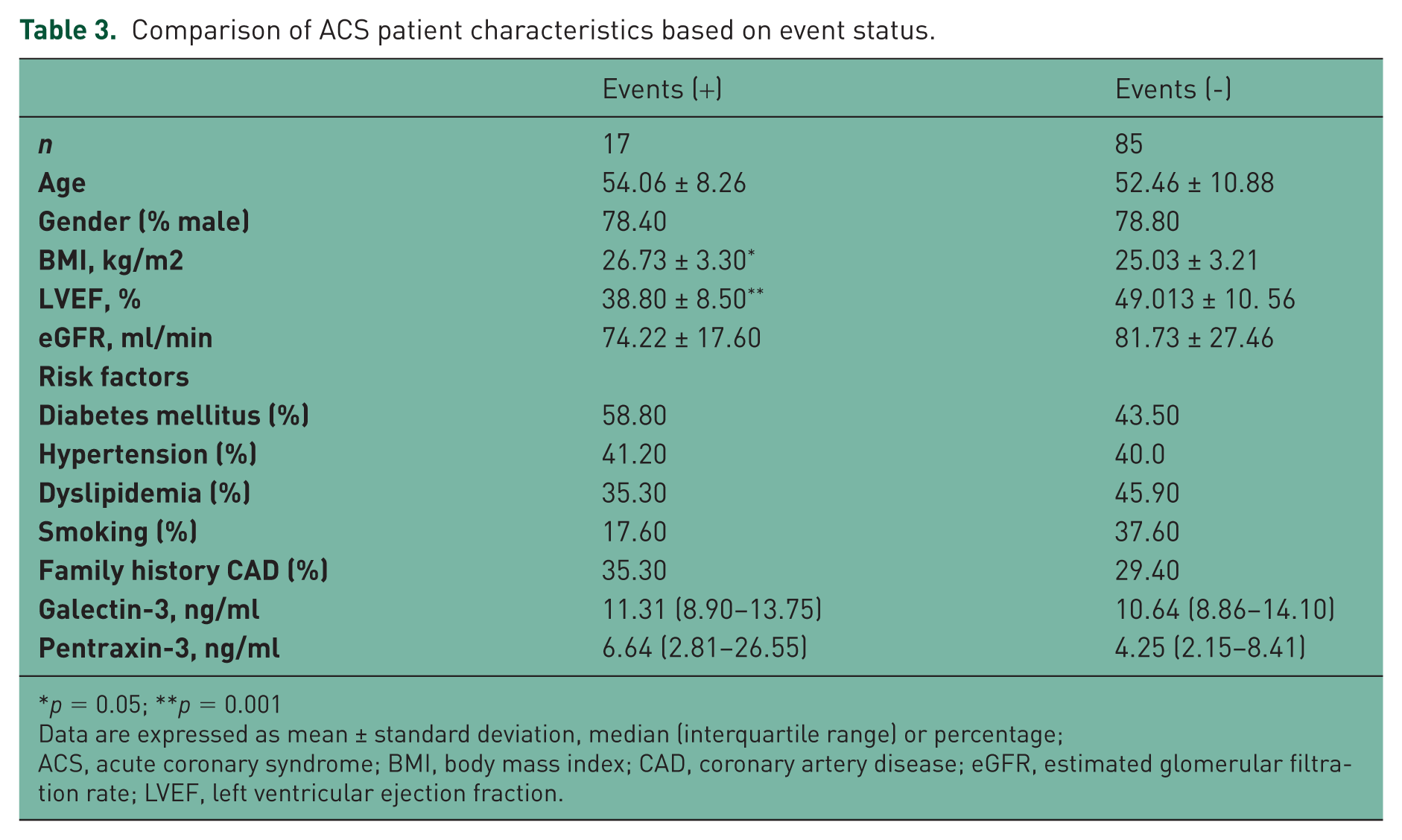
p = 0.05; **p = 0.001
Data are expressed as mean ± standard deviation, median (interquartile range) or percentage;
ACS, acute coronary syndrome; BMI, body mass index; CAD, coronary artery disease; eGFR, estimated glomerular filtration rate; LVEF, left ventricular ejection fraction.
Discussion
To the best of our knowledge, this is the first prospective study conducted in Indian populations which evaluates the levels of pentraxin-3 and galectin-3 in ACS. Our study demonstrated that the median concentrations of the biomarkers pentraxin-3 and galectin-3 were significantly higher in the MI population and that the cohort with biomarker levels greater than the cutoff derived from ROC had greater number of deaths, thus indicating that their measurement may be suitable indicators of poor prognosis.
