
Abstract
Objective
Contrast-induced nephropathy (CIN) is a serious complication in patients with acute coronary syndrome (ACS) and percutaneous coronary intervention (PCI). This study aimed to analyze the potential risk factors for CIN in patients undergoing PCI.
Methods
Patients with ACS who underwent PCI treatment from January 2017 to January 2020 were selected. The patients’ characteristics and medical information were collected and compared.
Results
A total of 1331 patients undergoing PCI were included. The incidence of CIN was 15.33%. Logistic regression analyses showed that a left ventricular ejection fraction ≤45% (odds ratio [OR] 4.18, 95% confidence interval [CI] 1.10–7.36), serum creatinine levels ≤60 μmol/L (OR 3.03, 95% CI 1.21–5.57), age ≥65 years (OR 2.75, 95% CI 1.32–4.60), log N-terminal pro-B-type natriuretic peptide levels ≥2.5 pg/mL (OR 2.31, 95% CI 1.18–5.13), uric acid levels ≥350 μmol/L (OR 2.29, 95% CI 1.04–5.30), emergency percutaneous intervention (OR 1.35, 95% CI 0.34–3.12), and triglyceride levels ≤1.30 mmol/L (OR 1.10, 95% CI 0.01–2.27) were independent risk factors for CIN in patients who underwent PCI.
Conclusions
Early prevention is required to reduce the occurrence of CIN in patients who undergo PCI and have risk factors for CIN.
Keywords
Background
Acute coronary syndrome (ACS) is a type of acute and severe disease of the cardiovascular system. Percutaneous coronary intervention (PCI) is an important approach for the definitive diagnosis and revascularization of patients with ACS.1,2 In patients undergoing PCI, contrast-induced nephropathy (CIN) has become a serious complication and it is closely related to clinical adverse events, such as an increased incidence of renal failure and increased short- and long-term mortality rates.3,4 CIN refers to an increase in serum creatinine levels by 25% or an increase in the absolute value by more than 44.2 μmol/L after application of a contrast agent. 5 CIN has become a common cause of hospital-acquired kidney damage. 6 The clinical symptoms of CIN are usually relatively mild or there is no obvious discomfort, which is easy for clinicians to miss. 7 However, CIN is associated with a prolonged hospital stay and increased incidence of adverse renal and cardiovascular events, and it even seriously threatens the patient’s prognosis and life. 8 Currently, there is no effective treatment for CIN. 9 Therefore, early detection and prevention of CIN are essential for prognosis of patients undergoing PCI.
Previous studies10,11 have shown that patients with ACS have a high incidence of CIN, and this incidence is three times higher than that in other groups. Moreover, diabetes and renal dysfunction can increase the incidence of CIN to 50%. 12 Studies 13 have shown that the incidence of CIN in patients with normal or slightly increased creatinine levels before surgery can be up to 13.9% after PCI. Additionally, the mortality rate of patients with CIN is significantly increased, and other clinical adverse events, such as renal replacement therapy and recurrent myocardial infarction, are also significantly increased after PCI. 14 At present, there is insufficient medical evidence for treatment of CIN. The potential risk factors for CIN need to be identified in patients undergoing PCI to provide evidence for managing these patients. Therefore, this study aimed to analyze the potential risk factors for CIN in patients undergoing PCI.
Methods
Ethical considerations
This present study was approved by the ethical committee of Yan’an University Affiliated Hospital (No. 20161008062). Written informed consent was obtained from all of the participants.
Patients
Patients with ACS who underwent PCI treatment in our hospital from January 2017 to January 2020 were selected as potential participants. The inclusion criteria were as follows: adult patients aged ≥18 years; patients who underwent primary PCI; and patients who agreed to participate in the present study. The exclusion criteria were as follows: patients with severe heart insufficiency (New York Heart Association class ≥III), renal insufficiency (glomerular filtration rate ≤20 mL/minute, serum creatinine levels ≥442 µmol/L), kidney transplantation, dialysis, abnormal thyroid function; patients who had taken drugs that might affect kidney function; and patients who did not agree to participate in this study.