Earlier studies in HF populations suggest that higher levels of pentraxin-3 and galectin-3 are indicative of advanced disease progression and reduced response to therapy. In our study performed in ACS populations we found that pentraxin-3 levels were significantly higher in the STEMI population compared with NSTEMI/controls. The median pentraxin-3 concentration observed in our study was comparable with other studies in the ACS population [Matsui et al.2010; Lee et al. 2010]. Galectin-3 was significantly higher in the STEMI patients than in the control population and these findings concurred with that of Tsai and colleagues [Tsai et al. 2012]. Although most studies report levels greater than those reported in our study, comparable concentrations have also been reported [Milting et al. 2008; Van Kimmenade et al. 2008].
When patients in the ACS cohort were divided based on their pentraxin levels, it was found that a greater number of events occurred in the cohort with pentraxin levels greater than cutoff derived from ROC (6.45 ng/ml). The STEMI patients that died had elevated levels of pentraxin-3 measured within 48 hours before acute event. While the role of the inflammatory biomarker pentraxin-3 in atherosclerosis is still unclear, studies do suggest that pentraxin levels are higher in ACS populations. After an acute event, a study reported that the expression of pentraxin-3 increased over time in patients with AMI, and peaked at 7.5 hours post AMI and returns to normal levels after 3 days [Peri et al. 2000]. We collected samples from our patients within 48 hours of the acute event, and the raised concentration of pentraxin-3 may reflect the triggered inflammatory process during myocardial infarction. CRP and pentraxin-3 belong to the same family of proteins. An earlier study found that CRP was markedly elevated in STEMI patients compared with NSTEMI patients [Habib et al. 2011] and the level of CRP was hypothesized to reflect the degree of intracoronary thrombosis[Arroyo-Espliguero et al. 2004; Zairis et al. 2005; Zouridakis et al. 2004].
It was also observed that LVEF, diabetic and hypertension status significantly differed between the two groups divided based on pentraxin-3 levels. A greater percentage of patients with higher levels of pentraxin were found to be hypertensive, diabetic and having a lower LVEF. Another study also found that a significantly large number of hypertensive patients had high pentraxin levels [Matsui et al. 2010]. Hypertension and diabetes are low-grade inflammatory processes and the release of pentraxin suggests the occurrence of vascular inflammatory processes. An observational study found pentraxin-3 to be 15 times the normal limit of the upper range in newly diagnosed hypertensive patients. As suggested by Parlak and colleagues, vascular inflammation could link hypertension to atherosclerotic process driving cardiovascular disorders [Parlak et al. 2012]. A direct association between insulin resistance and pentraxin-3 has been found in other populations. However, to the best of our knowledge, this has not been documented in ACS populations.
Furthermore, when we explored the relationship between LVEF and pentraxin-3, we found a significant moderate correlation between the two in ACS populations. However, we found a weak but significant correlation between LVEF and pentraxin-3 in the MI subcohort. To the best of our knowledge, the association between LVEF and pentraxin-3 has not yet been studied in the ACS populations. However, Matsubara and colleagues observed that there is no association between LVEF and pentraxin in HF population [Matsubara et al. 2011]. We found that the eGFR did not emerge to be significantly different between the groups with high and low pentraxin-3 levels. Furthermore, no correlation was observed between the two variables in ACS populations. However, in a cohort of NSTEMI patients from the GUSTO-IV study, multiple linear regression analysis found a significant association between eGFR and pentraxin-3 [Eggers et al. 2013]. A study by Kanbay and colleagues found that pentraxin-3 levels was associated with CAD risk in stage II and III chronic kidney disease (CKD) patients [Kanbay et al. 2011]
In our study, when ACS patients that experienced events were divided based on galectin levels (cutoff based on ROC: 11.02 ng/ml), a greater number of people died at 6 months in the group with galectin levels greater than cutoff. In fact, all patients who died had STEMI at the time of admission, and elevated galectin-3 levels when measured within 48 hours of the acute event. In the PRIDE study, galectin-3 levels were higher in HF than non-HF patients; 29% of the acute heart failure (AHF) patients experienced recurrent HF, while 8% of them died. Based on the sensitivity and specificity of galectin-3, the authors defined a cutoff of 9.58 (ng/ml) to predict 60-day mortality [Van Kimmenade et al. 2006]. Galectin-3 has also been implicated in inflammatory processes [Sharma et al. 2004; De Boer et al. 2010] and it is possible that the raised levels indicate the inflammation that occurs during atherosclerosis. However, it is also possible that its raised levels may reflect the initiation of a cascade of events resulting in fibrosis.
We further looked into other factors that may be influenced by galectin-3 levels and we found that LVEF was significantly lower in the cohort with high galectin-3 levels. Also, in our study we found that the cohort with higher galectin-3 levels had a lower LVEF and observed a greater number of events. Furthermore, galectin-3 and LVEF showed a weak correlation in the ACS cohort and in the MI subcohort. Similar findings were observed by Weir and colleagues where baseline galectin-3 levels negatively correlated with 24-week LVEF [Weir et al. 2013]. In a community study by Motiwala and colleagues, higher baseline galectin-3 predicted a decrease in LVEF with an odds ratio (OR) = 8.11 (p = 0.02) [Motiwala et al. 2013]. However, studies such as the ones by Mayr and colleagues and Szadkowska and colleagues found no correlation between LVEF and galectin-3, although we should note that both these studies were performed in post percutaneous coronary intervention (PCI0 patients. Therefore, there is a need to perform more studies to assess this relationship, and the role of galectin-3 as a fibrosis marker [Mayr et al. 2013; Szadkowska et al. 2013].
We found a significant moderate correlation between eGFR and galectin-3. The cohort of patients with high galectin-3 levels had significantly lower eGFR. Such an association has also been found by Anand and colleagues in whose study 20% variability in baseline galectin-3 levels could be attributed to the strong association between galectin-3 and eGFR [Anand et al. 2013]. Gopal and colleagues found that plasma galectin-3 levels were 2 fold higher in HF patients with eGFR <30 ml/min than in normal controls [Gopal et al. 2012]. Meijers and colleagues observed that, while plasma galectin-3 levels were significantly higher, fractional galectin-3 excretion was lower in HF patients compared with healthy controls. The authors speculate that the high plasma levels of galectin-3 could be due to the impaired renal clearance of the biomarker in HF patients. Mechanistic studies that may serve to disentangle the seemingly complicated biochemistry behind the role of galectin along the cardio renal axis may serve as an important tool to reduce disease burden [Meijers et al. 2014].
Pentraxin-3 is a biomarker of the CRP family, sharing 98% identity with tumour necrosis factor (TNF) stimulated gene 14 [Breviario et al. 1992; Lee et al. 1994]. Endothelial cells, macrophages, myeloid cells and dendritic cells produce PTX3 upon stimulation by cytokines and endotoxins such as interleukin 1 (IL-1) and TNF. Several studies have examined the role of pentraxin-3 in CVD, and studies conducted in mice suggest that the plasma levels of the biomarker may increase as a protective mechanism against cardiac tissue damage. Exogenous pentraxin-3 has been shown to reverse the phenotypes of increased inflammatory response characterized by increased neutrophil infiltration and apoptotic cardiomyocytes in pentraxin-3 knockout mice induced with AMI by coronary artery litigation [Inoue et al. 2012; Salio et al. 2008]. Maugeri and colleagues showed that lowest PTX3 expression was found in early MI (< 6 hours) and the released PTX3 was found to aggregate with platelets thereby inhibiting their prothombotic and proinflammatory activity, and possibly illustrating its cardioprotective activity[Maugeri et al. 2011]. Galectin-3, however, belongs to the evolutionary conserved family of the soluble β-galactoside binding lectin, which are expressed in macrophages, neutrophils, mast cells, fibroblasts and osteoclasts. The lectin is found in the nucleus, cytosol and extracellular space, where it plays numerous roles as a mediator of pre mRNA splicing in the nucleus, as a factor inhibiting apoptosis, controlling survival, regulating exocytosis in the cytosol, and exhibiting numerous autocrine and paracrine properties [Dagher et al. 1995; Hughes, 2001; Sato and Hughes, 1994] While galectin-3 has not been found in cardiomyocytes, it is found in high levels in cardiac fibroblasts. Animal model studies by Sharma and colleagues showed that rat models that progressed to HF expressed high levels of galectin-3, and the infusion of galectin-3 in the pericardium of rats induced myocardial collagen deposition and remodeling. These effects were reversed by the antifibrotic peptide, N-acetyl-seryl-aspartyl-lysyl-proline [Sharma et al. 2004].
A number of studies have thus investigated the role of galectin-3 as a diagnostic and prognostic marker for cardiovascular diseases. Considering that the disparate pathways through which pentraxin-3 and galectin-3 operate, we found a weak correlation between the two biomarkers in our study.
Limitations
While our study contributes to the growing wealth of evidence on cardiovascular biomarkers in ACS, it is not without limitations. Since the sample size was small, the number of events observed in our study was comparatively low. Logistical reasons prevented us from performing a more intense follow up of patients during the 6-month period. While a control population of healthy adults would have been ideal, we used patients with MVA and CSA as controls. We have also not accounted for the influence of drug therapies on biomarker levels and other procedures such as PCI on the event rate.
Conclusion
Pentraxin-3 and galectin-3 are novel circulatory biomarkers found to be elevated in cardiovascular diseases. In our study, we found that patients with ACS had higher levels of these biomarkers. Patients with elevated levels of these biomarkers experienced higher number of deaths and had a lower mean LVEF. Furthermore, there is a dearth of studies investigating the role of pentraxin-3 in ACS and this area calls for more research. Finally, determining the role of pentraxin-3 and galectin-3 in ACS patients is worth investigating using larger populations.
Footnotes
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.
Funding
We thank the Office of the Honorable Pro Vice Chancellor of SRM Medical College Hospital, Kattankulathur, Kancheepuram, for funding the study.