All patients were divided into the CIN and non-CIN groups on the basis of whether they had a CIN attack. The diagnosis of CIN was based on the following definition of the European Association of Genitourinary Radiology: 15 nephropathy occurred after injection of iodine hypotonic contrast agent within 3 days, and other causes were excluded, serum creatinine levels increased by 44.2 μmol/L or were 25% higher than the baseline value, and creatinine levels were detected every day for 3 days.
Data collection
Two authors retrospectively collected data and any discrepancy was solved by further discussion. In all patients, serum creatinine, uric acid, and N-terminal pro-B-type natriuretic peptide (NT-proBNP) levels were measured at 24 hours after surgery. Baseline indicators, laboratory test results, surgical procedures, and major adverse cardiovascular events (including recurrent angina and myocardial infarction, cardiogenic shock, death) were recoded accordingly. Recurrent angina and myocardial infarction were defined as recurrently squeezing pain in the precordial area, and they were confirmed by further coronary angiography. Cardiogenic shock was defined as systolic blood pressure <90 mmHg, fluid resuscitation was difficult to control, and there was clinical and laboratory evidence of end-organ dysfunction (cardiac index per square meter ≤2.2 L/minute and lung capillary wedge pressure ≥15 mmHg). Emergency PCI refers to urgent PCI in our study.
PCI for all patients was performed by experienced clinical interventional cardiologists using standard techniques. Preoperatively, 0.1% lidocaine was used for local anesthesia. The contrast agent used was hypotonic iopromide (containing 370 mg iodine/mL; Dmile, Shanghai, China), with a dosage of 5 mL × weight (kg)/creatinine (mg/dL). The intraoperative heparin dosage was 60 U/kg, and platelet glycoprotein III receptor antagonists were administered as appropriate to maintain the activated coagulation time at 200 to 250 s.
The left ventricular ejection fraction (LVEF) was measured using an ACUSON X180 ultrasound diagnostic system (Daxin Company, Nanjing, China). NT-proBNP levels were measured with a fully automatic fluorescent immunoassay analyzer (Nizper; Linux, Shanghai, China). Laboratory analyses were conducted by using the Mingxes 200 automatic biochemical analyzer (Minhua, Beijing, China).
Statistical analysis
Data analyses were conducted using IBM SPSS version 23.0 statistical software (IBM Corp., Armonk, NY, USA). The characteristics of the patients between the two groups were analyzed and compared. Continuous variables were compared by the t test and categorical variables were compared by the chi-square test. Potential candidate variables were those with p<0.01 in univariate analyses. We constructed a receiver operating curve and used Youden’s index to calculate the cutoff value. Multivariate regression analyses were performed using the forward likelihood ratio selection method to identify independent factors. Odds ratios (ORs) and 95% confidence intervals (95% CIs) are presented. We used the stepwise regression method to check multicollinearity. Principal component methods were conducted to check the interaction between variables in multivariable analysis. Comparisons were considered statistically different if p was <0.05.
Results
Characteristics of the patients
A total of 1331 patients undergoing PCI were included in whom 204 had an attack of CIN. The incidence of CIN in patients with PCI was 15.33%. Age was significantly older and the rate of cases of emergency PCI was significantly higher in patients in the CIN group than in the non-CIN group (both p<0.05, Table 1). There were no significant differences in sex, weight, body mass index, smoking status, past medical history, number of stents uses, staged PCI and contrast dosage, angiotensin-converting enzyme inhibitor, angiotensin receptor blocker, and statin treatment, and the estimated glomerular filtration rate between the groups.
Characteristics of the included patients.

Data are mean ± standard deviation or n (%).
CIN, contrast-induced nephropathy; PCI, percutaneous intervention; ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; eGFR, estimated glomerular filtration rate.
Comparison of laboratory indices
Log NT-proBNP and uric acid levels were significantly higher, and triglyceride levels and the LVEF were significantly lower in patients in the CIN group than in those in the non-CIN group (all p<0.05, Table 2). There were no significant differences in levels of urea nitrogen, blood glucose, glycated hemoglobin, hemoglobin, albumin, total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, potassium, and sodium, the glomerular filtration rate, the platelet count, and the white blood cell count between the two groups.
Comparison of laboratory indices between the two groups.
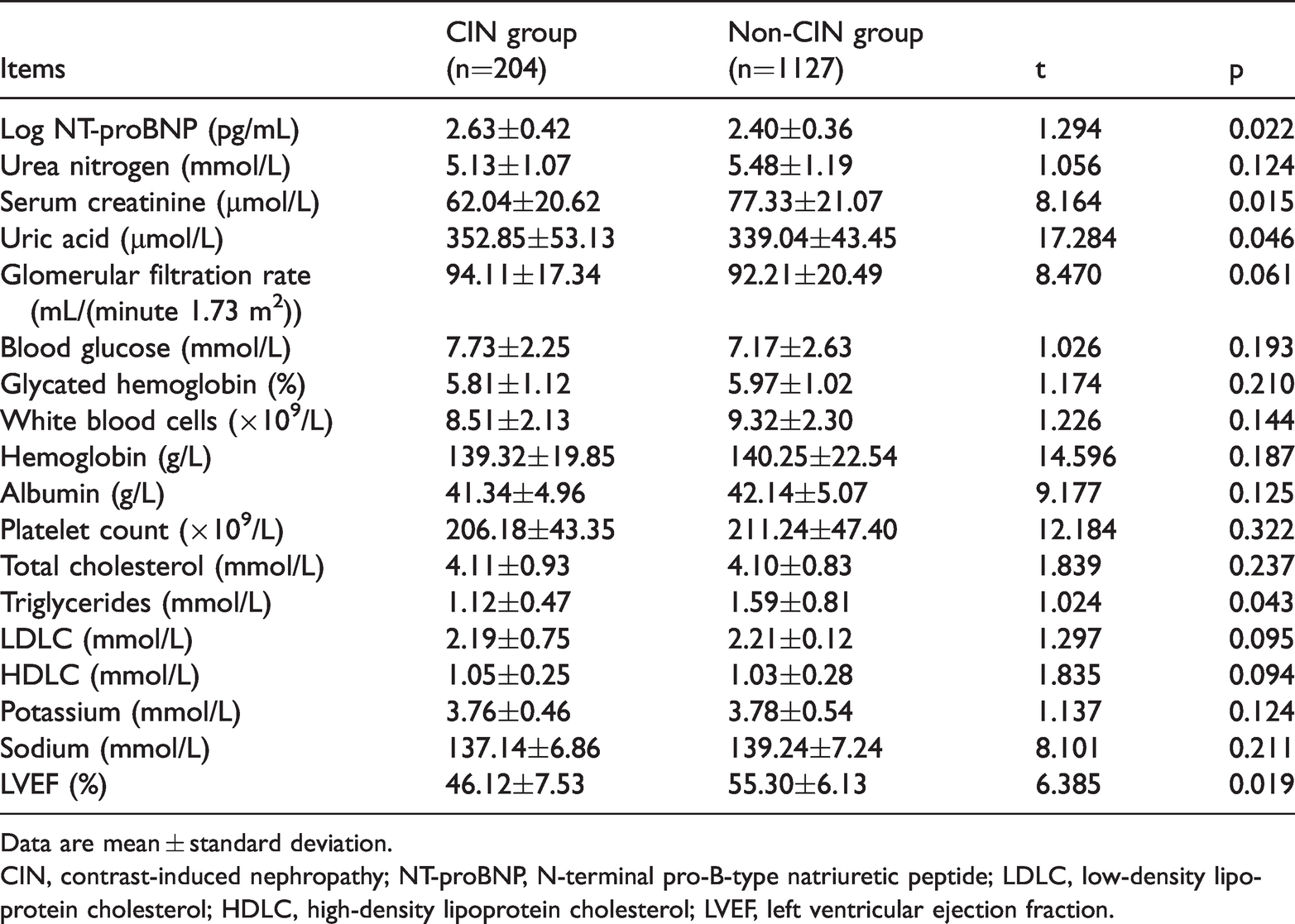
Data are mean ± standard deviation.
CIN, contrast-induced nephropathy; NT-proBNP, N-terminal pro-B-type natriuretic peptide; LDLC, low-density lipoprotein cholesterol; HDLC, high-density lipoprotein cholesterol; LVEF, left ventricular ejection fraction.
Comparison of adverse cardiovascular events
There was a significantly higher incidence of heart failure and cardiogenic shock in the CIN group than in the non-CIN group (both p<0.05, Table 3). There were no significant differences in the rates of arrhythmia, secondary angina, and death between the two groups.
Comparison of adverse cardiovascular events between the two groups.

CIN, contrast-induced nephropathy.
Logistic regression analyses
We found that an LVEF ≤45% (OR 4.18, 95% CI 1.10–7.36), serum creatinine levels ≤60 μmol/L (OR 3.03, 95% CI 1.21–5.57), age ≥65 years (OR 2.75, 95% CI 1.32–4.60), log NT-proBNP levels ≥2.5 pg/mL (OR 2.31, 95% CI 1.18–5.13), uric acid levels ≥350 μmol/L (OR 2.29, 95% CI 1.04–5.30), emergency PCI (OR 1.35, 95% CI 0.34–3.12), and triglyceride levels ≤1.30 mmol/L (OR 1.10, 95% CI 0.01–2.27) were independent risk factors for CIN in patients who underwent PCI (Table 4).
Logistic regression analyses on the risk factors for CIN in patients with PCI.

CIN, contrast-induced nephropathy; PCI, percutaneous intervention; SE, standard error; OR, odds ratio; CI, confidence interval; LVEF, left ventricular ejection fraction; NT-proBNP, N-terminal pro-B-type natriuretic peptide.
Discussion
The incidence of CIN in the general population ranges from 0.3% to 2.6%.16,17 The incidence of CIN is significantly increased in high-risk people with multiple risk factors, especially in patients with diabetes with renal insufficiency (up to 50%).18,19 A previous report 20 showed that the incidence of CIN in 510 patients after PCI was 14.5%. Our study showed that the incidence of CIN in patients with PCI was 15.33%. This finding suggests that CIN has a higher incidence after PCI and more attention needs to be paid to this condition. Furthermore, we found that an LVEF ≤45%, serum creatinine levels ≤60 μmol/L, age ≥65 years, log NT-proBNP levels ≥2.5 pg/mL, uric acid levels ≥350 μmol/L, emergency PCI, and triglyceride levels ≤1.30 mmol/L were independent risk factors for CIN in patients who underwent PCI. Patients with those factors are at risk for CIN after PCI and early intervention is required for prophylaxis of CIN.
CIN is a serious complication after PCI. Studies21–23 have shown that patients with ACS have hemodynamic instability, activation of the neuroendocrine system, and a strong inflammatory response. After application of a contrast agent, the contrast agent induces endothelin, adenosine, and angiotensin secretion through its viscosity, osmotic pressure, and ionic properties. 24 Increased secretion of nitric oxide and prostacyclin leads to contraction of infiltrating blood vessels, and ischemia and hypoxia of the renal medulla. 25 This increased secretion also directly damages the renal tubules, stimulates production of reactive oxygen species in the kidneys, and causes increased oxidative stress and lipid peroxidation of the biofilm, eventually leading to CIN. Even if coronary revascularization is successful, occurrence of CIN is a sign of short-term and long-term poor prognosis. 26 The mortality rate within 2 years in patients on dialysis with CIN can be up to 40%. 27 Therefore, early detection and prophylaxis is vital to the prognosis of patients with CIN.
Currently identified risk factors for CIN include renal insufficiency, older age, cardiac insufficiency, diabetes, and a large amount of contrast agent use. 28 Renal function is usually evaluated by the glomerular filtration rate. However, the glomerular filtration rate is susceptible to various factors, such as age, sex, body mass, and diet. With an increase in the patient’s age, the renal unit progressively decreases and the glomerular filtration rate gradually decreases, which leads to poor compensatory function of renal reserve in older patients.29,30 Therefore, a large amount of contrast agent is often required for PCI treatment. 31 Additionally, some studies32–34 have shown that cardiac insufficiency can activate the renin–angiotensin system, causing changes in endocrine factors, such as an increase in the vasoconstrictor endothelin and a decrease in the vasodilator prostaglandin. This results in an imbalance in renal vasoconstriction, finally leading to occurrence of CIN. Mehran et al. 35 studied 8357 patients and found that the incidence of CIN was 13.1% in the development set and 13.9% in the validation set (stages of CIN). They also found that hypotension, intra-aortic balloon pump placement, congestive heart failure, chronic kidney disease, diabetes, age ≥75 years, anemia, and total volume of contrast were independent predictors of CIN. There was also a strong association between an increased risk score and development of CIN. Some of our results are consistent with Mehran et al.’s 35 findings, which provide further clarification on the risk factors of CIN after PCI.
Elevated NT-proBNP levels are an independent risk factor for CIN. NT-proBNP is a cardiac and renal neurohumoral signal, which is secreted by ventricular myocytes and excreted by the kidneys.36,37 Myocardial cells in patients with ACS are severely ischemic and hypoxic, and some myocardial cells are necrotic, which stimulates ventricular myocytes to secrete NT-proBNP. 38 High oxidative stress and inflammation and an immune response stimulate release of NT-proBNP, causing its level to significantly increase. 39 Higher NT-proBNP levels induce renal vasodilation, decrease renal blood flow, and lead to medullary ischemia and hypoxia by inhibiting sympathetic nerves, dilating blood vessels, and diuresis, which result in CIN.40,41 Previous studies42,43 have also shown that NT-proBNP is a risk factor for CIN in patients with ACS, which is consistent with our findings. Emergency PCI is an independent risk factor of CIN and may be related to the situation where patients who undergo emergency PCI lack preoperative preparations, such as corrected renal function. Therefore, these patients may have a higher risk of CIN. This possibility needs to be verified in future studies.
There are several limitations to the present study. Contrast agents can be divided into hypotonic, isotonic, and hypertonic on the basis of osmotic pressure. The osmotic pressure of a hypotonic contrast agent is approximately two to three times lower than that of plasma, and the osmotic pressure of a hypertonic contrast is approximately five to seven times that of plasma. 44 Previous studies45,46 have shown that hypertonic contrast agents are significantly more toxic to the kidneys than the other two types of contrast agents. However, there are still differences in the effects of isotonic and hypotonic contrast agents on CIN. A possible limitation is that we only used hypotonic contrast agents in the present study. However, some studies have reported that isotonic contrast agents are better than hypotonic contrast agents. 47 Future studies on the role of osmotic pressure in CIN are warranted. Another limitation is that not all of the patients in the present study received hydration therapy. Therefore, we could not include this factor in data analysis. Because hydration is the most effective way to prevent CIN, application of hydration may directly affect the incidence of CIN. Therefore, hydration analysis should be added in future studies. Moreover, because of limited resources, we did not conduct long-term follow-up for the patients’ prognosis. Finally, we excluded the patients who had severe renal insufficiency. Chronic kidney disease, particularly secondary to diabetes, is an independent risk factor of CIN. Additionally, mild renal insufficiency secondary to diabetes and factors, such as kidney and renal artery stenosis, should be considered. Therefore, patients with severe renal insufficiency who have PCI should be studied in the future.
Conclusions
Our findings suggest that special attention should be paid to patients with an LVEF ≤45%, serum creatinine levels ≤60 μmol/L, age ≥65 years, log NT-proBNP levels ≥2.5 pg/mL, uric acid levels ≥350 μmol/L, emergency PCI, and triglyceride levels ≤1.30 mmol/L, which are risk factors for CIN. Early intervention is required for these patients for prophylaxis of CIN. However, this study was a retrospective, single-center study, and C-reactive protein is not regularly detected to reflect systemic inflammation. 48 Therefore, studies with a larger sample size and more objective outcome analysis are required in the future to make more reliable conclusions and provide insight into the management of PCI.
Footnotes
Availability of data and materials
All data generated or analyzed during this study are included in this article.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author contributions
JW and CZ designed the study; JW and YB conducted the research; JW and ZL analyzed the data; JW and CZ wrote the first draft of the manuscript; and YB had primary responsibility for the final content. All authors read and approved the final manuscript.